Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Healthy Vision-Prevent and Reverse Eye Disease Through Better NutritionDocument105 pagesHealthy Vision-Prevent and Reverse Eye Disease Through Better NutritionAnh Ngô Đức100% (2)
- Lecture 7Document68 pagesLecture 7Gay TonyNo ratings yet
- 통계 숙제 9Document2 pages통계 숙제 9Khongmuon NoiNo ratings yet
- IMDC Anatomy Mock Test 1b-1-1Document4 pagesIMDC Anatomy Mock Test 1b-1-1Tofunmi AdegokeNo ratings yet
- APE QuestionsDocument6 pagesAPE QuestionsJahg WongNo ratings yet
- GMO Presentation PDFDocument20 pagesGMO Presentation PDFKen CabanligNo ratings yet
- Modified IntroductionDocument28 pagesModified IntroductionNormana ZureikatNo ratings yet
- Myelodysplasia (Definition/Incidence)Document10 pagesMyelodysplasia (Definition/Incidence)IlyasHasanNo ratings yet
- Liver: Prepared By: Marah Abo Rashed Instructor: DR - Nimer KhraimDocument13 pagesLiver: Prepared By: Marah Abo Rashed Instructor: DR - Nimer KhraimSheMoHijaziNo ratings yet
- STEP Biology (1-18) All Worksheets 2020Document294 pagesSTEP Biology (1-18) All Worksheets 2020kirki pNo ratings yet
- Developmental Disturbances in Oral CavityDocument14 pagesDevelopmental Disturbances in Oral CavityYashmeen XNo ratings yet
- PSILOCYBIN MUSHROOMS The Complete Guide To Grow Magic Mushrooms and Safe Use, Discover The Healing Power of Psychedelic Mushrooms by Frank HollandDocument62 pagesPSILOCYBIN MUSHROOMS The Complete Guide To Grow Magic Mushrooms and Safe Use, Discover The Healing Power of Psychedelic Mushrooms by Frank HollandFernanda Martínez CórdobaNo ratings yet
- Structure and Function of EyesDocument11 pagesStructure and Function of EyesSamar Ameen SialNo ratings yet
- Holistic Health EssayDocument28 pagesHolistic Health EssayDr. Luciano A. Pulido100% (1)
- Drug-Induced Taste Disorders in Clinical Practice and Preclinical Safety EvaluationDocument10 pagesDrug-Induced Taste Disorders in Clinical Practice and Preclinical Safety EvaluationBharat NarumanchiNo ratings yet
- Aspergillus SPDocument10 pagesAspergillus SPSandu PaulNo ratings yet
- Human Immunodeficiency VirusDocument87 pagesHuman Immunodeficiency Virustummalapalli venkateswara raoNo ratings yet
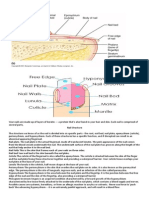
- Your Nails Are Made Up of Layers of KeratinDocument2 pagesYour Nails Are Made Up of Layers of KeratinRetchel LiwagonNo ratings yet
- Contrabending and Reverse Twist As A Basic Biomechanical Force To Correct Deformity in Scoliosis (Revision) Docx PDFDocument11 pagesContrabending and Reverse Twist As A Basic Biomechanical Force To Correct Deformity in Scoliosis (Revision) Docx PDFFahmi AnshoriNo ratings yet
- Vox Sanguin April 2022 - Opt1Document181 pagesVox Sanguin April 2022 - Opt1rsdarsono labNo ratings yet
- UG022524 International GCSE in Human Biology 4HB0 For PrintDocument60 pagesUG022524 International GCSE in Human Biology 4HB0 For Printneoiq5719No ratings yet
- Effects of Different Natural Dewormers FDocument10 pagesEffects of Different Natural Dewormers FMelvin John EnanoNo ratings yet
- Stages of Prenatal Development Causes of Development DiseasesDocument2 pagesStages of Prenatal Development Causes of Development DiseasesAnnah Caponpon GalorNo ratings yet
- Historyof Genetics QuizDocument2 pagesHistoryof Genetics QuizGelli NancaNo ratings yet
- Project in Mapeh (Health)Document8 pagesProject in Mapeh (Health)guache warrinNo ratings yet
- Chronic Leukemia HerfindalDocument40 pagesChronic Leukemia HerfindalAanshi ShahNo ratings yet
- How To Transfer A Mobilizable Plasmid From A Cell Without A Conjugative Plasmid?Document14 pagesHow To Transfer A Mobilizable Plasmid From A Cell Without A Conjugative Plasmid?m86544422No ratings yet
- Autosomal Dominant DisordersDocument11 pagesAutosomal Dominant DisordersbluesaltNo ratings yet
- Albrektsson Foreign Body ReactionDocument11 pagesAlbrektsson Foreign Body ReactionjeremyvoNo ratings yet
- (Ricardo v. Lloyd) Morphology Methods Cell and Mo (B-Ok - Xyz)Document439 pages(Ricardo v. Lloyd) Morphology Methods Cell and Mo (B-Ok - Xyz)dedi sunarto100% (1)