
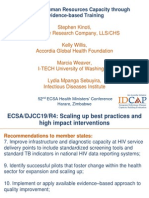
Cyprien Nioble, Jhpiego-Cote Divoire, IAS2012 Poster, MNH Quality Improvement
Cyprien Nioble, Jhpiego-Cote Divoire, IAS2012 Poster, MNH Quality Improvement
You might also like
- Nursing Informatics: Scope and Standards of PracticeFrom EverandNursing Informatics: Scope and Standards of PracticeRating: 4 out of 5 stars4/5 (6)
- Alice MonologuesDocument4 pagesAlice MonologuesLa Spera Ottava67% (3)
- Stanford Neurodiagnostics Policies Manual 2010Document241 pagesStanford Neurodiagnostics Policies Manual 2010Felipe Kanda50% (2)
- Healthcare Quality Assurance ManualDocument77 pagesHealthcare Quality Assurance ManualEvonne Tan100% (1)
- General Standards (NDT)Document2 pagesGeneral Standards (NDT)agniva dattaNo ratings yet
- Equity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiDocument34 pagesEquity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiEjemai EboreimeNo ratings yet
- ISQua Webinar - Nick Sevdalis - September 2017Document39 pagesISQua Webinar - Nick Sevdalis - September 2017utari dewiNo ratings yet
- 05b HIV Testing and Counseling (National)Document26 pages05b HIV Testing and Counseling (National)AIDSPhilNo ratings yet
- Introduction To QoC SurveysDocument8 pagesIntroduction To QoC SurveysBaleegh Al-sharabyNo ratings yet
- Nationaln Tle: National Audit of Continence Care: Laying The FoundationDocument23 pagesNationaln Tle: National Audit of Continence Care: Laying The Foundationi can always make u smile :DNo ratings yet
- DR Nabila Zaka UNICEF PresentationDocument15 pagesDR Nabila Zaka UNICEF PresentationMaternal and Child Survival Program (MCSP)No ratings yet
- Cdc-Hiv-Adherence Clubs LRC Ebi RetentionDocument4 pagesCdc-Hiv-Adherence Clubs LRC Ebi Retentiontshepoteeman05No ratings yet
- Lauren B. LittlejohnDocument16 pagesLauren B. Littlejohnapi-516216369No ratings yet
- Service & Quality, Management in Hospitals (S&QMH) : Subject Code: CC2110 Roll No: MHA19102Document26 pagesService & Quality, Management in Hospitals (S&QMH) : Subject Code: CC2110 Roll No: MHA19102Dr. Ebinesh AntonyNo ratings yet
- Quality ImprovementDocument3 pagesQuality ImprovementViky SinghNo ratings yet
- Translate AnakDocument12 pagesTranslate AnakAndikNo ratings yet
- Jurnal 1Document12 pagesJurnal 1Riafinola IfanisariNo ratings yet
- Understanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiDocument34 pagesUnderstanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiEjemai EboreimeNo ratings yet
- Philippines: Country ProfileDocument4 pagesPhilippines: Country ProfileElica Bolhano NarcisoNo ratings yet
- Key Points For Considering Adoption of The Who Labour Care Guide: Policy BriefDocument12 pagesKey Points For Considering Adoption of The Who Labour Care Guide: Policy BriefYuli AstutiNo ratings yet
- Monograph of Qi ProjectDocument29 pagesMonograph of Qi ProjectmerahiNo ratings yet
- Smart Ta Plan HB Eng FinalDocument9 pagesSmart Ta Plan HB Eng Finalapi-242232457No ratings yet
- 13 Patient Saefty and Quality ImprovementDocument36 pages13 Patient Saefty and Quality ImprovementShafiq Ur RahmanNo ratings yet
- Main Conclusions and RecommendationsDocument15 pagesMain Conclusions and RecommendationsEmeka ChrizNo ratings yet
- SOP - HIV Care Patient Follow-Up ProgrammeDocument23 pagesSOP - HIV Care Patient Follow-Up ProgrammeParwatiNo ratings yet
- Pharmacy 07 00083Document18 pagesPharmacy 07 00083alfinadyaNo ratings yet
- Hermida: Experiences Using Routine Monitoring Data For Quality Improvement of Newborn Health in EcuadorDocument14 pagesHermida: Experiences Using Routine Monitoring Data For Quality Improvement of Newborn Health in EcuadorNewborn2013No ratings yet
- Introduction To Quality Improvement Tools: Changing Processes To Improve OutcomesDocument34 pagesIntroduction To Quality Improvement Tools: Changing Processes To Improve OutcomesLibyaFlowerNo ratings yet
- Cqi ProjectDocument5 pagesCqi Projectapi-307103979No ratings yet
- Quality Standards For Urban Primary Health CentreDocument284 pagesQuality Standards For Urban Primary Health CentreGajendra TodakarNo ratings yet
- PR As Innovation in Volta RegionDocument37 pagesPR As Innovation in Volta RegionSimon DzokotoNo ratings yet
- Clinical Governance in The UK NHSDocument4 pagesClinical Governance in The UK NHSchiefsanjivNo ratings yet
- Picker Disclosure Final Report 07262011ssDocument7 pagesPicker Disclosure Final Report 07262011ssapi-283934309No ratings yet
- MBFHI Self-Assessment ToolDocument64 pagesMBFHI Self-Assessment ToolMash JumahariNo ratings yet
- R HFA Report Example RwandaDocument66 pagesR HFA Report Example RwandaOluranti SijuwolaNo ratings yet
- Corrected PicotDocument8 pagesCorrected Picotjosephmainam9No ratings yet
- NHS Framework For Clinical GovernanceDocument12 pagesNHS Framework For Clinical Governancetiara_kusumaningtyas50% (2)
- Nursing AuditDocument26 pagesNursing AuditJoe ShewaleNo ratings yet
- Enhancing Clinical Practice in The Management of Distress: The Therapeutic Practices For Distress Management (TPDM) ProjectDocument7 pagesEnhancing Clinical Practice in The Management of Distress: The Therapeutic Practices For Distress Management (TPDM) ProjectKarolinaMaślakNo ratings yet
- 409 Toward Elimination of Perinatal HIV Transmission in The USDocument31 pages409 Toward Elimination of Perinatal HIV Transmission in The USAnn KayNo ratings yet
- JCI Update 2011Document26 pagesJCI Update 2011Bayuaji SismantoNo ratings yet
- Supportive SupervisionDocument21 pagesSupportive SupervisionSaad MotawéaNo ratings yet
- AUDITDocument6 pagesAUDITJay RathvaNo ratings yet
- Quality in Health Care:: DefinitionDocument7 pagesQuality in Health Care:: DefinitionREVATHI H KNo ratings yet
- Quality Assurance in IV TherapyDocument37 pagesQuality Assurance in IV TherapyMalena Joy Ferraz VillanuevaNo ratings yet
- RCH - Reproductive and Child Health Part 1Document21 pagesRCH - Reproductive and Child Health Part 1Dr. Rakshit SolankiNo ratings yet
- How Does Program Monitoring (Reading 1 and 2) Fit Into The Schematic Diagram of The Function of Program Evaluation Given in Figure?Document5 pagesHow Does Program Monitoring (Reading 1 and 2) Fit Into The Schematic Diagram of The Function of Program Evaluation Given in Figure?Noti GelzNo ratings yet
- Attaining ISO 15189 Accreditation Through SLMTA: A Journey by Kenya's National HIV Reference LaboratoryDocument9 pagesAttaining ISO 15189 Accreditation Through SLMTA: A Journey by Kenya's National HIV Reference LaboratoryHaytham Hagrass100% (1)
- 365 880 1 SpdranizaDocument12 pages365 880 1 Spdranizareluvsa2No ratings yet
- Ket ProposalDocument37 pagesKet ProposalEneyew BirhanNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument7 pagesBest Practice & Research Clinical Obstetrics and GynaecologyEko TulusNo ratings yet
- 03 QAP Orientation For QMT Members (Davao Sur - Davao City) July 9, 2014Document68 pages03 QAP Orientation For QMT Members (Davao Sur - Davao City) July 9, 2014John Russell MoralesNo ratings yet
- A Clinician’s Guide to HCV Treatment in the Primary Care Setting: A Multimedia eHealth Source™ Educational InitiativeFrom EverandA Clinician’s Guide to HCV Treatment in the Primary Care Setting: A Multimedia eHealth Source™ Educational InitiativeNo ratings yet
- Practice Standards For Obstetric and Gynaecological UnitDocument27 pagesPractice Standards For Obstetric and Gynaecological UnitRDi J100% (1)
- Policies and Procedures CQIPDocument4 pagesPolicies and Procedures CQIPRobjun AlvarezNo ratings yet
- Improving Human Resources Capacity Through Evidence-Based TrainingDocument14 pagesImproving Human Resources Capacity Through Evidence-Based TrainingIDCAP2011No ratings yet
- Department KPIDocument21 pagesDepartment KPIAbraham EshetuNo ratings yet
- Birthing Healthy BabiesDocument13 pagesBirthing Healthy Babiesapi-234924328No ratings yet
- PBC 2012 JCI Standards To Evaluate and Improve Pediatric Oncology Nursing Care in Guatemala PDFDocument6 pagesPBC 2012 JCI Standards To Evaluate and Improve Pediatric Oncology Nursing Care in Guatemala PDFEMIGDIO1969No ratings yet
- What Is Clinical GovernanceDocument8 pagesWhat Is Clinical GovernanceApollwn100% (1)
- ASSIGNMENT PlannigDocument6 pagesASSIGNMENT Plannigprabhjot singhNo ratings yet
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsFrom EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsNo ratings yet
- Closing Remarks - Nursing Midwifery LeadershipDocument19 pagesClosing Remarks - Nursing Midwifery LeadershipJhpiegoNo ratings yet
- GE Foundation Awards Jhpiego $2.3 Million To Accelerate Global Health InnovationsDocument2 pagesGE Foundation Awards Jhpiego $2.3 Million To Accelerate Global Health InnovationsJhpiegoNo ratings yet
- Cervical Cancer Screening - JhpiegoDocument15 pagesCervical Cancer Screening - JhpiegoJhpiego100% (1)
- Seizing The Opportunity - Working With Adolescent Boys For An HIV-free Generation"Document14 pagesSeizing The Opportunity - Working With Adolescent Boys For An HIV-free Generation"JhpiegoNo ratings yet
- Spatial Mapping Results in a Successful Large-Scale Voluntary Medical Male Circumcision (VMMC) Campaign: Using GIS Data for Decision-Making Positively Impacts the VMMC Scale-Up in Iringa and Njombe Regions of TanzaniaDocument1 pageSpatial Mapping Results in a Successful Large-Scale Voluntary Medical Male Circumcision (VMMC) Campaign: Using GIS Data for Decision-Making Positively Impacts the VMMC Scale-Up in Iringa and Njombe Regions of TanzaniaJhpiegoNo ratings yet
- Community Health Workers Creating Family Planning Social Networks Through Satisified ClientsDocument15 pagesCommunity Health Workers Creating Family Planning Social Networks Through Satisified ClientsJhpiegoNo ratings yet
- Capturing A Missed Opportunity Through Postpartum Intrauterine Contraceptive Device (PPIUCD) in Ethiopia: Experience of The Maternal and Child Health Integrated Program (MCHIP)Document13 pagesCapturing A Missed Opportunity Through Postpartum Intrauterine Contraceptive Device (PPIUCD) in Ethiopia: Experience of The Maternal and Child Health Integrated Program (MCHIP)JhpiegoNo ratings yet
- Screening For Maternal Anemia: A Low-Cost Solution For A Persistent Global Health ChallengeDocument1 pageScreening For Maternal Anemia: A Low-Cost Solution For A Persistent Global Health ChallengeJhpiegoNo ratings yet
- Date/Time: Thursday, November 14, 2013 Session: 2.2.11 Family Planning and Quality of CareDocument2 pagesDate/Time: Thursday, November 14, 2013 Session: 2.2.11 Family Planning and Quality of CareJhpiegoNo ratings yet
- Improving Maternal Child Health (MCH) ServicesDocument22 pagesImproving Maternal Child Health (MCH) ServicesJhpiegoNo ratings yet
- Pre-Test - Pediatric NursingDocument6 pagesPre-Test - Pediatric NursingogiskuadzNo ratings yet
- EWRFDocument1 pageEWRFHarini Sybel CullenNo ratings yet
- 10 Sample Paper Chennai Region 2Document11 pages10 Sample Paper Chennai Region 2Illaya BharathiNo ratings yet
- Manual On Settlement of Land DisputesDocument120 pagesManual On Settlement of Land Disputescookbooks&lawbooks100% (1)
- A Level Essay Questions by TopicsDocument11 pagesA Level Essay Questions by TopicsDD97No ratings yet
- Oisd STD 235Document110 pagesOisd STD 235naved ahmed100% (5)
- M607 L01 SolutionDocument7 pagesM607 L01 SolutionRonak PatelNo ratings yet
- Analysis of Credit Risk Measurement UsinDocument6 pagesAnalysis of Credit Risk Measurement UsinDia-wiNo ratings yet
- UBX Cloud - VEEAM Cloud Backup SlickDocument2 pagesUBX Cloud - VEEAM Cloud Backup SlickmohamedalihashNo ratings yet
- Aipmt Round 3Document335 pagesAipmt Round 3AnweshaBoseNo ratings yet
- Weekly Report w34Document19 pagesWeekly Report w34Asep MAkmurNo ratings yet
- FINA3010 Assignment1Document5 pagesFINA3010 Assignment1Hei RayNo ratings yet
- LABELDocument2 pagesLABELerinNo ratings yet
- ProjectDocument3 pagesProjectKimzee kingNo ratings yet
- The Effectiveness of Bilingual Program and Policy in The Academic Performance and Engagement of StudentsDocument10 pagesThe Effectiveness of Bilingual Program and Policy in The Academic Performance and Engagement of StudentsJoshua LagonoyNo ratings yet
- Ers. Co M: JANA Master Fund, Ltd. Performance Update - December 2010 Fourth Quarter and Year in ReviewDocument10 pagesErs. Co M: JANA Master Fund, Ltd. Performance Update - December 2010 Fourth Quarter and Year in ReviewVolcaneum100% (2)
- Media Release 3665 (English) 14 08 14Document2 pagesMedia Release 3665 (English) 14 08 14ElPaisUyNo ratings yet
- emPower-API-Specification-v0 90 PDFDocument26 pagesemPower-API-Specification-v0 90 PDFPape Mignane FayeNo ratings yet
- Assessment Form: Monitoring The Functionality of City/Municipal Council For The Protection of Children (C/MCPC)Document3 pagesAssessment Form: Monitoring The Functionality of City/Municipal Council For The Protection of Children (C/MCPC)dilg libmananNo ratings yet
- Acc21 March18Document12 pagesAcc21 March18Romero Mary Jane C.No ratings yet
- Milvik ProposalDocument29 pagesMilvik ProposalMin HajNo ratings yet
- Negara Hukum-5-1-Juni-2014Document99 pagesNegara Hukum-5-1-Juni-2014haekalnashvilleNo ratings yet
- Vinayyak - CV - Sap - ExpDocument3 pagesVinayyak - CV - Sap - ExpmanikandanNo ratings yet
- Responsibility Accounting Practice ProblemDocument4 pagesResponsibility Accounting Practice ProblemBeomiNo ratings yet
- Other Hands - Issue #15-16, Supplement PDFDocument8 pagesOther Hands - Issue #15-16, Supplement PDFAlHazredNo ratings yet
- Memorial For The Appellants-Team Code L PDFDocument44 pagesMemorial For The Appellants-Team Code L PDFAbhineet KaliaNo ratings yet
- ICICI Prudential Life Insurance CompanyDocument21 pagesICICI Prudential Life Insurance CompanySayantan ChoudhuryNo ratings yet
- Theory, Culture & Society: The AestheticDocument8 pagesTheory, Culture & Society: The AestheticJaime UtrerasNo ratings yet


































































































You might also like
- Nursing Informatics: Scope and Standards of PracticeFrom EverandNursing Informatics: Scope and Standards of PracticeRating: 4 out of 5 stars4/5 (6)
- Alice MonologuesDocument4 pagesAlice MonologuesLa Spera Ottava67% (3)
- Stanford Neurodiagnostics Policies Manual 2010Document241 pagesStanford Neurodiagnostics Policies Manual 2010Felipe Kanda50% (2)
- Healthcare Quality Assurance ManualDocument77 pagesHealthcare Quality Assurance ManualEvonne Tan100% (1)
- General Standards (NDT)Document2 pagesGeneral Standards (NDT)agniva dattaNo ratings yet
- Equity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiDocument34 pagesEquity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiEjemai EboreimeNo ratings yet
- ISQua Webinar - Nick Sevdalis - September 2017Document39 pagesISQua Webinar - Nick Sevdalis - September 2017utari dewiNo ratings yet
- 05b HIV Testing and Counseling (National)Document26 pages05b HIV Testing and Counseling (National)AIDSPhilNo ratings yet
- Introduction To QoC SurveysDocument8 pagesIntroduction To QoC SurveysBaleegh Al-sharabyNo ratings yet
- Nationaln Tle: National Audit of Continence Care: Laying The FoundationDocument23 pagesNationaln Tle: National Audit of Continence Care: Laying The Foundationi can always make u smile :DNo ratings yet
- DR Nabila Zaka UNICEF PresentationDocument15 pagesDR Nabila Zaka UNICEF PresentationMaternal and Child Survival Program (MCSP)No ratings yet
- Cdc-Hiv-Adherence Clubs LRC Ebi RetentionDocument4 pagesCdc-Hiv-Adherence Clubs LRC Ebi Retentiontshepoteeman05No ratings yet
- Lauren B. LittlejohnDocument16 pagesLauren B. Littlejohnapi-516216369No ratings yet
- Service & Quality, Management in Hospitals (S&QMH) : Subject Code: CC2110 Roll No: MHA19102Document26 pagesService & Quality, Management in Hospitals (S&QMH) : Subject Code: CC2110 Roll No: MHA19102Dr. Ebinesh AntonyNo ratings yet
- Quality ImprovementDocument3 pagesQuality ImprovementViky SinghNo ratings yet
- Translate AnakDocument12 pagesTranslate AnakAndikNo ratings yet
- Jurnal 1Document12 pagesJurnal 1Riafinola IfanisariNo ratings yet
- Understanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiDocument34 pagesUnderstanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiEjemai EboreimeNo ratings yet
- Philippines: Country ProfileDocument4 pagesPhilippines: Country ProfileElica Bolhano NarcisoNo ratings yet
- Key Points For Considering Adoption of The Who Labour Care Guide: Policy BriefDocument12 pagesKey Points For Considering Adoption of The Who Labour Care Guide: Policy BriefYuli AstutiNo ratings yet
- Monograph of Qi ProjectDocument29 pagesMonograph of Qi ProjectmerahiNo ratings yet
- Smart Ta Plan HB Eng FinalDocument9 pagesSmart Ta Plan HB Eng Finalapi-242232457No ratings yet
- 13 Patient Saefty and Quality ImprovementDocument36 pages13 Patient Saefty and Quality ImprovementShafiq Ur RahmanNo ratings yet
- Main Conclusions and RecommendationsDocument15 pagesMain Conclusions and RecommendationsEmeka ChrizNo ratings yet
- SOP - HIV Care Patient Follow-Up ProgrammeDocument23 pagesSOP - HIV Care Patient Follow-Up ProgrammeParwatiNo ratings yet
- Pharmacy 07 00083Document18 pagesPharmacy 07 00083alfinadyaNo ratings yet
- Hermida: Experiences Using Routine Monitoring Data For Quality Improvement of Newborn Health in EcuadorDocument14 pagesHermida: Experiences Using Routine Monitoring Data For Quality Improvement of Newborn Health in EcuadorNewborn2013No ratings yet
- Introduction To Quality Improvement Tools: Changing Processes To Improve OutcomesDocument34 pagesIntroduction To Quality Improvement Tools: Changing Processes To Improve OutcomesLibyaFlowerNo ratings yet
- Cqi ProjectDocument5 pagesCqi Projectapi-307103979No ratings yet
- Quality Standards For Urban Primary Health CentreDocument284 pagesQuality Standards For Urban Primary Health CentreGajendra TodakarNo ratings yet
- PR As Innovation in Volta RegionDocument37 pagesPR As Innovation in Volta RegionSimon DzokotoNo ratings yet
- Clinical Governance in The UK NHSDocument4 pagesClinical Governance in The UK NHSchiefsanjivNo ratings yet
- Picker Disclosure Final Report 07262011ssDocument7 pagesPicker Disclosure Final Report 07262011ssapi-283934309No ratings yet
- MBFHI Self-Assessment ToolDocument64 pagesMBFHI Self-Assessment ToolMash JumahariNo ratings yet
- R HFA Report Example RwandaDocument66 pagesR HFA Report Example RwandaOluranti SijuwolaNo ratings yet
- Corrected PicotDocument8 pagesCorrected Picotjosephmainam9No ratings yet
- NHS Framework For Clinical GovernanceDocument12 pagesNHS Framework For Clinical Governancetiara_kusumaningtyas50% (2)
- Nursing AuditDocument26 pagesNursing AuditJoe ShewaleNo ratings yet
- Enhancing Clinical Practice in The Management of Distress: The Therapeutic Practices For Distress Management (TPDM) ProjectDocument7 pagesEnhancing Clinical Practice in The Management of Distress: The Therapeutic Practices For Distress Management (TPDM) ProjectKarolinaMaślakNo ratings yet
- 409 Toward Elimination of Perinatal HIV Transmission in The USDocument31 pages409 Toward Elimination of Perinatal HIV Transmission in The USAnn KayNo ratings yet
- JCI Update 2011Document26 pagesJCI Update 2011Bayuaji SismantoNo ratings yet
- Supportive SupervisionDocument21 pagesSupportive SupervisionSaad MotawéaNo ratings yet
- AUDITDocument6 pagesAUDITJay RathvaNo ratings yet
- Quality in Health Care:: DefinitionDocument7 pagesQuality in Health Care:: DefinitionREVATHI H KNo ratings yet
- Quality Assurance in IV TherapyDocument37 pagesQuality Assurance in IV TherapyMalena Joy Ferraz VillanuevaNo ratings yet
- RCH - Reproductive and Child Health Part 1Document21 pagesRCH - Reproductive and Child Health Part 1Dr. Rakshit SolankiNo ratings yet
- How Does Program Monitoring (Reading 1 and 2) Fit Into The Schematic Diagram of The Function of Program Evaluation Given in Figure?Document5 pagesHow Does Program Monitoring (Reading 1 and 2) Fit Into The Schematic Diagram of The Function of Program Evaluation Given in Figure?Noti GelzNo ratings yet
- Attaining ISO 15189 Accreditation Through SLMTA: A Journey by Kenya's National HIV Reference LaboratoryDocument9 pagesAttaining ISO 15189 Accreditation Through SLMTA: A Journey by Kenya's National HIV Reference LaboratoryHaytham Hagrass100% (1)
- 365 880 1 SpdranizaDocument12 pages365 880 1 Spdranizareluvsa2No ratings yet
- Ket ProposalDocument37 pagesKet ProposalEneyew BirhanNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument7 pagesBest Practice & Research Clinical Obstetrics and GynaecologyEko TulusNo ratings yet
- 03 QAP Orientation For QMT Members (Davao Sur - Davao City) July 9, 2014Document68 pages03 QAP Orientation For QMT Members (Davao Sur - Davao City) July 9, 2014John Russell MoralesNo ratings yet
- A Clinician’s Guide to HCV Treatment in the Primary Care Setting: A Multimedia eHealth Source™ Educational InitiativeFrom EverandA Clinician’s Guide to HCV Treatment in the Primary Care Setting: A Multimedia eHealth Source™ Educational InitiativeNo ratings yet
- Practice Standards For Obstetric and Gynaecological UnitDocument27 pagesPractice Standards For Obstetric and Gynaecological UnitRDi J100% (1)
- Policies and Procedures CQIPDocument4 pagesPolicies and Procedures CQIPRobjun AlvarezNo ratings yet
- Improving Human Resources Capacity Through Evidence-Based TrainingDocument14 pagesImproving Human Resources Capacity Through Evidence-Based TrainingIDCAP2011No ratings yet
- Department KPIDocument21 pagesDepartment KPIAbraham EshetuNo ratings yet
- Birthing Healthy BabiesDocument13 pagesBirthing Healthy Babiesapi-234924328No ratings yet
- PBC 2012 JCI Standards To Evaluate and Improve Pediatric Oncology Nursing Care in Guatemala PDFDocument6 pagesPBC 2012 JCI Standards To Evaluate and Improve Pediatric Oncology Nursing Care in Guatemala PDFEMIGDIO1969No ratings yet
- What Is Clinical GovernanceDocument8 pagesWhat Is Clinical GovernanceApollwn100% (1)
- ASSIGNMENT PlannigDocument6 pagesASSIGNMENT Plannigprabhjot singhNo ratings yet
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsFrom EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsNo ratings yet
- Closing Remarks - Nursing Midwifery LeadershipDocument19 pagesClosing Remarks - Nursing Midwifery LeadershipJhpiegoNo ratings yet
- GE Foundation Awards Jhpiego $2.3 Million To Accelerate Global Health InnovationsDocument2 pagesGE Foundation Awards Jhpiego $2.3 Million To Accelerate Global Health InnovationsJhpiegoNo ratings yet
- Cervical Cancer Screening - JhpiegoDocument15 pagesCervical Cancer Screening - JhpiegoJhpiego100% (1)
- Seizing The Opportunity - Working With Adolescent Boys For An HIV-free Generation"Document14 pagesSeizing The Opportunity - Working With Adolescent Boys For An HIV-free Generation"JhpiegoNo ratings yet
- Spatial Mapping Results in a Successful Large-Scale Voluntary Medical Male Circumcision (VMMC) Campaign: Using GIS Data for Decision-Making Positively Impacts the VMMC Scale-Up in Iringa and Njombe Regions of TanzaniaDocument1 pageSpatial Mapping Results in a Successful Large-Scale Voluntary Medical Male Circumcision (VMMC) Campaign: Using GIS Data for Decision-Making Positively Impacts the VMMC Scale-Up in Iringa and Njombe Regions of TanzaniaJhpiegoNo ratings yet
- Community Health Workers Creating Family Planning Social Networks Through Satisified ClientsDocument15 pagesCommunity Health Workers Creating Family Planning Social Networks Through Satisified ClientsJhpiegoNo ratings yet
- Capturing A Missed Opportunity Through Postpartum Intrauterine Contraceptive Device (PPIUCD) in Ethiopia: Experience of The Maternal and Child Health Integrated Program (MCHIP)Document13 pagesCapturing A Missed Opportunity Through Postpartum Intrauterine Contraceptive Device (PPIUCD) in Ethiopia: Experience of The Maternal and Child Health Integrated Program (MCHIP)JhpiegoNo ratings yet
- Screening For Maternal Anemia: A Low-Cost Solution For A Persistent Global Health ChallengeDocument1 pageScreening For Maternal Anemia: A Low-Cost Solution For A Persistent Global Health ChallengeJhpiegoNo ratings yet
- Date/Time: Thursday, November 14, 2013 Session: 2.2.11 Family Planning and Quality of CareDocument2 pagesDate/Time: Thursday, November 14, 2013 Session: 2.2.11 Family Planning and Quality of CareJhpiegoNo ratings yet
- Improving Maternal Child Health (MCH) ServicesDocument22 pagesImproving Maternal Child Health (MCH) ServicesJhpiegoNo ratings yet
- Pre-Test - Pediatric NursingDocument6 pagesPre-Test - Pediatric NursingogiskuadzNo ratings yet
- EWRFDocument1 pageEWRFHarini Sybel CullenNo ratings yet
- 10 Sample Paper Chennai Region 2Document11 pages10 Sample Paper Chennai Region 2Illaya BharathiNo ratings yet
- Manual On Settlement of Land DisputesDocument120 pagesManual On Settlement of Land Disputescookbooks&lawbooks100% (1)
- A Level Essay Questions by TopicsDocument11 pagesA Level Essay Questions by TopicsDD97No ratings yet
- Oisd STD 235Document110 pagesOisd STD 235naved ahmed100% (5)
- M607 L01 SolutionDocument7 pagesM607 L01 SolutionRonak PatelNo ratings yet
- Analysis of Credit Risk Measurement UsinDocument6 pagesAnalysis of Credit Risk Measurement UsinDia-wiNo ratings yet
- UBX Cloud - VEEAM Cloud Backup SlickDocument2 pagesUBX Cloud - VEEAM Cloud Backup SlickmohamedalihashNo ratings yet
- Aipmt Round 3Document335 pagesAipmt Round 3AnweshaBoseNo ratings yet
- Weekly Report w34Document19 pagesWeekly Report w34Asep MAkmurNo ratings yet
- FINA3010 Assignment1Document5 pagesFINA3010 Assignment1Hei RayNo ratings yet
- LABELDocument2 pagesLABELerinNo ratings yet
- ProjectDocument3 pagesProjectKimzee kingNo ratings yet
- The Effectiveness of Bilingual Program and Policy in The Academic Performance and Engagement of StudentsDocument10 pagesThe Effectiveness of Bilingual Program and Policy in The Academic Performance and Engagement of StudentsJoshua LagonoyNo ratings yet
- Ers. Co M: JANA Master Fund, Ltd. Performance Update - December 2010 Fourth Quarter and Year in ReviewDocument10 pagesErs. Co M: JANA Master Fund, Ltd. Performance Update - December 2010 Fourth Quarter and Year in ReviewVolcaneum100% (2)
- Media Release 3665 (English) 14 08 14Document2 pagesMedia Release 3665 (English) 14 08 14ElPaisUyNo ratings yet
- emPower-API-Specification-v0 90 PDFDocument26 pagesemPower-API-Specification-v0 90 PDFPape Mignane FayeNo ratings yet
- Assessment Form: Monitoring The Functionality of City/Municipal Council For The Protection of Children (C/MCPC)Document3 pagesAssessment Form: Monitoring The Functionality of City/Municipal Council For The Protection of Children (C/MCPC)dilg libmananNo ratings yet
- Acc21 March18Document12 pagesAcc21 March18Romero Mary Jane C.No ratings yet
- Milvik ProposalDocument29 pagesMilvik ProposalMin HajNo ratings yet
- Negara Hukum-5-1-Juni-2014Document99 pagesNegara Hukum-5-1-Juni-2014haekalnashvilleNo ratings yet
- Vinayyak - CV - Sap - ExpDocument3 pagesVinayyak - CV - Sap - ExpmanikandanNo ratings yet
- Responsibility Accounting Practice ProblemDocument4 pagesResponsibility Accounting Practice ProblemBeomiNo ratings yet
- Other Hands - Issue #15-16, Supplement PDFDocument8 pagesOther Hands - Issue #15-16, Supplement PDFAlHazredNo ratings yet
- Memorial For The Appellants-Team Code L PDFDocument44 pagesMemorial For The Appellants-Team Code L PDFAbhineet KaliaNo ratings yet
- ICICI Prudential Life Insurance CompanyDocument21 pagesICICI Prudential Life Insurance CompanySayantan ChoudhuryNo ratings yet
- Theory, Culture & Society: The AestheticDocument8 pagesTheory, Culture & Society: The AestheticJaime UtrerasNo ratings yet