Download as pdf or txt
You might also like
- Head-to-Toe Assessment Checklist: Department of Nursing Health AssessmentDocument2 pagesHead-to-Toe Assessment Checklist: Department of Nursing Health AssessmentRachel Ray100% (3)
- Skills Checklist-Critical CareDocument3 pagesSkills Checklist-Critical CareRom Anog100% (4)
- Exam 1 (NUR-152)Document5 pagesExam 1 (NUR-152)davidvpnNo ratings yet
- Neurological ChecklistDocument2 pagesNeurological ChecklistAshley100% (1)
- Interactive Code Blue Evaluation FormDocument2 pagesInteractive Code Blue Evaluation FormAyman Ali100% (1)
- Bachelor of Dental Surgery Clinical LogbookDocument69 pagesBachelor of Dental Surgery Clinical Logbookkachy892075% (4)
- Code Blue Form - SKHDocument2 pagesCode Blue Form - SKHRaviraj Pishe89% (9)
- Preop ChecklistDocument2 pagesPreop ChecklistJan Federick BantayNo ratings yet
- Triage ESI Practice QuestionsDocument6 pagesTriage ESI Practice QuestionsSusan Harden50% (2)
- Assessment Leadership Community Health 4 1Document14 pagesAssessment Leadership Community Health 4 1Royal Shop100% (1)
- Preoperative Checklist-1Document10 pagesPreoperative Checklist-1June Faith HacheroNo ratings yet
- Sample Form of Quality Assurance Nursing AuditDocument2 pagesSample Form of Quality Assurance Nursing AuditgandhialpitNo ratings yet
- Care of Ventilated PatientsDocument2 pagesCare of Ventilated PatientsRaydan Francis Magana Antojado100% (1)
- Post Anaesthesia Recovery ScoreDocument2 pagesPost Anaesthesia Recovery ScoreRaviraj Pishe50% (2)
- I. Preoperative Assessment 1. Physical: Philippine Heart Center Perioperative Nursing RecordDocument2 pagesI. Preoperative Assessment 1. Physical: Philippine Heart Center Perioperative Nursing RecordERWINNo ratings yet
- Nursing Health Assessment Practice QuestionsDocument22 pagesNursing Health Assessment Practice QuestionsSraddha PatelNo ratings yet
- Discharge Plan FormatDocument2 pagesDischarge Plan FormatChristian67% (6)
- Registration FormDocument5 pagesRegistration FormSreejith Kelakam100% (1)
- Pretest IV TherapyDocument3 pagesPretest IV TherapyMeranda Martin0% (2)
- Black Ink 7:00 Am To 10:59 PMDocument2 pagesBlack Ink 7:00 Am To 10:59 PMjongmartinezNo ratings yet
- IDCAP Clinical Assessment ToolsDocument4 pagesIDCAP Clinical Assessment ToolsIDCAP2011100% (1)
- AORN Comprehensive Surgical Checklist 2016Document1 pageAORN Comprehensive Surgical Checklist 2016Firma WahyuNo ratings yet
- Surgical Safety ChecklistDocument1 pageSurgical Safety ChecklistАндрій ДанильцівNo ratings yet
- Perioperative Nursing (1) 2007Document14 pagesPerioperative Nursing (1) 2007Lorraine BuelvaNo ratings yet
- NABH Staff RatioDocument1 pageNABH Staff RatioRetteri KUMARANNo ratings yet
- National Core Competency StandardsDocument89 pagesNational Core Competency Standardsverna100% (1)
- Preoperative ChecklistDocument1 pagePreoperative ChecklistRyrey Abraham Pacamana100% (1)
- Board Questions 2009Document16 pagesBoard Questions 2009Erick EspinoNo ratings yet
- Pain Care PlanDocument18 pagesPain Care Planjordanw0613No ratings yet
- Best Practice Statement AuditDocument2 pagesBest Practice Statement Auditns officeNo ratings yet
- IV Therapy ChecklistDocument3 pagesIV Therapy ChecklistJestoni SalvadorNo ratings yet
- START / Jump START Triage: ImmediateDocument2 pagesSTART / Jump START Triage: ImmediateJerome DanielNo ratings yet
- Pre Op ChecklistDocument1 pagePre Op ChecklistKoushik Reddy PodduturiNo ratings yet
- Surgery 1 - UCDocument101 pagesSurgery 1 - UCEsvinch EsvinchNo ratings yet
- Code Blue EvaluationDocument1 pageCode Blue EvaluationJessica Garlets0% (1)
- Community Health Nursing - Nclex QuestionsDocument13 pagesCommunity Health Nursing - Nclex QuestionsJESLINE ANTONYNo ratings yet
- Schmid Fall Risk Assessment Tool - Acute CareDocument2 pagesSchmid Fall Risk Assessment Tool - Acute CareMark Avellanosa50% (2)
- Patient A KARDEX 1Document2 pagesPatient A KARDEX 1Franz Patrick Legria, CPAC - SNNo ratings yet
- ASSISTING IN A MAJOR OPERATION Circulating Nurse Performance EvaluationDocument2 pagesASSISTING IN A MAJOR OPERATION Circulating Nurse Performance EvaluationKrizzia Angela BacotocNo ratings yet
- L&D C-Section Care PlanDocument12 pagesL&D C-Section Care PlanGina Giammalvo100% (2)
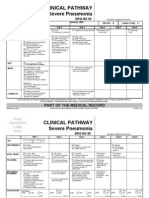
- Clinical Pathways Severe PneumoniaDocument2 pagesClinical Pathways Severe PneumoniaaandakuNo ratings yet
- IV and GCS ChecklistDocument2 pagesIV and GCS ChecklistEricka Shayne Andaya100% (2)
- Sample Charting orDocument1 pageSample Charting orKatherine Ibarra100% (1)
- Morse Fall Risk Assessment ToolDocument2 pagesMorse Fall Risk Assessment ToolDinar Chieko100% (1)
- Roth 10e Nclex Chapter 10Document4 pagesRoth 10e Nclex Chapter 10jennaaahhhNo ratings yet
- Outline Perioperative NursingDocument8 pagesOutline Perioperative NursingMM VNo ratings yet
- Operating Room Nurse Interview QuestionsDocument2 pagesOperating Room Nurse Interview Questionsali aliNo ratings yet
- Hospital Daily Census ReportDocument1 pageHospital Daily Census ReportGerald TalledoNo ratings yet
- Calculating For Staffing Needs PDFDocument11 pagesCalculating For Staffing Needs PDFkcharmaigneNo ratings yet
- IVTDocument11 pagesIVTNoorwashilaNo ratings yet
- Orientation Program For New Nurses in Emergency DepartmentDocument38 pagesOrientation Program For New Nurses in Emergency DepartmentNers SenNo ratings yet
- Nursing Audit ToolDocument2 pagesNursing Audit Toolalaysa udok100% (2)
- 107 CalculationsDocument3 pages107 CalculationsAna Tabanao100% (1)
- Fundamentals of Nursing1Document4 pagesFundamentals of Nursing1TEre DemegilioNo ratings yet
- Case PresentationDocument2 pagesCase Presentationalalrashidi1No ratings yet
- ContentServer CompletoDocument42 pagesContentServer CompletoLaura CandeiasNo ratings yet
- Izazovi U Menadzmentu Snabdevanja Lekovima Indija - SHAMIMA TAYOB FINAL EXAMDocument221 pagesIzazovi U Menadzmentu Snabdevanja Lekovima Indija - SHAMIMA TAYOB FINAL EXAMHokusyNo ratings yet
- BioMedical Waste AuditDocument1 pageBioMedical Waste AuditPrabhat Kumar0% (2)
- Clinical Review October 20 2017 - SHINGRIXDocument158 pagesClinical Review October 20 2017 - SHINGRIXPayneMaxNo ratings yet
- Colorful Modern Hello August Instagram Story-5Document1 pageColorful Modern Hello August Instagram Story-5Althea Carla AndayaNo ratings yet