Download as pdf or txt
You might also like
- Emergency Antibiotic Guide A6 105 1048mm February9 2022Document48 pagesEmergency Antibiotic Guide A6 105 1048mm February9 2022Iain HarrisonNo ratings yet
- Colorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsDocument48 pagesColorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsBrian HarrisNo ratings yet
- Precipitation ProcessesDocument2 pagesPrecipitation ProcessesThembi Matebula100% (1)
- Different Classification of FeedstuffDocument13 pagesDifferent Classification of FeedstuffNiño Joshua Ong Balbin67% (6)
- Service-manual-SG Emachines E725 E525 031809Document236 pagesService-manual-SG Emachines E725 E525 031809andhrimnirNo ratings yet
- Toshiba Case 3Document4 pagesToshiba Case 3Deta Detade100% (1)
- Colorado Guidelines of Professional Practice For Controlled SubstancesDocument65 pagesColorado Guidelines of Professional Practice For Controlled SubstancesBrian HarrisNo ratings yet
- Managerial Level-1: Part - Aweightage 20%Document6 pagesManagerial Level-1: Part - Aweightage 20%fawad aslamNo ratings yet
- Doryx Drug DescriptionDocument9 pagesDoryx Drug DescriptionJj DelacruzNo ratings yet
- FilariasisDocument8 pagesFilariasisBangaru BabuNo ratings yet
- Current Treatment of Oral Candidiasis: A Literature ReviewDocument12 pagesCurrent Treatment of Oral Candidiasis: A Literature ReviewgilangNo ratings yet
- CandidiasisDocument3 pagesCandidiasisYanna Habib-MangotaraNo ratings yet
- Double Anaerobic Coverage Guideline AgainstDocument2 pagesDouble Anaerobic Coverage Guideline AgainstioanaNo ratings yet
- Monograph-ID1007600-TOBROSONDocument4 pagesMonograph-ID1007600-TOBROSONSanEmirzaNo ratings yet
- AmeobaDocument4 pagesAmeobaCristinaNo ratings yet
- Jase Medical Antibiotic GuideDocument33 pagesJase Medical Antibiotic GuideelectronicoscaldasNo ratings yet
- Rifaximin For The Treatment of TDDocument11 pagesRifaximin For The Treatment of TDAnkur AgrawalNo ratings yet
- Jurnal 1.topical Ivermectin-Metronidazole Gel Therapy in The Treatment of BlepharitisDocument6 pagesJurnal 1.topical Ivermectin-Metronidazole Gel Therapy in The Treatment of BlepharitisChintya Redina HapsariNo ratings yet
- Viru El Adelmo No 23Document37 pagesViru El Adelmo No 23garciaarielfrancisco9No ratings yet
- Doxycycline in Clinical MedicineDocument4 pagesDoxycycline in Clinical Medicinethanh ba matNo ratings yet
- Guidelines For Treatment of Infections in Primary Care in Hull and East RidingDocument22 pagesGuidelines For Treatment of Infections in Primary Care in Hull and East RidingSiLvia Riska PratiwiNo ratings yet
- Journal Reading - HordeolumDocument20 pagesJournal Reading - HordeolumsnylstlNo ratings yet
- Drugs For Common Eye Problems: Cecilia A. Jimeno, M.DDocument70 pagesDrugs For Common Eye Problems: Cecilia A. Jimeno, M.Dpriti089No ratings yet
- DoxycyclineDocument1 pageDoxycyclineRimsha AzeemNo ratings yet
- Prophylactic Use of Anti-Microbial Agents: Presented By: Jagir R. Patel Assistant ProfessorDocument18 pagesProphylactic Use of Anti-Microbial Agents: Presented By: Jagir R. Patel Assistant ProfessorJagirNo ratings yet
- JurnalDocument4 pagesJurnalAnonymous pfHZusnNo ratings yet
- Candidiasis (Brut)Document6 pagesCandidiasis (Brut)Ilyes FerenczNo ratings yet
- Tra KhomaDocument7 pagesTra KhomaLinda ArimbiNo ratings yet
- XDR Typhoid Advisory Feb 19Document1 pageXDR Typhoid Advisory Feb 19Dr.Asad RehmanNo ratings yet
- Idcm 2020 0006Document12 pagesIdcm 2020 0006tennakoonk943No ratings yet
- CDC Diphtheria Surveillance WorksheetDocument6 pagesCDC Diphtheria Surveillance WorksheetLuna WhiteNo ratings yet
- Dexamethasone: Quick LinksDocument5 pagesDexamethasone: Quick Linksali aliNo ratings yet
- Treatment of Chlamydia Trachomatis InfectionDocument23 pagesTreatment of Chlamydia Trachomatis InfectionAmbarNo ratings yet
- Evolving Patient Care: The Pharmacists' Role: Jessica Haskins-Cummings, Pharmd Pharmacy Manager, WalgreensDocument26 pagesEvolving Patient Care: The Pharmacists' Role: Jessica Haskins-Cummings, Pharmd Pharmacy Manager, WalgreensJavad Rahman NezhadNo ratings yet
- What Is Multidrug-Resistant Tuberculosis (MDR-TB) ?Document63 pagesWhat Is Multidrug-Resistant Tuberculosis (MDR-TB) ?Birhanu AbebeNo ratings yet
- Treatment of Chlamydia Trachomatis InfectionDocument9 pagesTreatment of Chlamydia Trachomatis InfectioneeeeewwwwwNo ratings yet
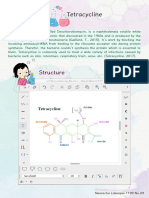
- TetracyclineDocument5 pagesTetracyclineapi-296073547No ratings yet
- Khamlin Hamad Abdal - GroupeaDocument39 pagesKhamlin Hamad Abdal - GroupeaKhamlin NurseNo ratings yet
- Khamlin Hamad Abdal - GroupeaDocument39 pagesKhamlin Hamad Abdal - GroupeaKhamlin NurseNo ratings yet
- Macro Li DesDocument15 pagesMacro Li DesSEIYADU IBRAHIM KNo ratings yet
- Acne Vulgaris Management: What's New and What's Still True?: Review ArticleDocument5 pagesAcne Vulgaris Management: What's New and What's Still True?: Review ArticleAlmuizzu NurjannahNo ratings yet
- The Role of Antifungal Drugs in The Management of Denture-Associated StomatitisDocument5 pagesThe Role of Antifungal Drugs in The Management of Denture-Associated StomatitisInternational Medical PublisherNo ratings yet
- G AntibiotictherapyDocument3 pagesG AntibiotictherapyJavangula Tripura PavitraNo ratings yet
- Clostridium Difficile Infection Fidaxomicin Esnm1Document11 pagesClostridium Difficile Infection Fidaxomicin Esnm1Pet UrNo ratings yet
- The Use of DDT in Malaria Vector ControlDocument16 pagesThe Use of DDT in Malaria Vector ControlIsis BugiaNo ratings yet
- Current Treatment of Oral Candidiasis A Literature ReviewDocument8 pagesCurrent Treatment of Oral Candidiasis A Literature ReviewRonaldo PutraNo ratings yet
- 25.antifungal NigamPKDocument10 pages25.antifungal NigamPKnurulunismuhNo ratings yet
- Keratoconjuncitivitis Treatment ALLDocument13 pagesKeratoconjuncitivitis Treatment ALLNorhan KhaledNo ratings yet
- BPJ Vol 14 No 2 P 1077-1086Document10 pagesBPJ Vol 14 No 2 P 1077-1086Emeray EssenceNo ratings yet
- Maxitrol (Neomycin and Polymyxin B Sulfates and Dexamethasone Ophthalmic Ointment) Sterile Description: MaxitrolDocument6 pagesMaxitrol (Neomycin and Polymyxin B Sulfates and Dexamethasone Ophthalmic Ointment) Sterile Description: Maxitroldjilal430No ratings yet
- Examination Card 10Document9 pagesExamination Card 10FUTURE DOCTORNo ratings yet
- Decadron: (Dexamethasone Tablets, Usp)Document8 pagesDecadron: (Dexamethasone Tablets, Usp)Anonymous QqyLDoW1No ratings yet
- DiphtheriaDocument25 pagesDiphtheriaRohan TejaNo ratings yet
- Tobradex SuspensionDocument4 pagesTobradex SuspensionKaka KakoNo ratings yet
- How Are Odontogenic Infections Best ManagedDocument5 pagesHow Are Odontogenic Infections Best ManagedNurfidini AzmiNo ratings yet
- TBDocument5 pagesTBSuneel KumarNo ratings yet
- Fungal InfectionsDocument13 pagesFungal Infectionspragna novaNo ratings yet
- Title: Antibiotic Guideline For Acute Pelvic Inflammatory DiseaseDocument5 pagesTitle: Antibiotic Guideline For Acute Pelvic Inflammatory DiseaseresortbabeNo ratings yet
- Antimicrobial Prescribing Delafloxacin For Acute Bacterial Skin and Skin Structure Infections PDF 1158232915141Document6 pagesAntimicrobial Prescribing Delafloxacin For Acute Bacterial Skin and Skin Structure Infections PDF 1158232915141carlettino7No ratings yet
- Antibiotics 07 00059 v2Document8 pagesAntibiotics 07 00059 v2alfiraNo ratings yet
- Pelvic Inflammatory Disease MedicationDocument5 pagesPelvic Inflammatory Disease MedicationErick DuqueNo ratings yet
- GP 2 PresentationDocument18 pagesGP 2 PresentationmechellesibandaNo ratings yet
- The Essential Guide to Doxycycline: Usage, Precautions, Interactions and Side Effects.From EverandThe Essential Guide to Doxycycline: Usage, Precautions, Interactions and Side Effects.No ratings yet
- The Essential Guide to Metronidazole: Usage, Precautions, Interactions and Side Effects.From EverandThe Essential Guide to Metronidazole: Usage, Precautions, Interactions and Side Effects.No ratings yet
- Practical Patch Testing and Chemical Allergens in Contact DermatitisFrom EverandPractical Patch Testing and Chemical Allergens in Contact DermatitisNo ratings yet
- The Ideal Candida Diet Cookbook; The Superb Diet Guide To Alleviate Candida Symptoms And Restore Gut Health With Nutritious RecipesFrom EverandThe Ideal Candida Diet Cookbook; The Superb Diet Guide To Alleviate Candida Symptoms And Restore Gut Health With Nutritious RecipesNo ratings yet
- Colorado Medical Board Policy Guidelines For The Use of Controlled Substances For The Treatment of Pain 12-36-117, C.R.S.Document5 pagesColorado Medical Board Policy Guidelines For The Use of Controlled Substances For The Treatment of Pain 12-36-117, C.R.S.Brian HarrisNo ratings yet
- Colorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Document69 pagesColorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Brian HarrisNo ratings yet
- Colorado Peace Officer Manual 2013Document373 pagesColorado Peace Officer Manual 2013Brian Harris100% (1)
- Colorado Preferred Drug List (PDL) 2013Document25 pagesColorado Preferred Drug List (PDL) 2013Brian HarrisNo ratings yet
- Colorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Document69 pagesColorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Brian HarrisNo ratings yet
- Colorado Medical Board Policy Guidelines Pertaining To The Release and Retention of Medical Records Policy Number 40-07Document2 pagesColorado Medical Board Policy Guidelines Pertaining To The Release and Retention of Medical Records Policy Number 40-07Brian HarrisNo ratings yet
- 42 CFR Part 8 Opioid Drugs in Maintenance and Detoxification Treatment of Opiate Addiction Final RuleDocument28 pages42 CFR Part 8 Opioid Drugs in Maintenance and Detoxification Treatment of Opiate Addiction Final RuleBrian HarrisNo ratings yet
- The DEA Position On MarijuanaDocument63 pagesThe DEA Position On MarijuanaBrian HarrisNo ratings yet
- Alcohol and Drug Abuse Division (ADAD) Substance Use Disorder Treatment Rules Colorado DHSDocument80 pagesAlcohol and Drug Abuse Division (ADAD) Substance Use Disorder Treatment Rules Colorado DHSBrian HarrisNo ratings yet
- State Board of Pharmacy Rules, Effective January 1, 2013Document176 pagesState Board of Pharmacy Rules, Effective January 1, 2013Brian HarrisNo ratings yet
- State Board of Pharmacy Rules, Effective January 1, 2013Document176 pagesState Board of Pharmacy Rules, Effective January 1, 2013Brian HarrisNo ratings yet
- Seventh Annual Report of Colorado State Methamphetamine Task Force (2013)Document21 pagesSeventh Annual Report of Colorado State Methamphetamine Task Force (2013)Brian HarrisNo ratings yet
- State of Colorado Board of Pharmacy Rules 3 CCR 719-1Document178 pagesState of Colorado Board of Pharmacy Rules 3 CCR 719-1Brian Harris100% (1)
- Debilitating Medical ConditionsDocument1 pageDebilitating Medical ConditionsBrian HarrisNo ratings yet
- Disinfection Cabinet and Insect KillersDocument4 pagesDisinfection Cabinet and Insect Killerssathya moorthy KamakottiNo ratings yet
- Railway Recruitment Board SiliguriDocument9 pagesRailway Recruitment Board SiliguripranavsircarNo ratings yet
- Death of A Salesman by Arthur MillerDocument125 pagesDeath of A Salesman by Arthur MillerNaman VasalNo ratings yet
- Sist TS Cen TS 17091 2018Document11 pagesSist TS Cen TS 17091 2018سعد خضر الياسNo ratings yet
- Oracle Certified Professional Java Programmer (OCPJP 7) BookDocument38 pagesOracle Certified Professional Java Programmer (OCPJP 7) BookDhivya Ganesh100% (2)
- Bill Sahli - Mind Becomes MassDocument76 pagesBill Sahli - Mind Becomes MassIvan TaranovNo ratings yet
- Et Annual Report 04 05Document48 pagesEt Annual Report 04 05Pavlo Andre AbiyNo ratings yet
- Ebiz Steps PDFDocument59 pagesEbiz Steps PDFBathina Srinivasa RaoNo ratings yet
- First Quarterly Assessment Intle7: School Year 2021-2022Document3 pagesFirst Quarterly Assessment Intle7: School Year 2021-2022marjorie rochaNo ratings yet
- Hydrogen EconomyDocument19 pagesHydrogen EconomyEdgar Gabriel Sanchez DominguezNo ratings yet
- The Silt Verses - Chapter 21 TranscriptDocument32 pagesThe Silt Verses - Chapter 21 TranscriptVictória MoraesNo ratings yet
- Stressed Syllable, While Free Vowels Are Those That May Stand in A Stressed Open Syllable With No Following ConsonantDocument2 pagesStressed Syllable, While Free Vowels Are Those That May Stand in A Stressed Open Syllable With No Following ConsonantResiNo ratings yet
- The Filipino EmpanadaDocument2 pagesThe Filipino EmpanadaMaria Lourdez Bayan100% (3)
- 3 Asch - The Metaphor - 1958Document10 pages3 Asch - The Metaphor - 1958Aysen Ece BörkNo ratings yet
- ABC - Suggested Answer - 0Document8 pagesABC - Suggested Answer - 0pam pamNo ratings yet
- Primary School Planner Second Year of English: 11 - 20 WordsearchDocument0 pagesPrimary School Planner Second Year of English: 11 - 20 WordsearchJunaidi HamdiNo ratings yet
- Lesson 1 - Plumbing MaterialsDocument18 pagesLesson 1 - Plumbing MaterialsNicholas Bonn SingNo ratings yet
- Canadian Soil Quality Guidelines For The Protection of Environmental and Human Health Uranium 2007Document14 pagesCanadian Soil Quality Guidelines For The Protection of Environmental and Human Health Uranium 2007njcojann_co901745No ratings yet
- VarahamihiraDocument6 pagesVarahamihiraSTAR GROUPS100% (1)
- Summary 6ugfg4xf 54jdkatjDocument16 pagesSummary 6ugfg4xf 54jdkatjsaritabasnet916No ratings yet
- Anh Văn Chuyên NgànhDocument7 pagesAnh Văn Chuyên Ngành19150004No ratings yet
- Nokia: Management of SmesDocument32 pagesNokia: Management of SmesSimone SantosNo ratings yet
- Near Source Fault Effects On The Performance of Base-Isolated Hospital Building vs. A BRBF Hospital BuildingDocument6 pagesNear Source Fault Effects On The Performance of Base-Isolated Hospital Building vs. A BRBF Hospital BuildingJosé Antonio Alarcón LeónNo ratings yet
- TTD Series Configurable Fault AnnunciatorDocument4 pagesTTD Series Configurable Fault AnnunciatorAlejandroMuñozNo ratings yet
- Advancement ProposalDocument2 pagesAdvancement ProposalJEFFERSON GOMEZNo ratings yet