Download as pdf or txt
You might also like
- AWWA-AWWA Standard C530-12 Pilot Operated Control Valves-American Water Works Association (2012)Document32 pagesAWWA-AWWA Standard C530-12 Pilot Operated Control Valves-American Water Works Association (2012)virtech100% (1)
- An Update On Ultrasonic Irrigant ActivationDocument15 pagesAn Update On Ultrasonic Irrigant ActivationkarishmaNo ratings yet
- Maytag MFR40 - MFR50PD SpecificationsDocument2 pagesMaytag MFR40 - MFR50PD Specificationsmairimsp2003No ratings yet
- The Characterization of Acoustic Cavitation Bubbles - An OverviewDocument9 pagesThe Characterization of Acoustic Cavitation Bubbles - An Overview劉平本No ratings yet
- Power Toothbrushes: A Critical Review: C PenickDocument5 pagesPower Toothbrushes: A Critical Review: C PenickEltonJCSilveiraNo ratings yet
- Land ClearingDocument9 pagesLand ClearingAzmi Fauzi100% (2)
- Ef Cacy of Sonically, Ultrasonically Andlaser-Activated Irrigation in Removing Abio Lm-Mimicking Hydrogel From An Isthmus ModelDocument9 pagesEf Cacy of Sonically, Ultrasonically Andlaser-Activated Irrigation in Removing Abio Lm-Mimicking Hydrogel From An Isthmus ModelBenjiNo ratings yet
- Liquid Processing CatalogDocument31 pagesLiquid Processing CatalogLina Maria RodriguezNo ratings yet
- Catalogue - Probe Sonicator - Ultra Autosonic IndiaDocument4 pagesCatalogue - Probe Sonicator - Ultra Autosonic IndiaGirish GuptaNo ratings yet
- Ultrasonic Cleaning - Fundamental Theory and Application CTG Clean PDFDocument12 pagesUltrasonic Cleaning - Fundamental Theory and Application CTG Clean PDFMusunuri Ratna TejaNo ratings yet
- SlidesDocument169 pagesSlidesAndrew Coleman100% (2)
- Computer-Controlled Sophisticated Ultrasonic Cleaner: H. Muthurajan, H.H. Kumar, and D.K. KharatDocument4 pagesComputer-Controlled Sophisticated Ultrasonic Cleaner: H. Muthurajan, H.H. Kumar, and D.K. KharatNKJemesNo ratings yet
- Sonication From Wikipedia, The Free Encyclopedia: UltrasonicDocument4 pagesSonication From Wikipedia, The Free Encyclopedia: UltrasonicJimmyNo ratings yet
- Underwater Laser Micromachining of Silicon in Pressurized EnvironmentDocument9 pagesUnderwater Laser Micromachining of Silicon in Pressurized Environmentসুহাস মন্ডলNo ratings yet
- Ultrasonic Assisted Underwater Laser Micromachining of SiliconDocument29 pagesUltrasonic Assisted Underwater Laser Micromachining of SiliconBLACK SABBATHNo ratings yet
- Diffraction by Ultrasonic Waves in LiquidDocument5 pagesDiffraction by Ultrasonic Waves in LiquidParmanandaNo ratings yet
- VASCHE AD ULTRASUONI GB LowDocument16 pagesVASCHE AD ULTRASUONI GB Lowkaka punNo ratings yet
- Resonance UnlockedDocument5 pagesResonance UnlockedgjjgNo ratings yet
- Review of Ultrasonic Irrigation in Endodontics Increasing Action of Irrigating SolutionsDocument10 pagesReview of Ultrasonic Irrigation in Endodontics Increasing Action of Irrigating SolutionsayoubNo ratings yet
- Dental Health CavitationDocument3 pagesDental Health CavitationAyu Pujiwati100% (1)
- Acoustic Microbubble Dynamics With Viscous Effects 2016Document10 pagesAcoustic Microbubble Dynamics With Viscous Effects 2016Kawa Mustafa AzizNo ratings yet
- Wave Motion PDFDocument23 pagesWave Motion PDFFRANCES VISAYA100% (1)
- Photo Accoustic ImagineDocument7 pagesPhoto Accoustic ImagineArpan MannaNo ratings yet
- Acoustic Cavitation Field Prediction at Low and High Frequency UltrasoundsDocument7 pagesAcoustic Cavitation Field Prediction at Low and High Frequency UltrasoundsHamza FerkousNo ratings yet
- 5.3 Ultrasonics in EndoDocument23 pages5.3 Ultrasonics in EndoRevathy M NairNo ratings yet
- Introduction To Magnetic CircuitsDocument23 pagesIntroduction To Magnetic Circuitssharad kumarNo ratings yet
- Chapter 3: Electrolytic Conductance 3.1. Specific Conductance Specific Conductance Is A Measure of The Electric Current in The Water SampledDocument11 pagesChapter 3: Electrolytic Conductance 3.1. Specific Conductance Specific Conductance Is A Measure of The Electric Current in The Water SampledBùi Hữu ĐứcNo ratings yet
- Infection Prevention Using Sterelization MethodsDocument42 pagesInfection Prevention Using Sterelization MethodsAliyu NasirNo ratings yet
- Computing CapacitanceDocument16 pagesComputing Capacitancepraveeng11100% (1)
- Advanced Cavitation Institute Alternative Energy NanotechnologyDocument18 pagesAdvanced Cavitation Institute Alternative Energy NanotechnologyVincent J. CataldiNo ratings yet
- CavitationDocument12 pagesCavitationVarun Vikram SinghNo ratings yet
- Ultrasonic Cleaning NoteDocument4 pagesUltrasonic Cleaning NoteRKMNo ratings yet
- Resonance of A Closed Air ColumnDocument11 pagesResonance of A Closed Air ColumnHo Ping100% (6)
- Dental PricingDocument4 pagesDental PricingsolutionbeautyNo ratings yet
- Articulo de Crown DownDocument13 pagesArticulo de Crown DownLaura DanielaNo ratings yet
- "3Mix-MP in Endodontics - An Overview": Varalakshmi R Parasuraman MDS, Banker Sharadchandra Muljibhai MDSDocument10 pages"3Mix-MP in Endodontics - An Overview": Varalakshmi R Parasuraman MDS, Banker Sharadchandra Muljibhai MDSFirma Nurdinia DewiNo ratings yet
- Cracked Tooth SyndromeDocument4 pagesCracked Tooth SyndromeANUBHANo ratings yet
- Op Calcium HydroxideDocument1 pageOp Calcium HydroxideFaizal Prabowo KalimanNo ratings yet
- Present Status and Future Directions of Intracanal MedicamentsDocument24 pagesPresent Status and Future Directions of Intracanal MedicamentsJavier VillalobosNo ratings yet
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDocument6 pagesNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaNo ratings yet
- Traumatic Injuries of The Tooth / Orthodontic Courses by Indian Dental AcademyDocument43 pagesTraumatic Injuries of The Tooth / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Acne Grading Guideline (Group 17)Document3 pagesAcne Grading Guideline (Group 17)Jennifer MartindocNo ratings yet
- Basics of DOM FINALDocument32 pagesBasics of DOM FINALachsah johnsonNo ratings yet
- Surface Decontamination Protocols For Surgical Treatment of Peri-Implantitis A Systematic Review With Meta-AnalysisDocument18 pagesSurface Decontamination Protocols For Surgical Treatment of Peri-Implantitis A Systematic Review With Meta-Analysiskaue franco100% (1)
- "Endodontic Sealers": Current Concepts and Comparative Analysis ReviewDocument6 pages"Endodontic Sealers": Current Concepts and Comparative Analysis ReviewAlina TomaNo ratings yet
- Irrigation Needle StandardizationDocument7 pagesIrrigation Needle StandardizationEmilio González Polar MesíaNo ratings yet
- Fundamentals of Ultrasonics PDFDocument6 pagesFundamentals of Ultrasonics PDFMahima TyagiNo ratings yet
- An Improved Direct InjectionDocument8 pagesAn Improved Direct InjectionJuan Francisco CamposNo ratings yet
- Modern Pumping - 052014Document60 pagesModern Pumping - 052014anjangandak2932No ratings yet
- Comenda AcrsDocument10 pagesComenda Acrso.m.martin81gmail.comNo ratings yet
- Cavitator FE EngineeringDocument2 pagesCavitator FE Engineeringstev_zoranNo ratings yet
- Role of Artificial Intelligence in ProsthodonticsDocument7 pagesRole of Artificial Intelligence in ProsthodonticsIJAR JOURNALNo ratings yet
- DT Mar 15 NPR Buchanan FNLDocument10 pagesDT Mar 15 NPR Buchanan FNLKranti PrajapatiNo ratings yet
- 3 - Guideline Energy Efficiency in The Confectionery IndustryDocument12 pages3 - Guideline Energy Efficiency in The Confectionery IndustryNasional GotongroyongNo ratings yet
- The Use of Ultrasound To Mitigate Membrane Fouling in Desalination and Water TreatmentDocument61 pagesThe Use of Ultrasound To Mitigate Membrane Fouling in Desalination and Water TreatmentFatma Al BelushiNo ratings yet
- Pasta TripleDocument7 pagesPasta TripleLincoln GarciaNo ratings yet
- Plaque ConDocument31 pagesPlaque ConKruti PatelNo ratings yet
- Manual Vs ElectricDocument5 pagesManual Vs ElectricnasyaNo ratings yet
- G06052938 PDFDocument10 pagesG06052938 PDFSiti Fatimah Khaerun NisaNo ratings yet
- A Review On Toothbrushes and Tooth Brushing MethodsDocument10 pagesA Review On Toothbrushes and Tooth Brushing MethodsinventionjournalsNo ratings yet
- M K J M. G E C R A C - V C. R G A: Purpose: To Compare The Efficacy of An Oscillating-Rotating Power Toothbrush With A Novel Brush HeadDocument6 pagesM K J M. G E C R A C - V C. R G A: Purpose: To Compare The Efficacy of An Oscillating-Rotating Power Toothbrush With A Novel Brush HeadAdam SweidanNo ratings yet
- Your Path to Healthier Dentistry: A Holistic Approach to Keeping Your Teeth for a LifetimeFrom EverandYour Path to Healthier Dentistry: A Holistic Approach to Keeping Your Teeth for a LifetimeRating: 5 out of 5 stars5/5 (1)
- Oral Mucous MembraneDocument71 pagesOral Mucous MembraneHarleen GrewalNo ratings yet
- Alveolar BoneDocument78 pagesAlveolar BoneHarleen GrewalNo ratings yet
- Abstract For Er. Yag ReviewDocument1 pageAbstract For Er. Yag ReviewHarleen GrewalNo ratings yet
- Department of Periodontology and Oral Implantology National Dental College and Hospital DerabassiDocument2 pagesDepartment of Periodontology and Oral Implantology National Dental College and Hospital DerabassiHarleen GrewalNo ratings yet
- Anti TB Hospital DaskaDocument11 pagesAnti TB Hospital DaskaWaqas ShamshadNo ratings yet
- DR - Nitish Kumar - CV ..Document6 pagesDR - Nitish Kumar - CV ..ABHISHEK SINGHNo ratings yet
- Homestay Application FormDocument4 pagesHomestay Application FormlazikotoshpulatovaNo ratings yet
- Research ProjectDocument37 pagesResearch ProjectSurya DodveNo ratings yet
- FRB13089887411Document4 pagesFRB13089887411MAHA KAALNo ratings yet
- S80 2007 Wiring SupplementDocument109 pagesS80 2007 Wiring Supplementjstdoma /No ratings yet
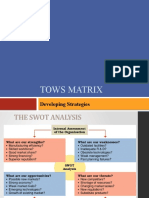
- Tows Matrix: Developing StrategiesDocument29 pagesTows Matrix: Developing StrategiesalkalkiaNo ratings yet
- Application of IntegralsDocument14 pagesApplication of IntegralsSanjayNo ratings yet
- 1454665129905-MNRE Empanelled Agency-All India PDFDocument25 pages1454665129905-MNRE Empanelled Agency-All India PDFAurobindo SaxenaNo ratings yet
- ASON SLA Classification of ServicesDocument6 pagesASON SLA Classification of ServicesWondale KebedeNo ratings yet
- Inv - 1124003027 - Po - 407097662 - VR - 407097662 - (Top Synthetic Rubber)Document1 pageInv - 1124003027 - Po - 407097662 - VR - 407097662 - (Top Synthetic Rubber)shamirah98No ratings yet
- Kuratko 8 e CH 13Document36 pagesKuratko 8 e CH 13waqasNo ratings yet
- Poliomyelitis: By: Reema I. DabbasDocument35 pagesPoliomyelitis: By: Reema I. DabbasReema DabbasNo ratings yet
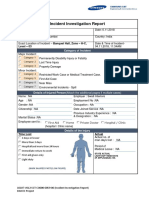
- Incident Investigation Report - Fire Incedent - 04-11-2018 Swati InteriorsDocument4 pagesIncident Investigation Report - Fire Incedent - 04-11-2018 Swati InteriorsMobin Thomas AbrahamNo ratings yet
- SOAP Notes: HistoryDocument5 pagesSOAP Notes: HistoryRajveerNo ratings yet
- Ae tt1021 Grammar Worksheet 18Document1 pageAe tt1021 Grammar Worksheet 18Carmen TeixeiraNo ratings yet
- Thesis Format Iit KanpurDocument7 pagesThesis Format Iit Kanpurvictoriathompsonaustin100% (2)
- The Hubbard Energy Transformer by Gaston Burridge, Fate Magazine 1956Document24 pagesThe Hubbard Energy Transformer by Gaston Burridge, Fate Magazine 1956pplowe2305tedNo ratings yet
- Carbon-Based Molecules Are The Foundation of Life.: Key ConceptDocument17 pagesCarbon-Based Molecules Are The Foundation of Life.: Key ConceptNoN -NaNo ratings yet
- CHE2871 Biochemistry For EngineersDocument2 pagesCHE2871 Biochemistry For EngineersBlue JunNo ratings yet
- SOPs River Sand and Stone Mining ActivitiesDocument64 pagesSOPs River Sand and Stone Mining ActivitiesAliffIrhamMohdHashimNo ratings yet
- AHF Thesis - CorrectedDocument146 pagesAHF Thesis - CorrectedAlasdair FikourasNo ratings yet
- Instron Low Velocity Impact TesterDocument179 pagesInstron Low Velocity Impact TesterEmre GuneyNo ratings yet
- Department of Applied Physics Applied Physics Question Bank Session - 2012-13Document4 pagesDepartment of Applied Physics Applied Physics Question Bank Session - 2012-13Sajid Ur RehmanNo ratings yet
- Tagbino National High SchoolDocument2 pagesTagbino National High SchooldarelleNo ratings yet
- Honda City Vs Toyota CorollaDocument1 pageHonda City Vs Toyota CorollaMuhammad Sheharyar MohsinNo ratings yet
- Classification of HotelsDocument14 pagesClassification of HotelsJeevesh ViswambharanNo ratings yet
- Admission CriteriaDocument2 pagesAdmission CriteriaDr Vikas GuptaNo ratings yet