Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- APN License IllinoisDocument19 pagesAPN License IllinoisEvangelist Michelle Leavy-BreunigNo ratings yet
- Perianesthesia Nursing Core Curriculum e Book Preprocedure Phase I and Phase II Pacu Nursing Ebook PDF VersionDocument62 pagesPerianesthesia Nursing Core Curriculum e Book Preprocedure Phase I and Phase II Pacu Nursing Ebook PDF Versionronald.robotham754100% (48)
- Inventaris NewDocument6 pagesInventaris NewJogi PanggabeanNo ratings yet
- Resume Mina GhazaviDocument2 pagesResume Mina Ghazavimohammadrezahajian12191No ratings yet
- Cv-Update For DoctorDocument2 pagesCv-Update For DoctorRATANRAJ SINGHDEONo ratings yet
- Optiflow Flow Matters Edition 9 PM 619256Document4 pagesOptiflow Flow Matters Edition 9 PM 619256Thanh TrầnNo ratings yet
- Daftar Pustaka RFDocument4 pagesDaftar Pustaka RFAndanoktaviaNo ratings yet
- Opioid Free Anesthesia A Different Regard To.98965 PDFDocument6 pagesOpioid Free Anesthesia A Different Regard To.98965 PDFgabriel herrera100% (1)
- Regional Anesthesia - 3B NotesDocument5 pagesRegional Anesthesia - 3B NotesBetina HernandezNo ratings yet
- Rle NotesDocument7 pagesRle NotesLorens Troy SoltisNo ratings yet
- CPSA Hearing Tribunal Decision - Dr. Gaylord WardellDocument27 pagesCPSA Hearing Tribunal Decision - Dr. Gaylord WardellCTV CalgaryNo ratings yet
- Anesthesia in HorseDocument4 pagesAnesthesia in HorseLessana de Moura GonçalvesNo ratings yet
- Vitreo Retinal Society India 2Document44 pagesVitreo Retinal Society India 2Ramesh BabuNo ratings yet
- Alur Manajemen Nyeri Rumah SakitDocument45 pagesAlur Manajemen Nyeri Rumah SakitRadit NasillaNo ratings yet
- DR - Ajay Wahi 2019Document3 pagesDR - Ajay Wahi 2019vidya jyotiNo ratings yet
- Novada ACLS AHA 2015Document25 pagesNovada ACLS AHA 2015novada indraNo ratings yet
- Weingart Vent HandoutDocument4 pagesWeingart Vent HandoutStrept Pneumonia100% (1)
- Rss SC SpinalDocument6 pagesRss SC SpinalBhenNo ratings yet
- Anesth ThesisDocument11 pagesAnesth ThesisAkshay HariNo ratings yet
- Benefits and Risks of Dexamethasone in Noncardiac SurgeryDocument9 pagesBenefits and Risks of Dexamethasone in Noncardiac SurgeryHenry Gabriel HarderNo ratings yet
- Caesarean Section CS Pre Peri and Post Op CareDocument13 pagesCaesarean Section CS Pre Peri and Post Op CareRajni KakranNo ratings yet
- RSP New Nomenclature Ventilation Modes Icu Booklet 9066477 enDocument72 pagesRSP New Nomenclature Ventilation Modes Icu Booklet 9066477 enNasro Juv100% (1)
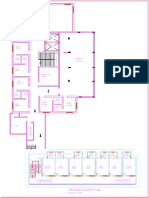
- Hospital Second FloorDocument1 pageHospital Second FloorArya M.SNo ratings yet
- Anesthesia ConsentDocument4 pagesAnesthesia ConsentvinodshsaNo ratings yet
- ANESTHESIOLOGY 2019 From A Third Year Medical Student's PerspectiveDocument10 pagesANESTHESIOLOGY 2019 From A Third Year Medical Student's PerspectiveSatyam PandeyNo ratings yet
- FAST HUGS BID: Modified Mnemonic For Surgical PatientDocument2 pagesFAST HUGS BID: Modified Mnemonic For Surgical PatientdefitranandaNo ratings yet
- Assignment / Tugasan NBNS1503 Trauma and Emergency Nursing September Semester 2021Document8 pagesAssignment / Tugasan NBNS1503 Trauma and Emergency Nursing September Semester 2021sitiNo ratings yet
- Society For Education in Anesthesia Medical Student Guide To Anesthesiology Fifth Edition 2009Document46 pagesSociety For Education in Anesthesia Medical Student Guide To Anesthesiology Fifth Edition 2009Laylee ClareNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Luka Dekubitus Akibat Penggunaan Alat Medis Di Ruang PicuDocument11 pagesFaktor-Faktor Yang Berhubungan Dengan Kejadian Luka Dekubitus Akibat Penggunaan Alat Medis Di Ruang PicuChensya SouisaNo ratings yet
- Daftar PustakaDocument7 pagesDaftar Pustakaauliana tesaNo ratings yet