Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Ebook On Feed Formulation EbookDocument17 pagesEbook On Feed Formulation EbookDada RasheedNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Gangaram Rate List PDFDocument315 pagesGangaram Rate List PDFAmit Kumar GuptaNo ratings yet
- CH 02Document9 pagesCH 02Akash Thummar100% (2)
- 2014 Animal Feeds Formulation Training - 18-03-2014Document1 page2014 Animal Feeds Formulation Training - 18-03-2014Eddy Mwachenje100% (1)
- 2011 Opel Corsa 53003Document218 pages2011 Opel Corsa 53003Alina RogojanuNo ratings yet
- PhysicsDocument2 pagesPhysicsAlina RogojanuNo ratings yet
- PROGRAM - DETAILAT Conferinta Bioinginerie 2015 PDFDocument41 pagesPROGRAM - DETAILAT Conferinta Bioinginerie 2015 PDFAlina RogojanuNo ratings yet
- Irelands West CoastDocument36 pagesIrelands West CoastAlina RogojanuNo ratings yet
- Evaluation of Image Quality Parameters of Representative Intraoral Radiographic SystemsDocument10 pagesEvaluation of Image Quality Parameters of Representative Intraoral Radiographic SystemsAlina RogojanuNo ratings yet
- Radiation Therapy ICRUDocument1 pageRadiation Therapy ICRUAlina RogojanuNo ratings yet
- Imaging Quality Assurance Manual: - Revision 13 Dated 10/25/2013Document102 pagesImaging Quality Assurance Manual: - Revision 13 Dated 10/25/2013Alina RogojanuNo ratings yet
- Infrared SpectrosDocument38 pagesInfrared Spectrosfazraz100% (11)
- Reina Bridge2Document7 pagesReina Bridge2Phil StiltonNo ratings yet
- Incozol 4 TDSDocument1 pageIncozol 4 TDSsriatul2006No ratings yet
- Physics Student Safety ContractDocument3 pagesPhysics Student Safety ContractJdeen FajardoNo ratings yet
- Beyblade GDocument50 pagesBeyblade GRealmZeldaNo ratings yet
- Binocular Vision ScheimanDocument732 pagesBinocular Vision ScheimanOptom Dang100% (1)
- Mother's Day Differentiated Reading Comprehension ActivityDocument11 pagesMother's Day Differentiated Reading Comprehension ActivityKannybell BelleNo ratings yet
- Makahiya (Mimosa Pudica) Extract: Its Potential Efficiency in Decreasing The Blood Sugar LevelDocument10 pagesMakahiya (Mimosa Pudica) Extract: Its Potential Efficiency in Decreasing The Blood Sugar LevelJaneNo ratings yet
- Evening Street Review Number 36Document306 pagesEvening Street Review Number 36Barbara BergmannNo ratings yet
- Anticancer Activity of Medicinal Plants ThesisDocument7 pagesAnticancer Activity of Medicinal Plants Thesislbbzfoxff100% (2)
- Autism - Developmental-History-FormDocument12 pagesAutism - Developmental-History-Formmemphisosiris0No ratings yet
- Axial Piston Closed Circuit Pumps: Series 42Document76 pagesAxial Piston Closed Circuit Pumps: Series 42Евгений ГубаревNo ratings yet
- Lesson 3Document21 pagesLesson 3Carylle Shayne MarcellanaNo ratings yet
- Resonance Kvpy ChemistryDocument117 pagesResonance Kvpy ChemistryHarish MahadevanNo ratings yet
- Dish Id RosisDocument28 pagesDish Id RosisDM internaNo ratings yet
- Sustainability 14 07022 v2Document22 pagesSustainability 14 07022 v2Osman DenizNo ratings yet
- LeaP Science G7 Week 3 Q4 - JPSDocument7 pagesLeaP Science G7 Week 3 Q4 - JPSEdralyn PaduaNo ratings yet
- Introductory Topics HandoutDocument43 pagesIntroductory Topics HandoutGGuillorn100% (1)
- NMDs OrientationDocument31 pagesNMDs OrientationRasheedAladdinNGuiomalaNo ratings yet
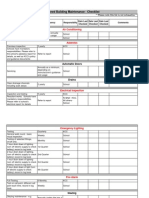
- Building Maintenance ChecklistDocument5 pagesBuilding Maintenance ChecklistcajaroNo ratings yet
- Advanced Nursing AdministrationDocument5 pagesAdvanced Nursing AdministrationProvidence MuswizuNo ratings yet
- Anatomical Terminology 2Document63 pagesAnatomical Terminology 2blackamir385No ratings yet
- Case Presentatio Insomnia 1Document49 pagesCase Presentatio Insomnia 1kiran mahal100% (1)
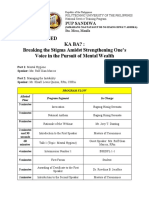
- Open-Minded Ka Ba?: Breaking The Stigma Amidst Strengthening One's Voice in The Pursuit of Mental WealthDocument3 pagesOpen-Minded Ka Ba?: Breaking The Stigma Amidst Strengthening One's Voice in The Pursuit of Mental WealthEstrada JulianeNo ratings yet
- Agilent Application Note HILIC Column BetaineDocument2 pagesAgilent Application Note HILIC Column BetainePrashant GaurNo ratings yet
- Dde 650Document1 pageDde 650aertibraNo ratings yet
- A 26 V 14 N 02Document6 pagesA 26 V 14 N 02faustinopateiro3497No ratings yet