Download as pdf or txt
You might also like
- Eustachian Tube: Structure, Function, and Role in Middle-Ear Disease, 2eFrom EverandEustachian Tube: Structure, Function, and Role in Middle-Ear Disease, 2eNo ratings yet
- Family Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesDocument6 pagesFamily Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesAndrea Kristin OrigenesNo ratings yet
- #Complications of Suppurative Otitis MediaDocument8 pages#Complications of Suppurative Otitis MediaameerabestNo ratings yet
- Ryan Martin Ko, M.DDocument54 pagesRyan Martin Ko, M.DDhaval Makwana100% (2)
- #Disease of External EarDocument4 pages#Disease of External EarameerabestNo ratings yet
- External Ear DiseaseDocument60 pagesExternal Ear Diseasenitas23100% (1)
- Otitis MediaDocument8 pagesOtitis MediamuhammadridhwanNo ratings yet
- Chronic Suppurative Otitis Media (CSOM)Document31 pagesChronic Suppurative Otitis Media (CSOM)Mimo HemadNo ratings yet
- Inflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandInflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cholesteatoma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCholesteatoma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Lec.9 Sinonasal TumorsDocument25 pagesLec.9 Sinonasal TumorsMariam QaisNo ratings yet
- Pharyngeal Tumours2Document46 pagesPharyngeal Tumours2miramirajalalNo ratings yet
- External Ear Pathology - PresentationDocument25 pagesExternal Ear Pathology - PresentationNipun MalhotraNo ratings yet
- Cholesteatoma: Clinical Features Diagnosis TreatmentDocument19 pagesCholesteatoma: Clinical Features Diagnosis TreatmentDoodNo ratings yet
- Differential Diagnosis of VertigoDocument56 pagesDifferential Diagnosis of VertigoIkhfa Yusril BahariNo ratings yet
- Otitis MediaDocument67 pagesOtitis MediaFurqan MirzaNo ratings yet
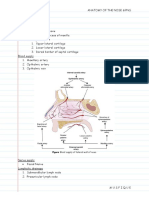
- Anatomy of The Nose & Paranasal Air SinusesDocument4 pagesAnatomy of The Nose & Paranasal Air SinusesMusfique RashidNo ratings yet
- Common Ent EmergenciesDocument65 pagesCommon Ent EmergenciesferaNo ratings yet
- DysphagiaDocument4 pagesDysphagiaMicaNo ratings yet
- ORL Interns NotesDocument15 pagesORL Interns NotesSandy Chiong MaganitoNo ratings yet
- Stridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiDocument33 pagesStridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiVishal GauravNo ratings yet
- Basic Sinus AnatomyDocument71 pagesBasic Sinus AnatomyTalal AlanzyNo ratings yet
- Diseases of External EarDocument66 pagesDiseases of External Earalmazmulu76100% (1)
- Developmental Disturbances of The TongueDocument29 pagesDevelopmental Disturbances of The TonguepriyaNo ratings yet
- External Ear DiseasesDocument6 pagesExternal Ear DiseasesJohn Christopher LucesNo ratings yet
- Laryngeal CancerDocument41 pagesLaryngeal CancerNidya PutriNo ratings yet
- Examination of ThyroidDocument4 pagesExamination of ThyroidNoor Ul AinNo ratings yet
- ENT AyaSalahEldeenDocument147 pagesENT AyaSalahEldeenFatma ShnewraNo ratings yet
- Benign Malignant LarynxDocument28 pagesBenign Malignant LarynxfaizNo ratings yet
- Juvenile Nasopharyngial AngiofibromaDocument8 pagesJuvenile Nasopharyngial AngiofibromaDr-Firas Nayf Al-ThawabiaNo ratings yet
- (Ent) 02 Endoscopy Applied Physiology EditedDocument5 pages(Ent) 02 Endoscopy Applied Physiology EditedKanako TakayaNo ratings yet
- Ent Ospe Badhahin v1 7 PDFDocument26 pagesEnt Ospe Badhahin v1 7 PDFWasi OsmanNo ratings yet
- JnaDocument34 pagesJnaDeepak KumarNo ratings yet
- ScenarioDocument23 pagesScenarioAakashNo ratings yet
- Tonsillitis & TonsillectomyDocument18 pagesTonsillitis & TonsillectomyLuqman HakimNo ratings yet
- Uk PFAPADocument5 pagesUk PFAPAPrerna SehgalNo ratings yet
- Sailedinitis PDFDocument8 pagesSailedinitis PDFNavatha MorthaNo ratings yet
- DYSPHAGIA Lecture NotesDocument84 pagesDYSPHAGIA Lecture Notesmcmak357No ratings yet
- Keratosis ObturansDocument12 pagesKeratosis ObturansRahma LuthfaNo ratings yet
- Rhino SinusitisDocument57 pagesRhino SinusitisArif MohammedNo ratings yet
- Upper Airway ObstructionDocument17 pagesUpper Airway ObstructionRai Hana100% (1)
- Cervicofacial LymphangiomasDocument11 pagesCervicofacial LymphangiomasCharmila Sari100% (1)
- ENT OSPE (Batch 2) - 1Document11 pagesENT OSPE (Batch 2) - 1Mahnoor khanNo ratings yet
- Nose and Parasinuses: I. A. B. C. D. E. F. G. II. A. B. C. D. IiiDocument3 pagesNose and Parasinuses: I. A. B. C. D. E. F. G. II. A. B. C. D. IiiKenneth TorresNo ratings yet
- Anatomy PharynxDocument15 pagesAnatomy PharynxNina ZabrinaNo ratings yet
- 20 - Common ENT Emergencies - FowlerDocument25 pages20 - Common ENT Emergencies - FowlerFrita Oktina WijayaNo ratings yet
- Tumours of Larynx: Benign MalignantDocument43 pagesTumours of Larynx: Benign MalignantVandana RaviNo ratings yet
- Oral Cavity PharynxDocument9 pagesOral Cavity PharynxKezia MondonedoNo ratings yet
- Recurrent Respiratory Papillomatosis: FaringDocument49 pagesRecurrent Respiratory Papillomatosis: FaringIchsanJuliansyahNo ratings yet
- AtelektasisDocument15 pagesAtelektasisMuhammad Ade RahmanNo ratings yet
- Ear, Nose and Throat EmergenciesDocument3 pagesEar, Nose and Throat Emergenciesfmta100% (1)
- Embryology, Anatomy and Physiology & Disease of The LarynxDocument83 pagesEmbryology, Anatomy and Physiology & Disease of The LarynxGeraldine Marie SalvoNo ratings yet
- Headache-An ENT ProblemDocument59 pagesHeadache-An ENT ProblemMrudula MukiriNo ratings yet
- Dse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesDocument5 pagesDse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesLuka Desabelle- JustoNo ratings yet
- Chronic RhinosinusitisDocument36 pagesChronic RhinosinusitisAritro BhattacharjiNo ratings yet
- Otogenic MeningitisDocument15 pagesOtogenic Meningitisadam Nohe100% (1)
- Pyogenic MeningitisDocument46 pagesPyogenic MeningitisShahnaaz ShahNo ratings yet
- Stenosis, Scleroma, TracheostomyDocument22 pagesStenosis, Scleroma, Tracheostomysimi yNo ratings yet
- Surgical Management of Thyroid NeoplasmsDocument15 pagesSurgical Management of Thyroid NeoplasmsalameluNo ratings yet
- Laryngitis: SpasmDocument13 pagesLaryngitis: Spasm44-Shruti paghdalNo ratings yet
- Middle Ear, Ossicles, Eustachian Tube (Done)Document17 pagesMiddle Ear, Ossicles, Eustachian Tube (Done)Dr-Firas Nayf Al-ThawabiaNo ratings yet
- Cme Bronchial AsthmaDocument28 pagesCme Bronchial AsthmaameerabestNo ratings yet
- @acute Nephritic SyndromeDocument3 pages@acute Nephritic Syndromeameerabest100% (1)
- Genital EmbryologyDocument6 pagesGenital EmbryologyameerabestNo ratings yet
- @tumors of The Breast 1Document2 pages@tumors of The Breast 1ameerabestNo ratings yet
- @ovary Cyst ComparisonDocument2 pages@ovary Cyst ComparisonameerabestNo ratings yet
- PleuraDocument6 pagesPleuraameerabest100% (1)
- Semen AnalysisDocument3 pagesSemen Analysisameerabest80% (5)
- #Chest TraumasDocument4 pages#Chest Traumasameerabest100% (3)
- OSCE DermaDocument8 pagesOSCE DermaameerabestNo ratings yet
- Extracorporial Circulation (Ecc) Heart Lung Machine Cardio-Pulmonary Bypass (CPB)Document2 pagesExtracorporial Circulation (Ecc) Heart Lung Machine Cardio-Pulmonary Bypass (CPB)ameerabestNo ratings yet
- #MediastinumDocument4 pages#Mediastinumameerabest100% (1)
- PharynxDocument2 pagesPharynxameerabest0% (1)
- Oesophagus & StomachDocument3 pagesOesophagus & StomachameerabestNo ratings yet
- #LungDocument1 page#LungameerabestNo ratings yet
- Parotid Gland Submandibular Gland Sublingual GlandDocument5 pagesParotid Gland Submandibular Gland Sublingual GlandameerabestNo ratings yet
- Mouth Cavity, Palate, TongueDocument8 pagesMouth Cavity, Palate, Tongueameerabest100% (1)
- Nle Nursing Practice VDocument13 pagesNle Nursing Practice Vjptorresrn09No ratings yet
- Common Ear ProblemsDocument3 pagesCommon Ear ProblemsJômêl D. GûîvêsêsNo ratings yet
- Ear, Nose and Throat emerg-ENT-cies: With Laura WilkinsDocument43 pagesEar, Nose and Throat emerg-ENT-cies: With Laura WilkinsIrina AndreeaNo ratings yet
- Daftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10Document10 pagesDaftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10kartianiNo ratings yet
- Ear ExaminationDocument3 pagesEar ExaminationmuhammadridhwanNo ratings yet
- IVRSDocument61 pagesIVRSAndrew ChinchillaNo ratings yet
- Ear InfectionDocument8 pagesEar InfectionArt Christian Ramos100% (1)
- Jurnal Adhesive Otitis MediaDocument18 pagesJurnal Adhesive Otitis MediaJimmy ChuaNo ratings yet
- ENT - UnitDocument63 pagesENT - Unitsuganthi rajesh kannaNo ratings yet
- Integrated Management of Childhood Illness (IMCI) Knowledge Post-Test With Answer KeyDocument8 pagesIntegrated Management of Childhood Illness (IMCI) Knowledge Post-Test With Answer KeyCarissa De Luzuriaga-BalariaNo ratings yet
- Kode ICD 10 THTDocument10 pagesKode ICD 10 THTAnung Setiawan0% (1)
- Pap 0106Document31 pagesPap 0106Bogdan PraščevićNo ratings yet
- Mankekar - Implantablehearing Devices Other Than Cochlear ImplantsDocument119 pagesMankekar - Implantablehearing Devices Other Than Cochlear ImplantscetristanNo ratings yet
- Chronic Otitis MediaDocument4 pagesChronic Otitis MediaOvyanda Eka MItraNo ratings yet
- Pharmacotherapy of Infectious Disease URTIDocument44 pagesPharmacotherapy of Infectious Disease URTIDigafe TolaNo ratings yet
- #Disease of External EarDocument4 pages#Disease of External EarameerabestNo ratings yet
- 10 Besar 1 TH 2017Document356 pages10 Besar 1 TH 2017dartosNo ratings yet
- Syllabus of Ent Residency ProgramJMOHDocument30 pagesSyllabus of Ent Residency ProgramJMOHadham bani younesNo ratings yet
- Candida ParapsilosisDocument20 pagesCandida ParapsilosisscribdenesimoNo ratings yet
- 18 COSM ProgramGuide Final PDFDocument76 pages18 COSM ProgramGuide Final PDFfluffy4202011No ratings yet
- Platinum Notes - ENTDocument55 pagesPlatinum Notes - ENTsk100% (1)
- Latest Research in HomeopathyDocument76 pagesLatest Research in Homeopathywww nambisons com100% (3)
- Otitis Media AkutDocument28 pagesOtitis Media AkutMuhammad IqbalNo ratings yet
- Cholesteatoma Definition and Classification: A Literature ReviewDocument6 pagesCholesteatoma Definition and Classification: A Literature ReviewRobertNo ratings yet
- Chapter 2 Board ExamDocument20 pagesChapter 2 Board ExamAljohn Galang100% (2)
- Ear Irrigation Assessment FormDocument1 pageEar Irrigation Assessment FormIosefina DudeanuNo ratings yet
- Guideline URTI in South Africa 2008Document9 pagesGuideline URTI in South Africa 2008Febbe Nadia Okky LucianaNo ratings yet
- Diseases of The EarDocument48 pagesDiseases of The Earabela_amulu100% (1)
- The Name of Your Medicine Is - : Ear DropsDocument2 pagesThe Name of Your Medicine Is - : Ear DropsKatty BrownNo ratings yet