Download as pdf or txt
You might also like
- An Atlas of Neonatal Brain Sonography, 2nd EditionFrom EverandAn Atlas of Neonatal Brain Sonography, 2nd EditionRating: 5 out of 5 stars5/5 (6)
- Beginners Guide To Blackwork by Lesley Wilkins2 PDFDocument63 pagesBeginners Guide To Blackwork by Lesley Wilkins2 PDFSCP100% (4)
- Cae Writing GuideDocument60 pagesCae Writing Guideelisadp95% (20)
- Disrafismo Spinal OcultaDocument4 pagesDisrafismo Spinal OcultaCarlos CalderwoodNo ratings yet
- Thomas 2011Document16 pagesThomas 2011varunraj362196No ratings yet
- Corpus Callosotomy With Disconnection SyndromeDocument8 pagesCorpus Callosotomy With Disconnection SyndromeRavi ChandraNo ratings yet
- Embryonal Remnants in The Testis and EpididymisDocument9 pagesEmbryonal Remnants in The Testis and EpididymisKata TölgyesiNo ratings yet
- Clinical Imaging: Jared Narvid, Jason F. Talbott, Christine M. GlastonburyDocument10 pagesClinical Imaging: Jared Narvid, Jason F. Talbott, Christine M. GlastonburyIrina TurcanuNo ratings yet
- Referral of Diagnosis and Management of Erb-Duchenne PalsyDocument22 pagesReferral of Diagnosis and Management of Erb-Duchenne PalsyAshielaNo ratings yet
- Boroumand 2016Document3 pagesBoroumand 2016Winston FontesNo ratings yet
- Incidental Reportzaharopoulos2000Document4 pagesIncidental Reportzaharopoulos2000maglangitmarvincNo ratings yet
- Congenital LaryngomalaciaDocument8 pagesCongenital LaryngomalaciaRettha SigiroNo ratings yet
- The Pathophysiology of Thoracic Disc DiseaseDocument6 pagesThe Pathophysiology of Thoracic Disc Diseasehoneyjane100% (1)
- Anatomy of LymphaticsDocument16 pagesAnatomy of LymphaticsmenafabNo ratings yet
- Acb 49 213Document4 pagesAcb 49 213Haru SahaNo ratings yet
- Papillary Carcinoma 7-2Document4 pagesPapillary Carcinoma 7-2Amna MurtaxaNo ratings yet
- Dayyani 2018Document3 pagesDayyani 2018Oswaldo MascareñasNo ratings yet
- Folliculosebaceous Cystic Hamartoma Associated With Melanocytic NevusDocument3 pagesFolliculosebaceous Cystic Hamartoma Associated With Melanocytic NevusCata RodriguezNo ratings yet
- Chiari MalformationDocument8 pagesChiari MalformationismailakarimNo ratings yet
- Neonatal White Matter Damage and the Fetal InflammDocument6 pagesNeonatal White Matter Damage and the Fetal InflammMerlin MaelissaNo ratings yet
- Posterior Fossa Arachnoid Cysts As Findings in An Ataxia ClinicDocument8 pagesPosterior Fossa Arachnoid Cysts As Findings in An Ataxia ClinicPedroNo ratings yet
- Follicular NeoplasmaDocument12 pagesFollicular NeoplasmaoudbanadalNo ratings yet
- ThymomasDocument6 pagesThymomasAsmara SyedNo ratings yet
- Anatomy and Pathology of The Cerebellar PeduncleDocument9 pagesAnatomy and Pathology of The Cerebellar PeduncleJulius Dominique L. AnjaoNo ratings yet
- Lymphatic Malformation (Cystic Hygroma)Document12 pagesLymphatic Malformation (Cystic Hygroma)afrisiammyNo ratings yet
- Excision of Branchial Cleft CystsDocument10 pagesExcision of Branchial Cleft Cystssjs315No ratings yet
- GGL Pelvis DelimitareDocument12 pagesGGL Pelvis DelimitareStefan AnaNo ratings yet
- NeurosurgicalDocument5 pagesNeurosurgicalErwin WibowoNo ratings yet
- 97488-Article Text-254532-1-10-20131122Document2 pages97488-Article Text-254532-1-10-20131122aaliagaqNo ratings yet
- Immunofluroscerence RenalDocument28 pagesImmunofluroscerence Renalchiluka87No ratings yet
- Imaging Features of Covid-19 Associated Rhino-Orbito-Cerebral Mucormycosis - A Review of Current Updates of Black FungusDocument11 pagesImaging Features of Covid-19 Associated Rhino-Orbito-Cerebral Mucormycosis - A Review of Current Updates of Black Fungusindex PubNo ratings yet
- Review Article: Splenic Anomalies of Shape, Size, and Location: Pictorial EssayDocument10 pagesReview Article: Splenic Anomalies of Shape, Size, and Location: Pictorial EssayyurikepratiwiNo ratings yet
- In Focus: Clinical Imaging of The Median Arcuate Ligament Through Cadaveric ExplorationDocument3 pagesIn Focus: Clinical Imaging of The Median Arcuate Ligament Through Cadaveric Explorationeditorial.boardNo ratings yet
- Splina Functii PDFDocument11 pagesSplina Functii PDFTotolici StefanNo ratings yet
- Wrist Ganglion Cysts - Radsource PDFDocument1 pageWrist Ganglion Cysts - Radsource PDFKhalid Al maneiNo ratings yet
- Lymphatic Malformations Diagnosis and ManagementDocument8 pagesLymphatic Malformations Diagnosis and ManagementMutiara KantikaNo ratings yet
- The Vermiform Appendix: AnatomyDocument10 pagesThe Vermiform Appendix: AnatomyBereket temesgenNo ratings yet
- Papular Nevus Spilus SyndromeDocument4 pagesPapular Nevus Spilus SyndromePedroNo ratings yet
- Cystic Lesions of The Brain A Classification Based On PathogenesisDocument16 pagesCystic Lesions of The Brain A Classification Based On Pathogenesisveerraju tvNo ratings yet
- Premidterm ObjectivesDocument16 pagesPremidterm ObjectivesDcd MurrayNo ratings yet
- Abiola Seminar in SpleenDocument23 pagesAbiola Seminar in SpleenBamgbose OpeyemiNo ratings yet
- IVU Changes in TBDocument8 pagesIVU Changes in TBBrendan DiasNo ratings yet
- Bilateral Nasolabial Cyst MarcoviceanuDocument4 pagesBilateral Nasolabial Cyst MarcoviceanubamsusiloNo ratings yet
- Review of The Major and Minor Salivary Glands, Part 1 - Anatomy, Infectious, and Inflammatory ProcessesDocument8 pagesReview of The Major and Minor Salivary Glands, Part 1 - Anatomy, Infectious, and Inflammatory ProcessesPao AlexaNo ratings yet
- Tumors of The Brain Stem, Cerebellum, and Fourth VentricleDocument22 pagesTumors of The Brain Stem, Cerebellum, and Fourth VentricleArjun RaNo ratings yet
- Clinical Imaging: Michela Gabelloni, Lorenzo Faggioni, Sandra Accogli, Giacomo Aringhieri, Emanuele NeriDocument12 pagesClinical Imaging: Michela Gabelloni, Lorenzo Faggioni, Sandra Accogli, Giacomo Aringhieri, Emanuele NeriJavier Araya CancinoNo ratings yet
- Bailey 5th Ed Cerebellopontine Angle TumorDocument33 pagesBailey 5th Ed Cerebellopontine Angle TumorOkky IrawanNo ratings yet
- Chapter I-V-1-Anatomy-Dr-Mark-MakaryDocument17 pagesChapter I-V-1-Anatomy-Dr-Mark-MakaryMark MakaryNo ratings yet
- Javt 14 I 2 P 86Document5 pagesJavt 14 I 2 P 86Bhayu RizallinoorNo ratings yet
- Short Case 9Document192 pagesShort Case 9Dr Gurunandini AcharNo ratings yet
- Electrodiagnosis of Cervical RadiculopathyDocument12 pagesElectrodiagnosis of Cervical RadiculopathywutariNo ratings yet
- Constriction Band SyndromeDocument8 pagesConstriction Band SyndromesabistonNo ratings yet
- Epidemiology: AssociationsDocument6 pagesEpidemiology: AssociationsFrendy YangNo ratings yet
- Anatomia InglesDocument12 pagesAnatomia InglesGerson SantosNo ratings yet
- 2006 A Suprarenal Mass in A Child. Pulmonary Sequestration. EJPDocument3 pages2006 A Suprarenal Mass in A Child. Pulmonary Sequestration. EJPJoseloNo ratings yet
- MECKELDocument9 pagesMECKELjuan.riosNo ratings yet
- International Journal of Surgery Case Reports: Case Report - Open AccessDocument3 pagesInternational Journal of Surgery Case Reports: Case Report - Open AccesscagcmdNo ratings yet
- Epidemiology and Pathology of Intraventricular TumorsDocument14 pagesEpidemiology and Pathology of Intraventricular TumorsNaim CalilNo ratings yet
- Interpretation of Chest RadiographDocument7 pagesInterpretation of Chest RadiographhengkileonardNo ratings yet
- Cleft Lip and Palate Management: A Comprehensive AtlasFrom EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunNo ratings yet
- Jadual Waktu Kelas PKPP PDFDocument18 pagesJadual Waktu Kelas PKPP PDFAidda SuriNo ratings yet
- Cape Sewing - Industrial Sewing TechnologyDocument33 pagesCape Sewing - Industrial Sewing TechnologyMonika GadgilNo ratings yet
- Aremonte Barnett - Beowulf Notetaking GuideDocument4 pagesAremonte Barnett - Beowulf Notetaking Guideapi-550410922No ratings yet
- B.SC Fashion Design R2018 C&SDocument85 pagesB.SC Fashion Design R2018 C&SvivekNo ratings yet
- Adjustment LetterDocument14 pagesAdjustment LetterQadr IftikharNo ratings yet
- Landslides Causes EffectsDocument9 pagesLandslides Causes EffectsDaljeet SidhuNo ratings yet
- The National Policy On Education (1981) : Problems of Implementation and The Way ForwardDocument8 pagesThe National Policy On Education (1981) : Problems of Implementation and The Way ForwardSaidu abuNo ratings yet
- Deloitte Part-2 Task-2Document5 pagesDeloitte Part-2 Task-2Nelikondi RakeshNo ratings yet
- Indian Api Industry - Reaching The Full Potential: AprilDocument88 pagesIndian Api Industry - Reaching The Full Potential: AprilStevin GeorgeNo ratings yet
- Lpo Birds NestDocument6 pagesLpo Birds Nestapi-265791946No ratings yet
- Ch-8 Challeges To DemocracyDocument2 pagesCh-8 Challeges To DemocracySujitnkbpsNo ratings yet
- Complete Each Sentence by Choosing The Correct Form:: Ell The Children To Tidy Their RoomDocument4 pagesComplete Each Sentence by Choosing The Correct Form:: Ell The Children To Tidy Their RoomIvana Slavevska-MarkovskaNo ratings yet
- SCHOOL YEAR 2017 - 2018: 1. Informational DataDocument8 pagesSCHOOL YEAR 2017 - 2018: 1. Informational Datadamyan_salazarNo ratings yet
- Katarungang Pambarangay: By: Angelo S. Mahinay Enhanced By: Mlgoo Fidel M. NarismaDocument138 pagesKatarungang Pambarangay: By: Angelo S. Mahinay Enhanced By: Mlgoo Fidel M. NarismaMelvs NavarraNo ratings yet
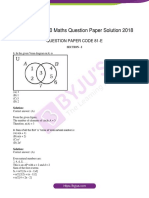
- Kseeb Class 10 Maths Question Paper Solution 2018Document23 pagesKseeb Class 10 Maths Question Paper Solution 2018Raghav L NaikNo ratings yet
- Assignment/ Tugasan - Introductory Employment LawDocument9 pagesAssignment/ Tugasan - Introductory Employment LawShasha LovelyNo ratings yet
- Practical Class 2 Text Artificial IntelligenceDocument3 pagesPractical Class 2 Text Artificial IntelligenceAlex VaskoNo ratings yet
- Training A320 DoorsDocument216 pagesTraining A320 DoorsMUHANDES UKRAINE100% (2)
- Chapter 14 NotesDocument21 pagesChapter 14 NotesnightdazeNo ratings yet
- Summer Training Project ReportDocument94 pagesSummer Training Project Reportumeshpastor100% (1)
- MOHAN RESUME FinalDocument4 pagesMOHAN RESUME Finalyeluru mohanNo ratings yet
- English File: Answer KeyDocument4 pagesEnglish File: Answer KeyEvelyn BoccioNo ratings yet
- World History GlossaryDocument20 pagesWorld History GlossaryRana MubasherNo ratings yet
- Mendelssohn Op. 19 Nr. 1 Analyse ENDocument2 pagesMendelssohn Op. 19 Nr. 1 Analyse ENLianed SofiaNo ratings yet
- FAGL TcodesDocument3 pagesFAGL TcodesRahul100% (2)
- Secondary Research of Telecom SectorDocument3 pagesSecondary Research of Telecom SectorVikram BhadauriaNo ratings yet
- Philippine National Philippine National Philippine National Philippine National Standard Standard Standard StandardDocument14 pagesPhilippine National Philippine National Philippine National Philippine National Standard Standard Standard StandardBernard Karlo BuduanNo ratings yet
- Concept: 18 Questions Were Answered Correctly. 4 Questions Were Answered IncorrectlyDocument15 pagesConcept: 18 Questions Were Answered Correctly. 4 Questions Were Answered IncorrectlyHugsNo ratings yet