Download as pdf
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Mania-Nursing Care PlanDocument2 pagesMania-Nursing Care PlanTracy74% (34)
- Soap NoteDocument2 pagesSoap Notetopopirate100% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Adventurers' Guild - SwordtagDocument12 pagesAdventurers' Guild - Swordtagtruly epicNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Common List of Cardiac DrugsDocument3 pagesCommon List of Cardiac DrugsTracy100% (3)
- Alcohol Withdrawal Assessment SheetsDocument2 pagesAlcohol Withdrawal Assessment SheetsTracy100% (1)
- PAS Quick GuideDocument1 pagePAS Quick GuideTracyNo ratings yet
- Cardiac Meds To MemorizeDocument4 pagesCardiac Meds To MemorizekellyaeNo ratings yet
- Acid Base DisturbancesDocument34 pagesAcid Base DisturbancesTracy100% (1)
- ABG Interpretation: Julie Perkins RRT-NPS LPCH Respiratory CareDocument14 pagesABG Interpretation: Julie Perkins RRT-NPS LPCH Respiratory CareTracy100% (5)
- Appendix B: Clinical Institute Withdrawal Assessment For Alcohol (CIWA-A)Document2 pagesAppendix B: Clinical Institute Withdrawal Assessment For Alcohol (CIWA-A)Tracy100% (1)
- Intravenous Fluid SelectionDocument12 pagesIntravenous Fluid SelectionTracy100% (4)
- Drug Calculation TutorialDocument13 pagesDrug Calculation TutorialTracyNo ratings yet
- Patient Implantable Medical DevicesDocument1 pagePatient Implantable Medical DevicesTracy100% (1)
- Common Cardiac Related MedicationsDocument18 pagesCommon Cardiac Related MedicationsTracy100% (2)
- Abg InterpretationDocument14 pagesAbg Interpretationmara5140100% (7)
- ScoliosisDocument3 pagesScoliosisTracy100% (1)
- Common Lab Values-ABG, CBG, Urinalysis, Mechanical TestingDocument2 pagesCommon Lab Values-ABG, CBG, Urinalysis, Mechanical TestingTracy75% (4)
- SBARQ FormDocument1 pageSBARQ FormTracy100% (5)
- Spina BifidaDocument2 pagesSpina BifidaTracy100% (2)
- Useful AbbreviationsDocument2 pagesUseful AbbreviationsTracyNo ratings yet
- Documenting A Transfusion Reaction: Chart SmartDocument2 pagesDocumenting A Transfusion Reaction: Chart SmartTracyNo ratings yet
- Types of PainDocument1 pageTypes of PainTracy100% (3)
- Nursing Care Plan GuideDocument1 pageNursing Care Plan GuideTracy100% (1)
- Cleft Lip and PalateDocument2 pagesCleft Lip and PalateTracy100% (1)
- Cerebral PalsyDocument2 pagesCerebral PalsyTracy100% (1)
- Fetal CirculationDocument2 pagesFetal CirculationTracy88% (8)
- Healing of FracturesDocument19 pagesHealing of FracturesTracy100% (4)
- Principles of Wound HealingDocument8 pagesPrinciples of Wound HealingTracy100% (6)
- Pregnancy: Signs/Symptoms and Common Health ConcernsDocument5 pagesPregnancy: Signs/Symptoms and Common Health ConcernsTracy50% (2)
- The Stigma of Mental IllnessDocument42 pagesThe Stigma of Mental IllnessTracy100% (5)
- TP-Link WiFi 6E AXE5400 PCIe WiFi Card - User GuideDocument23 pagesTP-Link WiFi 6E AXE5400 PCIe WiFi Card - User GuidehelpfulNo ratings yet
- WCR AscoDocument12 pagesWCR AscojuliosieteNo ratings yet
- FB-1 - Beam Detector Specification PDFDocument1 pageFB-1 - Beam Detector Specification PDFRafiq MagdyNo ratings yet
- Wall Colmonoy - Properties of Hard Surfacing Alloy Colmonoy 88 - July 2019Document8 pagesWall Colmonoy - Properties of Hard Surfacing Alloy Colmonoy 88 - July 2019joseocsilvaNo ratings yet
- 8 Gartner Magic Quadrant For A 774338Document40 pages8 Gartner Magic Quadrant For A 774338joao.lucas.ribeiroNo ratings yet
- Fertilizacion Nitrogenada en Maiz Basada en Materia Organica (Sanchez Roldan)Document33 pagesFertilizacion Nitrogenada en Maiz Basada en Materia Organica (Sanchez Roldan)Brian RamosNo ratings yet
- CTEO Chapter II B Chemistry and 10 Clinker FactsDocument43 pagesCTEO Chapter II B Chemistry and 10 Clinker FactsFranciscoCorreaJara100% (2)
- Waupaca Elevator BrochureDocument16 pagesWaupaca Elevator BrochureMade Agus BudiarthaNo ratings yet
- Descargar Manual de Taller Daewoo Tico PDFDocument2 pagesDescargar Manual de Taller Daewoo Tico PDFAlfredo Supo HuarayaNo ratings yet
- Unit 2.ieltsDocument11 pagesUnit 2.ieltsKarina HrishkovskaNo ratings yet
- Moloney Johannine TheologyDocument20 pagesMoloney Johannine Theologygogel33% (3)
- Clanbook Tremere (Revised Edition) (2000) WW2357 (With Bookmarks) (OEF)Document107 pagesClanbook Tremere (Revised Edition) (2000) WW2357 (With Bookmarks) (OEF)cwod100% (1)
- Non Verbal CommunicationDocument26 pagesNon Verbal Communicationrooroli74No ratings yet
- Asthma Action PlanDocument1 pageAsthma Action PlanAkosNo ratings yet
- Cell Division: Mitosis & MeiosisDocument50 pagesCell Division: Mitosis & MeiosisLyca GunayNo ratings yet
- Methods of Approximation and Determination of Human Vulnerability For Offshore Major Accident Hazard AssessmentDocument55 pagesMethods of Approximation and Determination of Human Vulnerability For Offshore Major Accident Hazard AssessmenthazopmanNo ratings yet
- X1D - USER GUIDE English PDFDocument157 pagesX1D - USER GUIDE English PDFSteveNo ratings yet
- Printmaking Unit Plan - Amy Robertson Revised By: Deanna Plested GradeDocument47 pagesPrintmaking Unit Plan - Amy Robertson Revised By: Deanna Plested Gradeapi-264279988No ratings yet
- J.saintifika Uji Bioavailabilitas Dan BioekivalensiDocument8 pagesJ.saintifika Uji Bioavailabilitas Dan BioekivalensiAhmad MujahidinNo ratings yet
- Group 3 Tests and Adjustments Group 3 Tests and AdjustmentsDocument15 pagesGroup 3 Tests and Adjustments Group 3 Tests and AdjustmentsGlaitonNo ratings yet
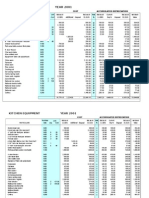
- Fixed Asset RegisterDocument3 pagesFixed Asset Registerzuldvsb0% (1)
- STEP 1 Could It Be HIV? STEP 2 Informed Consent and Testing STEP 3 Conveying Test ResultsDocument2 pagesSTEP 1 Could It Be HIV? STEP 2 Informed Consent and Testing STEP 3 Conveying Test ResultsahjkseflhasefNo ratings yet
- 02B - MYSTIKO OΠΛΟ HAARP ΑΚΤΙΝΟΒΟΛΙΕΣ - EGDocument325 pages02B - MYSTIKO OΠΛΟ HAARP ΑΚΤΙΝΟΒΟΛΙΕΣ - EGO TΣΑΡΟΣ ΤΗΣ ΑΝΤΙΒΑΡΥΤΗΤΑΣ ΛΙΑΠΗΣ ΠΑΝΑΓΙΩΤΗΣNo ratings yet
- Lecture 3 - Purpose of ArtDocument46 pagesLecture 3 - Purpose of ArtGrace LabayneNo ratings yet
- Shapeshell - Steel Structure Painting Technical Specification 2020-02-10 PDFDocument4 pagesShapeshell - Steel Structure Painting Technical Specification 2020-02-10 PDFmorisNo ratings yet
- Framework of Wild Life (Protection) Act, 1972Document17 pagesFramework of Wild Life (Protection) Act, 1972ishikakeswani4No ratings yet
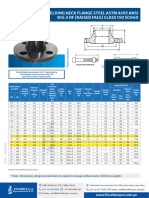
- Bridas WN Clase 150Document1 pageBridas WN Clase 150juan ormacheaNo ratings yet
- Underwater Windmill: A Seminar Report OnDocument52 pagesUnderwater Windmill: A Seminar Report OnShaik Towheed BanuNo ratings yet
- Advanced Graphics - ActivityDocument6 pagesAdvanced Graphics - ActivityReyan AKNo ratings yet