Download as pdf or txt
You might also like
- Sports Psychology for Athletes 2.0: Develop a Champion Mindset and Train for Optimal PerformanceFrom EverandSports Psychology for Athletes 2.0: Develop a Champion Mindset and Train for Optimal PerformanceNo ratings yet
- Medical History Physical FormDocument2 pagesMedical History Physical Formapi-69208402No ratings yet
- Brain InjuryDocument50 pagesBrain InjuryMuhammad Abdul RahmanNo ratings yet
- PhysicalDocument7 pagesPhysicalapi-315046090No ratings yet
- Piaa FormDocument9 pagesPiaa Formapi-325520279No ratings yet
- Child Abuse - PhysicalDocument3 pagesChild Abuse - PhysicalIsabella GomezNo ratings yet
- 2014 A Parent's Guide To ConcussionDocument5 pages2014 A Parent's Guide To ConcussionAngela CarterNo ratings yet
- Chisjh Sports Medicine Injury Evaluation WorkbookDocument16 pagesChisjh Sports Medicine Injury Evaluation Workbookyiy yuyNo ratings yet
- SEX Date of Birth: Allergies Regular Medications: Medical ConditionsDocument2 pagesSEX Date of Birth: Allergies Regular Medications: Medical Conditionsapi-284837640No ratings yet
- Concussion: Information and Signature Form For Student-Athletes & Parents/Legal GuardiansDocument3 pagesConcussion: Information and Signature Form For Student-Athletes & Parents/Legal Guardianscrock1615No ratings yet
- Sports Safety Website 7-28Document3 pagesSports Safety Website 7-28api-258374959No ratings yet
- Uhsaa B Form 2011Document3 pagesUhsaa B Form 2011Lisa WillardsonNo ratings yet
- Concussion Management Protocols: Cynthia Dilaura Devore, M.D., M.A., M.S., F.A.A.PDocument25 pagesConcussion Management Protocols: Cynthia Dilaura Devore, M.D., M.A., M.S., F.A.A.PkitsilcNo ratings yet
- Homework With A ConcussionDocument5 pagesHomework With A Concussionafetmagzj100% (1)
- Learners Record BookDocument11 pagesLearners Record BookMarjhun Flores GuingayanNo ratings yet
- Concussions in SportsDocument5 pagesConcussions in Sportsapi-231143197No ratings yet
- 2012 Returners Paperwork PacketDocument14 pages2012 Returners Paperwork Packetapi-151470460No ratings yet
- College of Liberal Arts, Sciences, and Education: The Physical Activity Readiness Questionnaire (PAR-Q)Document2 pagesCollege of Liberal Arts, Sciences, and Education: The Physical Activity Readiness Questionnaire (PAR-Q)Jello UcagNo ratings yet
- Self Report MedicationDocument3 pagesSelf Report MedicationMarjhun Flores GuingayanNo ratings yet
- Fulbright Certificate of HealthDocument8 pagesFulbright Certificate of HealthLinda Klimavicius100% (1)
- IqcodeDocument4 pagesIqcodeBilly ChandraNo ratings yet
- Can You Do Homework With A ConcussionDocument4 pagesCan You Do Homework With A Concussionafnkazmquziwrf100% (1)
- Form A: Use This Form For Initial Physical ExamDocument4 pagesForm A: Use This Form For Initial Physical ExamLisa WillardsonNo ratings yet
- Center For BrainHealthDocument5 pagesCenter For BrainHealthJames KuhnNo ratings yet
- 2324 ISA Athletic Forms-2Document5 pages2324 ISA Athletic Forms-2gavin.carlos.guNo ratings yet
- Name Home Address Phone Grade Sports Personal Physician Physician's Phone Number Date of Birth Sex SchoolDocument2 pagesName Home Address Phone Grade Sports Personal Physician Physician's Phone Number Date of Birth Sex SchoolCarmen SniderNo ratings yet
- Howard County [Md] Public Schools Athletic Director Annual Report to Bd of Ed, Re High School Sports Program p. 15 Concussion Stats by Sport p. 14 Limit on In-season Football Contact Practices to 2 Per WeekDocument15 pagesHoward County [Md] Public Schools Athletic Director Annual Report to Bd of Ed, Re High School Sports Program p. 15 Concussion Stats by Sport p. 14 Limit on In-season Football Contact Practices to 2 Per WeekConcussion_MCPS_MdNo ratings yet
- Department of State Academic Exchanges Participant Medical History and Examination FormDocument8 pagesDepartment of State Academic Exchanges Participant Medical History and Examination FormNurman HidayatNo ratings yet
- UHSAA Preparticipation FormDocument4 pagesUHSAA Preparticipation FormThe Salt Lake TribuneNo ratings yet
- Parq EditedDocument2 pagesParq EditedJay Ann AgarradoNo ratings yet
- 2021 Health QuestionnaireDocument3 pages2021 Health Questionnairemilksheikh2004No ratings yet
- 2012 Newcomers Paperwork PacketDocument15 pages2012 Newcomers Paperwork Packetapi-151470460No ratings yet
- Appendix A - FDocument54 pagesAppendix A - Fbakson college gr. noidaNo ratings yet
- Marietta City Schools' Athletic Physical, Insurance, and Consent FormDocument6 pagesMarietta City Schools' Athletic Physical, Insurance, and Consent FormPatavious SorrellNo ratings yet
- Instructions and Information For Completing The Evidence of Insurability FormDocument6 pagesInstructions and Information For Completing The Evidence of Insurability FormnzomniacNo ratings yet
- Concussion SmartphoneDocument6 pagesConcussion SmartphoneQurat-Ul-Aan WasimNo ratings yet
- Mental IllnessDocument2 pagesMental Illnesshavana1975No ratings yet
- Pshycology Mid Term PaperDocument17 pagesPshycology Mid Term PaperDaniyal ArifNo ratings yet
- Medical NarrativeDocument3 pagesMedical NarrativeJennessee MiagueNo ratings yet
- Day Camp Registration 12Document1 pageDay Camp Registration 12Redeemer Lutheran SchoolNo ratings yet
- School Participant FormDocument4 pagesSchool Participant FormJennifer CervelleraNo ratings yet
- M R C A P M: How Did You Hear About This Office?Document7 pagesM R C A P M: How Did You Hear About This Office?summitmediacorpNo ratings yet
- Neurotrauma Pediatric ScalesDocument16 pagesNeurotrauma Pediatric ScalesYudha Perwira PutraNo ratings yet
- Clearance For Safe Exercise Participation: I. Health HistoryDocument3 pagesClearance For Safe Exercise Participation: I. Health HistoryejjohnsoNo ratings yet
- PE11 Q3 Module 1 Weeks 1 2Document12 pagesPE11 Q3 Module 1 Weeks 1 2Jose Ruel Rosello Mendoza100% (1)
- Occupational Health QuestionnaireDocument13 pagesOccupational Health QuestionnaireMohamed HafezNo ratings yet
- Physical Assessment - Specifics On General ObservationsDocument14 pagesPhysical Assessment - Specifics On General ObservationsJennifer B. GarciaNo ratings yet
- Physical Form ADocument4 pagesPhysical Form Aapi-3958058100% (1)
- Assessment Done Prior To FitnessDocument15 pagesAssessment Done Prior To FitnessAditya SharmaNo ratings yet
- Nternational Chool Anila: STUDENT ID# - Please Print The Information Requested BelowDocument4 pagesNternational Chool Anila: STUDENT ID# - Please Print The Information Requested Belowainsleydevilla8079No ratings yet
- Senior Project PaperDocument8 pagesSenior Project Paperapi-285189408100% (1)
- Hockey Concussions Are Serious BusinessDocument9 pagesHockey Concussions Are Serious BusinessMyraNo ratings yet
- MDA Medical FormDocument5 pagesMDA Medical FormsofiablegerNo ratings yet
- FC Back To Sports Meeting Presentation Slides and Script With Video UCM - 490125Document53 pagesFC Back To Sports Meeting Presentation Slides and Script With Video UCM - 490125redaNo ratings yet
- Health FormsDocument5 pagesHealth FormsBianca Louise SengcoNo ratings yet
- Concussion Training For CoachesDocument8 pagesConcussion Training For Coachescharger1234No ratings yet
- Peak Performance: How to Think, Train and Eat for Optimal PerformanceFrom EverandPeak Performance: How to Think, Train and Eat for Optimal PerformanceRating: 3.5 out of 5 stars3.5/5 (2)
- Keto Fitness 2.0: How to Think, Eat and Train for Optimal PerformanceFrom EverandKeto Fitness 2.0: How to Think, Eat and Train for Optimal PerformanceNo ratings yet
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- Therapeutic Activities for Children and Teens Coping with Health IssuesFrom EverandTherapeutic Activities for Children and Teens Coping with Health IssuesNo ratings yet
- Parent Letter To MCPS Re Student Injury Data - 01-14-2015Document11 pagesParent Letter To MCPS Re Student Injury Data - 01-14-2015Concussion_MCPS_MdNo ratings yet
- MCPS Sports Concussion Data 2014-15Document1 pageMCPS Sports Concussion Data 2014-15Concussion_MCPS_MdNo ratings yet
- NFL 2010 Letter Re Concussion LegDocument2 pagesNFL 2010 Letter Re Concussion LegConcussion_MCPS_MdNo ratings yet
- Brain Sentry Inova Football Helmet Sensor Research Study ProposalDocument5 pagesBrain Sentry Inova Football Helmet Sensor Research Study ProposalConcussion_MCPS_MdNo ratings yet
- MCPS (MD) Tobacco-Free SCH PolicyDocument2 pagesMCPS (MD) Tobacco-Free SCH PolicyConcussion_MCPS_MdNo ratings yet
- Template 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Document1 pageTemplate 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Concussion_MCPS_MdNo ratings yet
- MCPS Student Injury Report FormDocument2 pagesMCPS Student Injury Report FormConcussion_MCPS_MdNo ratings yet
- MD Bill - HS Football Helmet Sensor Pilot ProgramDocument6 pagesMD Bill - HS Football Helmet Sensor Pilot ProgramConcussion_MCPS_MdNo ratings yet
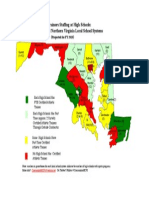
- Projected Ath Trainer HS Staffing in FY 2015-Map of MD and N. VA CountiesDocument1 pageProjected Ath Trainer HS Staffing in FY 2015-Map of MD and N. VA CountiesConcussion_MCPS_MdNo ratings yet
- REHAB Basel EnglischDocument2 pagesREHAB Basel EnglischMara BujorNo ratings yet
- Stephanie Hall - Grief PowerpointDocument22 pagesStephanie Hall - Grief PowerpointricciardettoNo ratings yet
- Physio Ex Lab 3 Part 1 Key - PDF SGD2Document5 pagesPhysio Ex Lab 3 Part 1 Key - PDF SGD2Kia G. EstavilloNo ratings yet
- Effect of Transcutaneous Electrical Nerve Stimulation On Spasticity in Adults With Stroke A Syst Review and Metaanalysis PDFDocument18 pagesEffect of Transcutaneous Electrical Nerve Stimulation On Spasticity in Adults With Stroke A Syst Review and Metaanalysis PDFjaunasvyras69 Jaunasvyras69No ratings yet
- Art and Science CollaborationDocument52 pagesArt and Science CollaborationderghalNo ratings yet
- Impaired Verbal CommunicationDocument2 pagesImpaired Verbal CommunicationMart AlunanNo ratings yet
- Lior Tiroshi CVDocument3 pagesLior Tiroshi CVapi-495268203No ratings yet
- Assignment#3Document3 pagesAssignment#3savitaannu07No ratings yet
- Cerebral Salt Wasting Syndrome - StatPearls - NCBI BookshelfDocument4 pagesCerebral Salt Wasting Syndrome - StatPearls - NCBI BookshelfOnggo WiliyantoNo ratings yet
- Occupational Therapy Ia Sample ReportsDocument11 pagesOccupational Therapy Ia Sample Reportssneha duttaNo ratings yet
- Anesthesia in DentistryDocument47 pagesAnesthesia in DentistryKennet CruzNo ratings yet
- Dozois 5e Chapter02 TIFDocument31 pagesDozois 5e Chapter02 TIFrebeccaNo ratings yet
- Antipsychotic Drugs: Conventional AntipsychoticsDocument16 pagesAntipsychotic Drugs: Conventional AntipsychoticsApple MaeNo ratings yet
- Human and Social Biology 5096 GCE O Level For Examination in 2008Document26 pagesHuman and Social Biology 5096 GCE O Level For Examination in 2008mstudy123456No ratings yet
- Neurogenic ShockDocument11 pagesNeurogenic Shocklulu voxNo ratings yet
- Jamaotolaryngology Lee 2020 Oi 190100Document7 pagesJamaotolaryngology Lee 2020 Oi 190100LeonNo ratings yet
- Physical Therapy Neuroscience Central Somatosensory Lecture POSTDocument43 pagesPhysical Therapy Neuroscience Central Somatosensory Lecture POSTashlyn granthamNo ratings yet
- THT Gambaran MTDocument109 pagesTHT Gambaran MTCindy RiannieNo ratings yet
- Biomechanical Basis of Traumatic Brain InjuryDocument32 pagesBiomechanical Basis of Traumatic Brain InjuryPutu AnantaNo ratings yet
- Basic Approch To CT BrainDocument62 pagesBasic Approch To CT BrainS B SayedNo ratings yet
- DrawittoknowitDocument2 pagesDrawittoknowitByeongsu ParkNo ratings yet
- A Trip I Will Never ForgetDocument1 pageA Trip I Will Never ForgetIuliana ȚigănașuNo ratings yet
- Angelman Syndrome: A Genetic Disorder Falcunilitin, Kirby Maravilla, Eunice MoureenDocument11 pagesAngelman Syndrome: A Genetic Disorder Falcunilitin, Kirby Maravilla, Eunice MoureenEunice Moureen MaravillaNo ratings yet
- Neuro AssessmentDocument6 pagesNeuro AssessmentKabilan RNo ratings yet
- C) Slow + Fast ComponentsDocument7 pagesC) Slow + Fast ComponentsUzair KhanNo ratings yet
- HeadacheDocument277 pagesHeadacheUlquiorra SchifferNo ratings yet
- MbbsDocument162 pagesMbbsKanwalAslam100% (1)
- Paediatrics 30 McQsDocument10 pagesPaediatrics 30 McQsRatan YadavNo ratings yet
- Anxiety DisordersDocument42 pagesAnxiety DisordersHazel Marie EchavezNo ratings yet
- نسخة Lecture - PAIN Assessment & ManagementDocument52 pagesنسخة Lecture - PAIN Assessment & Managementjsoal100% (1)


























![Howard County [Md] Public Schools
Athletic Director Annual Report to Bd of Ed,
Re High School Sports Program
p. 15 Concussion Stats by Sport
p. 14 Limit on In-season Football Contact Practices to 2 Per Week](https://imgv2-1-f.scribdassets.com/img/document/124077961/149x198/5a472ee067/1360115263?v=1)