Download as pdf or txt
You might also like
- Vincent Brody Care PlanDocument10 pagesVincent Brody Care PlanKarina Rodriguez50% (2)
- Lab09 Therapy4 IronDeficiencyDocument5 pagesLab09 Therapy4 IronDeficiencyHayna Rose100% (1)
- Chapter 12 - Hypertension - Pass The Salt, Please Level IIDocument7 pagesChapter 12 - Hypertension - Pass The Salt, Please Level IIRichix K Yabe0% (1)
- 03 PsoriasisDocument28 pages03 PsoriasisGlen Lester ChiongNo ratings yet
- Renal Case Study Final-2Document7 pagesRenal Case Study Final-2api-295221163100% (1)
- COPD Case StudyDocument4 pagesCOPD Case StudyPj Declarador100% (4)
- ACUTE AND CHRONIC PANCREATITIS-undoneDocument6 pagesACUTE AND CHRONIC PANCREATITIS-undonecory kurdapyaNo ratings yet
- Case Study RSsp2010Document18 pagesCase Study RSsp2010harvey63No ratings yet
- Cystic Fibrosis: Prepared By: Johanna PepitoDocument38 pagesCystic Fibrosis: Prepared By: Johanna PepitoDharrenceNo ratings yet
- Case Study #31: Nutrition Support in Sepsis and Morbid ObesityDocument24 pagesCase Study #31: Nutrition Support in Sepsis and Morbid ObesityCuteScribd100% (1)
- COPD Case StudyDocument23 pagesCOPD Case StudyXinyun XuNo ratings yet
- Laki-Laki, 21 Tahun Dengan Ketoasidosis DiabetikumDocument66 pagesLaki-Laki, 21 Tahun Dengan Ketoasidosis DiabetikumAnonymous gudRSKNo ratings yet
- Mortality-conference-2022.03.24 FINAL (自動儲存)Document51 pagesMortality-conference-2022.03.24 FINAL (自動儲存)許誌元No ratings yet
- Final DraftDocument6 pagesFinal DraftSimon KingNo ratings yet
- Nephrorounds3 2015final 150907110921 Lva1 App6892 PDFDocument133 pagesNephrorounds3 2015final 150907110921 Lva1 App6892 PDFTabada NickyNo ratings yet
- PneumoniaDocument69 pagesPneumoniaHamna ZainabNo ratings yet
- Case Presentation On Chronic BronchitisDocument20 pagesCase Presentation On Chronic BronchitisSafoora RafeeqNo ratings yet
- Nursing CareDocument13 pagesNursing CareKelvin TetoNo ratings yet
- Sample Patient ProfileDocument2 pagesSample Patient ProfileHanako ShigaNo ratings yet
- Askep CKD Bahasa InggrisDocument10 pagesAskep CKD Bahasa InggrisElisabeth PanjaitanNo ratings yet
- COPDDocument49 pagesCOPDArmoured SpartanNo ratings yet
- Case-Based Learning Thoracic Medicine: Chronic Obstructive Pulmonary DiseaseDocument22 pagesCase-Based Learning Thoracic Medicine: Chronic Obstructive Pulmonary DiseaseAnonymous HNTNhspNo ratings yet
- CopdDocument31 pagesCopdapi-483519259No ratings yet
- COPD3Document77 pagesCOPD3mohammedNo ratings yet
- Ajuomar - PmeumophysiologyDocument12 pagesAjuomar - PmeumophysiologyajuomarNo ratings yet
- NCP PneumoniaDocument47 pagesNCP Pneumoniabhevpat251100% (1)
- Tn. Ngadiran, r25Document21 pagesTn. Ngadiran, r25alanaaluNo ratings yet
- Copd 2022Document45 pagesCopd 2022Mubassir NisarNo ratings yet
- Case Conference Saturday Night Shift, MAY 4TH, 2019Document28 pagesCase Conference Saturday Night Shift, MAY 4TH, 2019Primadiati Nickyta SariNo ratings yet
- NFSC 471-Case StudyDocument8 pagesNFSC 471-Case Studyapi-242439244No ratings yet
- Pulmonary Sequele After COVID-19Document61 pagesPulmonary Sequele After COVID-19Nandha KumarNo ratings yet
- Crohns DiseaseDocument21 pagesCrohns DiseaseKasuganti koteshwar raoNo ratings yet
- Pulmonary CSDocument8 pagesPulmonary CSdakotaNo ratings yet
- Diabetic Ketoacidosis Case PresentationDocument37 pagesDiabetic Ketoacidosis Case PresentationNathan Vince Cruz100% (2)
- Asthma COPD Overlap Syndrome - ACOSDocument59 pagesAsthma COPD Overlap Syndrome - ACOSdrmaqsoodaliNo ratings yet
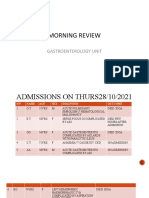
- MR GastroDocument31 pagesMR GastroAdefuye AbiolaNo ratings yet
- D5W (Dextrose 5%) ClassDocument4 pagesD5W (Dextrose 5%) ClassHanilyn ArdinaNo ratings yet
- Case Based CCNDocument36 pagesCase Based CCNKeep smileNo ratings yet
- CopdDocument32 pagesCopdMalou Yap BuotNo ratings yet
- Studi KasusDocument9 pagesStudi KasusWina YustisiaNo ratings yet
- Case Conference Saturday Night Shift, MAY 4TH, 2019Document28 pagesCase Conference Saturday Night Shift, MAY 4TH, 2019Primadiati Nickyta SariNo ratings yet
- Morning Report: Wednesday, March 8 2017Document14 pagesMorning Report: Wednesday, March 8 2017Safitri NindyaNo ratings yet
- HyperDocument21 pagesHyperayamalkawi204No ratings yet
- CC 2 Okt Hcu NeoDocument26 pagesCC 2 Okt Hcu NeolatifahNo ratings yet
- Nufd 488 - Cancer Case Study-7Document19 pagesNufd 488 - Cancer Case Study-7api-487121869No ratings yet
- PneumoniaDocument9 pagesPneumoniaRSNo ratings yet
- Differences Between AKURIT and Conventional TB DrugsDocument16 pagesDifferences Between AKURIT and Conventional TB DrugsKay RuzNo ratings yet
- CKDDocument48 pagesCKDJuniorNo ratings yet
- Shared RX Modules For FinalsDocument11 pagesShared RX Modules For FinalsOdyNo ratings yet
- IMED Case 2-1Document6 pagesIMED Case 2-1Shakshi RainaNo ratings yet
- Case Study 1Document15 pagesCase Study 1api-272464131100% (2)
- DGR Jeyjuj Il.Document15 pagesDGR Jeyjuj Il.Muhammad Cholis HidayatNo ratings yet
- Iron Deficiency Anameia (1)Document12 pagesIron Deficiency Anameia (1)LOW XIN LENGNo ratings yet
- PEDIA - TachypneaDocument12 pagesPEDIA - TachypneaAlvin Germo PasuquinNo ratings yet
- IMED Case 1-1Document6 pagesIMED Case 1-1Shakshi RainaNo ratings yet
- 70, - H 35 - H 2 - O N, L T: T: E G D - Develop A Self Management PlanDocument11 pages70, - H 35 - H 2 - O N, L T: T: E G D - Develop A Self Management PlanjljoioiuNo ratings yet
- Morning Report Case: June 7, 2011Document16 pagesMorning Report Case: June 7, 2011LittleChenaNo ratings yet
- Management of COPD in Primary and Secondary Care, TheFrom EverandManagement of COPD in Primary and Secondary Care, TheRating: 5 out of 5 stars5/5 (1)
- 500 Ketogenic Recipes: Hundreds of Easy and Delicious Recipes for Losing Weight, Improving Your Health, and Staying in the Ketogenic ZoneFrom Everand500 Ketogenic Recipes: Hundreds of Easy and Delicious Recipes for Losing Weight, Improving Your Health, and Staying in the Ketogenic ZoneRating: 5 out of 5 stars5/5 (1)
- Neurological Assgfhgfhfgessment 1Document8 pagesNeurological Assgfhgfhfgessment 1Husaifah BaliwanNo ratings yet
- Porcellio Scaber and Its Expression in Sternal Epithelia During The Moult CycleDocument9 pagesPorcellio Scaber and Its Expression in Sternal Epithelia During The Moult CycleHusaifah BaliwanNo ratings yet
- In Patients With Acute CholecystitisDocument2 pagesIn Patients With Acute CholecystitisHusaifah BaliwanNo ratings yet
- AnatomyDocument4 pagesAnatomyHusaifah BaliwanNo ratings yet
- Nausea and VomitingDocument9 pagesNausea and VomitingHusaifah BaliwanNo ratings yet
- Protifar Recipe BookletDocument16 pagesProtifar Recipe BookletHusaifah BaliwanNo ratings yet
- Something Substantial Fin Alp 2Document1 pageSomething Substantial Fin Alp 2Husaifah BaliwanNo ratings yet
- Assessment of Chest and LungsDocument23 pagesAssessment of Chest and LungsBaniwas Marie Agnes100% (1)
- Health Teaching Plan CalalangDocument5 pagesHealth Teaching Plan CalalangPhilip R. Marallag0% (1)
- Anterior Posterior Lateral Superior Inferior: of 1 2 Vascular Biology LECTURE 1Document2 pagesAnterior Posterior Lateral Superior Inferior: of 1 2 Vascular Biology LECTURE 1Fazreena EleenaNo ratings yet
- Ncle X RN Test Study GuideDocument199 pagesNcle X RN Test Study GuideKIT100% (1)
- Tobacco Smoking For Igcse BiologyDocument10 pagesTobacco Smoking For Igcse BiologyAbdul RehmanNo ratings yet
- Bronchial Asthma Final CompilationDocument51 pagesBronchial Asthma Final CompilationNurdalila ZabaNo ratings yet
- Autopeep Paul Pepe Jhon MariniDocument5 pagesAutopeep Paul Pepe Jhon MariniRenatoNo ratings yet
- Bronchopulmonary Dysplasia (BPD)Document13 pagesBronchopulmonary Dysplasia (BPD)Joan BuiNo ratings yet
- Teen-Health-Literacy B v9 vb0 s1Document48 pagesTeen-Health-Literacy B v9 vb0 s1Hannah Shiela MendozaNo ratings yet
- English ChillaDocument8 pagesEnglish ChillaChilla Adis ViolitaNo ratings yet
- Basic Concepts of Heart-Lung Interactions During Mechanical VentilationDocument14 pagesBasic Concepts of Heart-Lung Interactions During Mechanical VentilationanindiawNo ratings yet
- Atelectasis. Mechanisms, Diagnosis and Management (Peroni, 2000)Document5 pagesAtelectasis. Mechanisms, Diagnosis and Management (Peroni, 2000)Renato Li SoldevillaNo ratings yet
- NJ Dolphin Necropsy ReportDocument5 pagesNJ Dolphin Necropsy ReportopracrusadesNo ratings yet
- Laporan PRB RsucmDocument12 pagesLaporan PRB RsucmKurnia WatiNo ratings yet
- Empyema: An Uncommon Complication of Common Pneumonia: Heather Hsu, HMS III Gillian Lieberman, MDDocument0 pagesEmpyema: An Uncommon Complication of Common Pneumonia: Heather Hsu, HMS III Gillian Lieberman, MDAldo EmeraldNo ratings yet
- Assessment of Respiratory Muscle Function StrengthDocument8 pagesAssessment of Respiratory Muscle Function StrengthsstavrosNo ratings yet
- Science 9 DLP Q1 W1 D3Document7 pagesScience 9 DLP Q1 W1 D3ErwinNo ratings yet
- Nursing Care in Patient With Acute Cardiogenic Pulmonary EdemaDocument5 pagesNursing Care in Patient With Acute Cardiogenic Pulmonary EdemaAyyu Sandhi100% (1)
- Occupational Lung DiseasesDocument75 pagesOccupational Lung DiseasesAnonymous h1XAlApsU100% (1)
- EVS Learning Material Class 3 Our Body-A Living MachineDocument14 pagesEVS Learning Material Class 3 Our Body-A Living Machinesuhani.kaurNo ratings yet
- ACUTE RESPIRATORY FAILURE QuizDocument3 pagesACUTE RESPIRATORY FAILURE QuizTrish 001950% (2)
- A Detailed Lesson Plan in Earth and Life Science Organ SystemDocument11 pagesA Detailed Lesson Plan in Earth and Life Science Organ SystemRodelyn Dahay CalluengNo ratings yet
- Legal Med CasesDocument53 pagesLegal Med CasesAndrew MarzNo ratings yet
- Michael Servetus (1511-1553) and The Discovery of Pulmonary CirculationDocument6 pagesMichael Servetus (1511-1553) and The Discovery of Pulmonary CirculationMastering Zinc OxideNo ratings yet
- The Respiratory System LessonDocument2 pagesThe Respiratory System LessonKristine Ann Gocotano Dadole100% (2)
- Acupuncture Miriam Lee - Yin and Yang - HeartDocument24 pagesAcupuncture Miriam Lee - Yin and Yang - HeartAurora Alina Bujor-FlueranNo ratings yet
- Development of The Limbs: Mesoderm and Migrating MyotomesDocument27 pagesDevelopment of The Limbs: Mesoderm and Migrating MyotomesHany Shawky Nadim89% (9)
- 13 1.lung Auscultation#8E2EDocument23 pages13 1.lung Auscultation#8E2EAlina CazanNo ratings yet
- General AnatomyDocument25 pagesGeneral AnatomyAltamae IbayNo ratings yet
- Science 6 q2 Mod1Document20 pagesScience 6 q2 Mod13tj internetNo ratings yet