Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Payroll Audit Program FinalDocument39 pagesPayroll Audit Program FinalPushkar Deodhar100% (1)
- PD Software Test Engineer PB5 v201610Document3 pagesPD Software Test Engineer PB5 v201610Deepak Manohar EkboteNo ratings yet
- Project in Math: Submitted By: Micah Lalo 9-AcaciaDocument5 pagesProject in Math: Submitted By: Micah Lalo 9-AcaciaEman LaloNo ratings yet
- Communication AssessmentDocument3 pagesCommunication Assessmentairbuk doeingNo ratings yet
- Nokia n72 rm180 Schematics PDFDocument8 pagesNokia n72 rm180 Schematics PDFAbu Hanna MariamNo ratings yet
- Tourism Marketing Syllabus 7-20Document10 pagesTourism Marketing Syllabus 7-20Joy PhotographNo ratings yet
- Curtin University - Student Timetable - My Timetable - EstudentDocument2 pagesCurtin University - Student Timetable - My Timetable - Estudentfalam0877No ratings yet
- Fortran90 TutorialDocument86 pagesFortran90 TutorialFaulwienixNo ratings yet
- Sampaio2017 PDFDocument12 pagesSampaio2017 PDFCamilo DiazNo ratings yet
- Objectives: To Study The Market Mapping of NecktiesDocument4 pagesObjectives: To Study The Market Mapping of NecktiesMahek SisodiaNo ratings yet
- Gumbel DistributionDocument6 pagesGumbel DistributionMisty BellNo ratings yet
- Full Revolution Clutch OSHA ComplianceDocument3 pagesFull Revolution Clutch OSHA ComplianceVic HernandezNo ratings yet
- Assessment 3A - Tuckman Model For Team DevelopmentDocument3 pagesAssessment 3A - Tuckman Model For Team DevelopmentkhadijjatariqNo ratings yet
- Chapter IIIDocument3 pagesChapter IIIRatu TriaNo ratings yet
- Introduction To FIRODocument5 pagesIntroduction To FIROpara guegosNo ratings yet
- The Future of WorkplaceDocument8 pagesThe Future of WorkplaceJazreel HardinNo ratings yet
- C Algorithms For Real Time DSP (1995-Scanned) - P EmbreeDocument250 pagesC Algorithms For Real Time DSP (1995-Scanned) - P EmbreeChandra SekharNo ratings yet
- FGDocument1,337 pagesFGmarlynNo ratings yet
- Interconnect Intro FPGADocument50 pagesInterconnect Intro FPGATamzidul Hoque TonmoyNo ratings yet
- 6 - Impulse-Momentum TheoremDocument11 pages6 - Impulse-Momentum Theoremfrank dumbleNo ratings yet
- Jeenspsu 02Document8 pagesJeenspsu 02Siddharth BhattNo ratings yet
- Bijan. (2005) - China's "Peaceful Rise" To Great-Power Status PDFDocument8 pagesBijan. (2005) - China's "Peaceful Rise" To Great-Power Status PDFMajoAlmeidaNo ratings yet
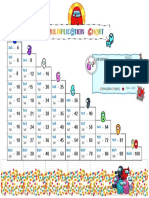
- Multiplication ChartDocument1 pageMultiplication ChartManeerat CharoennapapornNo ratings yet
- Total Station TopconDocument6 pagesTotal Station TopconRegan Tandukar100% (1)
- Use Equals Sign To Determine Missing Numbers Algebra Level 3 Worksheet - Ver - 3Document13 pagesUse Equals Sign To Determine Missing Numbers Algebra Level 3 Worksheet - Ver - 3Fatima AliuNo ratings yet
- CharaDashaPart1BW PDFDocument10 pagesCharaDashaPart1BW PDFGurpreet Kaur100% (1)
- MM7 International ManagementDocument4 pagesMM7 International ManagementRafael SotenNo ratings yet
- Bettis Cba 300 Series Pneumatic Actuators Us DataDocument6 pagesBettis Cba 300 Series Pneumatic Actuators Us DatasusantoNo ratings yet
- (Spi) Ritual OMnipotence BrochureDocument2 pages(Spi) Ritual OMnipotence BrochureOtherehtONo ratings yet
- Utilization of Waste Glass in ConcreteDocument8 pagesUtilization of Waste Glass in ConcreteSamarNo ratings yet