Download as ppt, pdf, or txt
You might also like
- MCQs in PediatricsDocument4 pagesMCQs in Pediatricsarun babu94% (17)
- Lung Collapse: A Review: Dr. Girish Kukade Radiology Department, AFHDocument61 pagesLung Collapse: A Review: Dr. Girish Kukade Radiology Department, AFHkukadegirishNo ratings yet
- Doppler UltrasoundDocument3 pagesDoppler UltrasoundDrShagufta IqbalNo ratings yet
- Acute Respiratory Distress SyndromeDocument43 pagesAcute Respiratory Distress SyndromeAgnes Pritama Fahmi100% (1)
- Arterial Blood Gas Analysis PDFDocument2 pagesArterial Blood Gas Analysis PDFJim Jose Antony100% (3)
- Approach To Interstitial Lung Disease 1Document33 pagesApproach To Interstitial Lung Disease 1MichaelNo ratings yet
- General ExaminationDocument112 pagesGeneral ExaminationChiranjeevi Kumar EndukuruNo ratings yet
- Restrictive Lung DiseasesDocument31 pagesRestrictive Lung DiseasesAnn FrancisNo ratings yet
- MED - Interstitial Lung Disease, Final Sept08Document91 pagesMED - Interstitial Lung Disease, Final Sept08api-3856051100% (3)
- Interstitial Lung Disease Slide ShareDocument18 pagesInterstitial Lung Disease Slide ShareEmma E. Vincent100% (1)
- Bronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandBronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Respiratory Failure (1) .Document36 pagesRespiratory Failure (1) .Ibrahim HemdanNo ratings yet
- Interstitial Lung DiseaseDocument145 pagesInterstitial Lung DiseaseMaduka SanjeewaNo ratings yet
- COPD Lecture Slides For BlackBoardDocument52 pagesCOPD Lecture Slides For BlackBoardClayton JensenNo ratings yet
- Lung Abscess Handout PDFDocument3 pagesLung Abscess Handout PDFTansanee MalivalayaNo ratings yet
- Shock: Classification and PathophysiologyDocument15 pagesShock: Classification and PathophysiologyAishwaray KohliNo ratings yet
- Respiratory ExaminationDocument20 pagesRespiratory ExaminationAmirul SyafizNo ratings yet
- CVS ExaminationDocument72 pagesCVS ExaminationPrashanthBhatNo ratings yet
- COPD HarrisonsDocument45 pagesCOPD HarrisonsNogra CarlNo ratings yet
- CopdDocument35 pagesCopdNurhidayahNo ratings yet
- How To Read A Chest X RayDocument11 pagesHow To Read A Chest X RayHilmia Fahma100% (2)
- Acid Base BalanceDocument3 pagesAcid Base BalanceHussein QasimNo ratings yet
- Lung AbsesDocument48 pagesLung AbsesAvhindAvhindNo ratings yet
- Respiratory Best RDocument5 pagesRespiratory Best RfrabziNo ratings yet
- Exam Name Exam ID: 56 - Pass Mark: 59: يـــنادوـسلا يـــبـطلا ســلجـملا Sudan Medical CouncilDocument91 pagesExam Name Exam ID: 56 - Pass Mark: 59: يـــنادوـسلا يـــبـطلا ســلجـملا Sudan Medical CouncilMoamen HellisNo ratings yet
- Chest X RayDocument61 pagesChest X RayP Vinod Kumar100% (1)
- Chest Xray 2Document39 pagesChest Xray 2sushma shresthaNo ratings yet
- How Long Do Partial Thickness Burns Typically Take To Heal?Document49 pagesHow Long Do Partial Thickness Burns Typically Take To Heal?Farah FarahNo ratings yet
- Acute Coronary SyndromeDocument21 pagesAcute Coronary SyndromeNabil Mosharraf Hossain100% (2)
- Spirometry in PracticeDocument24 pagesSpirometry in Practiceuser_at_scribd100% (1)
- Resp Bronch N LaDocument56 pagesResp Bronch N LaMansi GandhiNo ratings yet
- Empyema Thoracis: Ain Najwa BT Abd Rahim (090100457) MARDHIAH BT MARZUKI (090100470)Document22 pagesEmpyema Thoracis: Ain Najwa BT Abd Rahim (090100457) MARDHIAH BT MARZUKI (090100470)Dumora FatmaNo ratings yet
- Inguinal Hernia: Shohreh Toutounchi Reference: Schwartz Principles of Surgery 2010 Internship: 1391Document29 pagesInguinal Hernia: Shohreh Toutounchi Reference: Schwartz Principles of Surgery 2010 Internship: 1391Ritz CelsoNo ratings yet
- Medical Surgical Nursing Suretech College of NursingDocument18 pagesMedical Surgical Nursing Suretech College of NursingSanket TelangNo ratings yet
- Examination of Respiratory SystemDocument78 pagesExamination of Respiratory Systemwidya sri hastutiNo ratings yet
- Approach To Septic ShockDocument16 pagesApproach To Septic ShockRaja EllysyaNo ratings yet
- Respiratorydisease 170426125838Document69 pagesRespiratorydisease 170426125838Hayder MaqsadNo ratings yet
- Chest Pain: Sumit Bose, MD PGY-3Document55 pagesChest Pain: Sumit Bose, MD PGY-3Irfan100% (1)
- 4 - Pulmonary PathophysiologyDocument56 pages4 - Pulmonary PathophysiologyReynandriel100% (1)
- COPDDocument73 pagesCOPDBroken Oreos100% (1)
- BRONCHOSDocument21 pagesBRONCHOSMarivic Diano0% (1)
- Endotracheal IntubationDocument43 pagesEndotracheal IntubationBishow100% (2)
- Examination of The Respiratory SystemDocument2 pagesExamination of The Respiratory Systemkenners100% (17)
- Respiratory Failure in Children PDFDocument47 pagesRespiratory Failure in Children PDFOxana TurcuNo ratings yet
- Pulmonary: Ftplectures Pulmonary System Lecture NotesDocument34 pagesPulmonary: Ftplectures Pulmonary System Lecture NotesArif Setyawan100% (1)
- Tracheostomy CareDocument15 pagesTracheostomy CareZabeth ZabNo ratings yet
- On Emergency DrugsDocument25 pagesOn Emergency DrugsBikram Chhetry100% (1)
- Interstitial Lung Diseases (ILD)Document17 pagesInterstitial Lung Diseases (ILD)Rashed ShatnawiNo ratings yet
- EmpyemaDocument27 pagesEmpyemaMadyline VictoryaNo ratings yet
- Oxygen TherapyDocument25 pagesOxygen Therapypolosan123No ratings yet
- Respiratory Emergencies: Amy Bullock Amy - Bullock@students - Plymouth.ac - UkDocument34 pagesRespiratory Emergencies: Amy Bullock Amy - Bullock@students - Plymouth.ac - UkThea BerteaNo ratings yet
- Managing Mechanical VentilationDocument7 pagesManaging Mechanical VentilationArden QuiambaoNo ratings yet
- Lung AbscessDocument27 pagesLung AbscessMalueth Angui100% (1)
- Interstitial Lung DiseaseDocument77 pagesInterstitial Lung DiseaseMahaveer S ShekhawatNo ratings yet
- Intercollegiate Surgical Curriculum ENTDocument98 pagesIntercollegiate Surgical Curriculum ENTMendhi Ashish AnilNo ratings yet
- Chest X Ray BasicsDocument99 pagesChest X Ray BasicsHarshaWakodkarNo ratings yet
- Pulmonary Edema: (Acute Heart Failure)Document7 pagesPulmonary Edema: (Acute Heart Failure)james garcia100% (5)
- Case Discussion - CopdDocument63 pagesCase Discussion - CopdrajeshNo ratings yet
- Basic Principles of Mechanical VentilationDocument34 pagesBasic Principles of Mechanical VentilationMohamed KorieshNo ratings yet
- Congenital Heart Diseases, A Simple Guide to these Medical ConditionsFrom EverandCongenital Heart Diseases, A Simple Guide to these Medical ConditionsNo ratings yet
- 002 Assesment For Cough and Difficult BreathingDocument36 pages002 Assesment For Cough and Difficult BreathingSuhazeli AbdullahNo ratings yet
- Pulmonology: The Cells of The Bronchial Epithelium, LeucocytesDocument64 pagesPulmonology: The Cells of The Bronchial Epithelium, LeucocytesSk Chaudhry100% (1)
- Daftar PustakaDocument4 pagesDaftar PustakaAnisa OktavianiNo ratings yet
- Respiratory PathologyDocument42 pagesRespiratory PathologyMorgan PeggNo ratings yet
- B2 - A - Cystic FibrosisDocument1 pageB2 - A - Cystic FibrosisfaisalNo ratings yet
- Signs and Symptoms of Respiratory DiseasesDocument42 pagesSigns and Symptoms of Respiratory DiseasesjabeedNo ratings yet
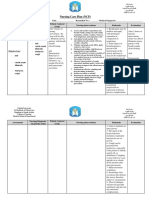
- 3 NCP Form (1) (5) .Docareway NoorDocument3 pages3 NCP Form (1) (5) .Docareway NoorALI-A ALINo ratings yet
- Hamman Rich SyndromeDocument7 pagesHamman Rich SyndromeGerardo Armando EsparzaNo ratings yet
- Shortness of BreathDocument3 pagesShortness of Breathamani abduNo ratings yet
- Asthma Patho CF UgDocument26 pagesAsthma Patho CF Ugtnandanwar91No ratings yet
- Spanish Flu: Jump To Navigation Jump To Search The Great InfluenzaDocument3 pagesSpanish Flu: Jump To Navigation Jump To Search The Great InfluenzaMattNo ratings yet
- Lovely Agromedicine Bagus Pratama 32Document74 pagesLovely Agromedicine Bagus Pratama 32Dandy Fahsi AlgifaryNo ratings yet
- Part B 33 Pandemic FluDocument6 pagesPart B 33 Pandemic FluLeah ValenciaNo ratings yet
- Definition of PneumoniaDocument4 pagesDefinition of PneumoniaEmylia Ananda PutriNo ratings yet
- Byssinosis in IndiaDocument4 pagesByssinosis in IndiaKessi VikaneswariNo ratings yet
- Healthcare-Associated Pneumonia (HCAP)Document20 pagesHealthcare-Associated Pneumonia (HCAP)mcvirgo014No ratings yet
- Test Your Knowledge About Pneumonia - ProProfs QuizDocument8 pagesTest Your Knowledge About Pneumonia - ProProfs QuizNaresh Kumar SoniNo ratings yet
- Chestgra、 Ph Hl-101: Spirometry SystemDocument2 pagesChestgra、 Ph Hl-101: Spirometry SystemDiep NguyentuanNo ratings yet
- 10 Respiratory System 2Document120 pages10 Respiratory System 2rosalyn gaboniNo ratings yet
- Etiopathogenesis of CroupDocument9 pagesEtiopathogenesis of CroupHarshith NaniNo ratings yet
- Hospitalazacao Por VSRDocument12 pagesHospitalazacao Por VSRnelcitojuniorNo ratings yet
- Bronkitis 2Document12 pagesBronkitis 2Lucky PuspitasariNo ratings yet
- L23 - Pneumonia MedDocument51 pagesL23 - Pneumonia MedAL-ashai MohammedNo ratings yet
- Management of InfluenzaDocument14 pagesManagement of Influenzajaish8904No ratings yet
- BronchitisDocument4 pagesBronchitisGokul SmartNo ratings yet
- Acute CoughDocument5 pagesAcute CoughSundar RamanathanNo ratings yet
- Sakit NovDocument126 pagesSakit NovArda SenjayaNo ratings yet
- Algorithm Immunisation Status Jan2020Document1 pageAlgorithm Immunisation Status Jan2020Afsan BulbulNo ratings yet
- Chronic Lower Respiratory Tract InfectionsDocument32 pagesChronic Lower Respiratory Tract Infectionsibnbasheer100% (2)