Download as pdf or txt
You might also like
- Lactic Acid Bacteria Fundamentals and Practice PDFDocument536 pagesLactic Acid Bacteria Fundamentals and Practice PDFIrving Mayo100% (3)
- Manual of Diagnostic Tests For Aquatic Animals 2010Document399 pagesManual of Diagnostic Tests For Aquatic Animals 2010Renato Leite LeonardoNo ratings yet
- Online High School OM013: Honors Precalculus With TrigonometryDocument2 pagesOnline High School OM013: Honors Precalculus With TrigonometryJin SiclonNo ratings yet
- WHO HSE WSH 10.04 Eng PDFDocument36 pagesWHO HSE WSH 10.04 Eng PDFDamaris AdiNo ratings yet
- Pharmaceuticals in WaterDocument49 pagesPharmaceuticals in Waterapi-256236481No ratings yet
- WHO HSE WSH 11.03 EngDocument32 pagesWHO HSE WSH 11.03 EngMaruthi KNo ratings yet
- Temephos in Drinking-Water: Use For Vector Control in Drinking-Water Sources and ContainersDocument14 pagesTemephos in Drinking-Water: Use For Vector Control in Drinking-Water Sources and ContainersMochHabibEl-HuseinyNo ratings yet
- Arsenic in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityDocument18 pagesArsenic in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityRebeca PanzlNo ratings yet
- Manual of Diagnostic Tests For Aquatic Animals: Fourth Edition, 2003Document366 pagesManual of Diagnostic Tests For Aquatic Animals: Fourth Edition, 2003nhimdoc2016No ratings yet
- Boron in Drinking WaterDocument28 pagesBoron in Drinking WatercysautsNo ratings yet
- OIE Manual Diagnostic ENGLISHDocument401 pagesOIE Manual Diagnostic ENGLISHIndah PraptiasihNo ratings yet
- Chlorine Dioxide Chlorite Chlorate Background Jan17Document24 pagesChlorine Dioxide Chlorite Chlorate Background Jan17Decky Ari IrwantoNo ratings yet
- Asbestos WHO 2003Document9 pagesAsbestos WHO 2003Ayman66No ratings yet
- Cyanobacterial Toxins - Microcystin LR in Drinking WaterDocument18 pagesCyanobacterial Toxins - Microcystin LR in Drinking WaterSusana NunesNo ratings yet
- Briefing Note: Antimicrobial Resistance: An Emerging Water, Sanitation and Hygiene IssueDocument16 pagesBriefing Note: Antimicrobial Resistance: An Emerging Water, Sanitation and Hygiene IssueBoni MagtibayNo ratings yet
- Bromide in Drinking-Water PDFDocument15 pagesBromide in Drinking-Water PDFSalem GarrabNo ratings yet
- Bartram2004 PDFDocument2 pagesBartram2004 PDF111280No ratings yet
- Molybdenum in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityDocument18 pagesMolybdenum in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityLaurențiu Mihai BălanNo ratings yet
- Dichloro Acetic Acid 0505Document29 pagesDichloro Acetic Acid 0505Neva BernadetteNo ratings yet
- Hex A Chloro But A DieneDocument15 pagesHex A Chloro But A DieneAfraNo ratings yet
- CadmiumDocument16 pagesCadmiumPopescu DragosNo ratings yet
- PH Drinking Water StandardsDocument7 pagesPH Drinking Water StandardsElisabeth BalarezoNo ratings yet
- Hardness by WHODocument19 pagesHardness by WHObtuzlaNo ratings yet
- Sodium in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityDocument11 pagesSodium in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityPopescu DragosNo ratings yet
- Guidelines For Drinking-Water QualityDocument8 pagesGuidelines For Drinking-Water QualityJin SiclonNo ratings yet
- International Standards of Drinking WaterDocument148 pagesInternational Standards of Drinking Watere_afshahNo ratings yet
- Edetic Acid (EDTA) in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityDocument15 pagesEdetic Acid (EDTA) in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityBhavikNo ratings yet
- Detection and Abundance of SARS-CoV-2 in Wastewater - jwh0200114Document12 pagesDetection and Abundance of SARS-CoV-2 in Wastewater - jwh0200114고주형No ratings yet
- WHO HSE WSH 10.01 10 Rev1 EngDocument19 pagesWHO HSE WSH 10.01 10 Rev1 EngAman YadavNo ratings yet
- Nickel2005 OmsDocument30 pagesNickel2005 OmsbuffysangoNo ratings yet
- Prevention of Legionnaires DiseaseDocument41 pagesPrevention of Legionnaires DiseasejoechengshNo ratings yet
- Petroleum Products in Drinking-Water: WHO/SDE/WSH/05.08/123 English OnlyDocument20 pagesPetroleum Products in Drinking-Water: WHO/SDE/WSH/05.08/123 English OnlyMaripaz DominguezNo ratings yet
- DH HTM 0401 Part C AccDocument20 pagesDH HTM 0401 Part C AccKarthikNo ratings yet
- Manganese WHODocument29 pagesManganese WHOFitri WulandariNo ratings yet
- 1,2 Dibromo 3 ChloropropaneDocument11 pages1,2 Dibromo 3 ChloropropaneWahyu Dwi suci putrianiNo ratings yet
- Evaluating Water TreatmentDocument68 pagesEvaluating Water TreatmentBinyam Kebede100% (1)
- Dichloromethane in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityDocument12 pagesDichloromethane in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityJudy Anne Mae Del RosarioNo ratings yet
- Chlorine in Drinking Water OMSDocument11 pagesChlorine in Drinking Water OMSAllan NavarroNo ratings yet
- Uranium in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityDocument23 pagesUranium in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityAdel SukerNo ratings yet
- Uranium290605 PDFDocument26 pagesUranium290605 PDFAnkur SoodNo ratings yet
- Water For HealthDocument6 pagesWater For HealthKeren ZelcNo ratings yet
- Food Safety Issues Associated With Products From AquacultureDocument68 pagesFood Safety Issues Associated With Products From AquaculturemdkadryNo ratings yet
- LE 01 - (1958) WHO - International Standards For Drinking-WaterDocument148 pagesLE 01 - (1958) WHO - International Standards For Drinking-WateryuliaNo ratings yet
- WHO Bromate in Drinking WaterDocument24 pagesWHO Bromate in Drinking WaterBernardo ChaconNo ratings yet
- Who CholeraDocument90 pagesWho CholeraNova ManNo ratings yet
- WHO Guidelines For WaterDocument80 pagesWHO Guidelines For WaterBilal Tahir GondalNo ratings yet
- 1 s2.0 S004313541730043X MainDocument9 pages1 s2.0 S004313541730043X MainMaría Fernanda Morales RodríguezNo ratings yet
- Aquatabs Technical Report.2012Document48 pagesAquatabs Technical Report.2012Carlos Alberto Rivera RuizNo ratings yet
- 9260 Introduction To Detecting Pathogenic BacteriaDocument3 pages9260 Introduction To Detecting Pathogenic Bacteriaandria.aquinoNo ratings yet
- Hardness in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityDocument9 pagesHardness in Drinking-Water: Background Document For Development of WHO Guidelines For Drinking-Water QualityLionel TaneoNo ratings yet
- Chloralhydrate 130605Document33 pagesChloralhydrate 130605Mohammed IbrahimNo ratings yet
- International Medical Guide For ShipsDocument364 pagesInternational Medical Guide For ShipsNaidin Iusein100% (1)
- FNE567 - 2017 Determination - of - Water - Activity - in - FoodDocument15 pagesFNE567 - 2017 Determination - of - Water - Activity - in - FoodJocilene DantasNo ratings yet
- Management of Waste From Injection Activities at District LevelDocument26 pagesManagement of Waste From Injection Activities at District LevelAyesha MunnirNo ratings yet
- 3105 PDFDocument177 pages3105 PDFsaishankarlNo ratings yet
- WHO Guidlines For Manganese 2021Document68 pagesWHO Guidlines For Manganese 2021Pike TVNo ratings yet
- EURO WSP Field Guide 2014Document100 pagesEURO WSP Field Guide 2014PoppyNo ratings yet
- Boron PDFDocument17 pagesBoron PDFAnonymous qKeDFDNo ratings yet
- Exposure due to Radionuclides in Food Other than During a Nuclear or Radiological Emergency: Part 1: Technical MaterialFrom EverandExposure due to Radionuclides in Food Other than During a Nuclear or Radiological Emergency: Part 1: Technical MaterialNo ratings yet
- Beyond One Health: From Recognition to ResultsFrom EverandBeyond One Health: From Recognition to ResultsJohn A. HerrmannNo ratings yet
- Securing Safe Water Supplies: Comparison of Applicable TechnologiesFrom EverandSecuring Safe Water Supplies: Comparison of Applicable TechnologiesNo ratings yet
- Xecutive Ummary: Work Sharing During The Great RecessionDocument4 pagesXecutive Ummary: Work Sharing During The Great RecessionJin SiclonNo ratings yet
- Essential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and NutritionDocument116 pagesEssential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and NutritionJin SiclonNo ratings yet
- Tendencias Mundiales Empleo - 2013 - OIT (Inglés)Document172 pagesTendencias Mundiales Empleo - 2013 - OIT (Inglés)David Velázquez SeiferheldNo ratings yet
- Informal Employment in Namibia 2008Document68 pagesInformal Employment in Namibia 2008Jin SiclonNo ratings yet
- Social Protection Floor For A Fair and Inclusive GlobalizationDocument150 pagesSocial Protection Floor For A Fair and Inclusive GlobalizationSalam Salam Solidarity (fauzi ibrahim)No ratings yet
- 2012 06 Statistical Update v2Document28 pages2012 06 Statistical Update v2Jin SiclonNo ratings yet
- Decent Work Indicators in Africa - A First Assessment Based On National SourcesDocument160 pagesDecent Work Indicators in Africa - A First Assessment Based On National SourcesJin SiclonNo ratings yet
- Decent Work Indicators - Concepts and DefinitionsDocument170 pagesDecent Work Indicators - Concepts and DefinitionsJin SiclonNo ratings yet
- Annex 9.: Most Malaria Prone Areas in The Menoreh Hills ( 200M) - Yogyakarta Central JavaDocument1 pageAnnex 9.: Most Malaria Prone Areas in The Menoreh Hills ( 200M) - Yogyakarta Central JavaJin SiclonNo ratings yet
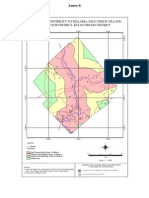
- Maps of Susceptibility To Malaria, Selo Timur Village, Kokap Sub District, Kulon Progo DistrictDocument1 pageMaps of Susceptibility To Malaria, Selo Timur Village, Kokap Sub District, Kulon Progo DistrictJin SiclonNo ratings yet
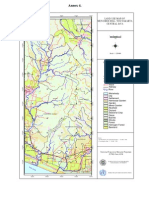
- Annex 4.: Land Use Map of Menoreh Hill-Yogyakarta Central JavaDocument1 pageAnnex 4.: Land Use Map of Menoreh Hill-Yogyakarta Central JavaJin SiclonNo ratings yet
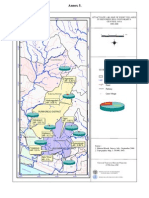
- Annex 5Document1 pageAnnex 5Jin SiclonNo ratings yet
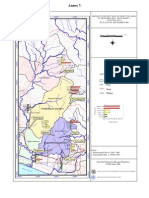
- Annex 7Document1 pageAnnex 7Jin SiclonNo ratings yet
- Annex 6.: Beyond The Study Area River Road Railway Case Village NgemplakDocument1 pageAnnex 6.: Beyond The Study Area River Road Railway Case Village NgemplakJin SiclonNo ratings yet
- 01-579 TDS enDocument2 pages01-579 TDS enGeoemilia1No ratings yet
- Guide To Infection ControlDocument9 pagesGuide To Infection ControlMita RefanitaNo ratings yet
- Bacteria and Yeast Work-Up ManualDocument19 pagesBacteria and Yeast Work-Up ManualS ONo ratings yet
- Ijmrhs Vol 2 Issue 3Document399 pagesIjmrhs Vol 2 Issue 3editorijmrhs100% (1)
- Isolation of Microbes From FruitsDocument3 pagesIsolation of Microbes From FruitsDevlina SenguptaNo ratings yet
- Antimicrobial ResistanceDocument46 pagesAntimicrobial ResistanceEmil CotenescuNo ratings yet
- Escherichia Coli, and Enteric: Enteric Indicator Organisms in FoodsDocument7 pagesEscherichia Coli, and Enteric: Enteric Indicator Organisms in Foodssiddharth2907No ratings yet
- Biochemical Test For Enterococcus SPDocument6 pagesBiochemical Test For Enterococcus SPganbio1981No ratings yet
- Azide Dextrose BrothDocument1 pageAzide Dextrose BrothJHOSELINE KHATERINE RAMIREZ BARBARANNo ratings yet
- Streptococci and Enterococci and OthersDocument11 pagesStreptococci and Enterococci and OthersthedarkwingNo ratings yet
- CAT Nº: 1031: Bile Esculin Agar Iso 10273Document2 pagesCAT Nº: 1031: Bile Esculin Agar Iso 10273KATHENo ratings yet
- Pediatric Antibiotic Dosing Card 2012Document2 pagesPediatric Antibiotic Dosing Card 2012yoshilimsiacoshigyoNo ratings yet
- BacteriaDocument3 pagesBacteriaviju josephNo ratings yet
- IDSA - Guía de Infección Asociada A Catéter VenosoDocument45 pagesIDSA - Guía de Infección Asociada A Catéter Venosoivonne micoltaNo ratings yet
- Antimicrobial Activity of Plant Extracts From Several GeneraDocument20 pagesAntimicrobial Activity of Plant Extracts From Several GeneraPrograma BRICNo ratings yet
- Food and Industrial MicrobiologyDocument196 pagesFood and Industrial Microbiologyisabeljanuario67% (3)
- Chapter 22 Streptococcus, Enterococcus and PneumococcusDocument73 pagesChapter 22 Streptococcus, Enterococcus and PneumococcusPriyanshiNo ratings yet
- Bile Aesuclin Azide Agar: ApplicationDocument3 pagesBile Aesuclin Azide Agar: ApplicationJimmy Rodríguez JuárezNo ratings yet
- Bacteria&YeastDocument13 pagesBacteria&YeastGuy SoreqNo ratings yet
- Uji Deteksi Biofilm Dari Isolat Klinik Kateter Urin Bakteri Entercoccus Dibandingkan Dengan Tube MethodDocument27 pagesUji Deteksi Biofilm Dari Isolat Klinik Kateter Urin Bakteri Entercoccus Dibandingkan Dengan Tube MethodIyannyanNo ratings yet
- Streptococcus and EnterococcusDocument91 pagesStreptococcus and EnterococcusAllyah Ross DuqueNo ratings yet
- Daptomycin 5Document2 pagesDaptomycin 5SachithNo ratings yet
- Central Line Infection PathwayDocument36 pagesCentral Line Infection PathwaycignalNo ratings yet
- 4-1 WaterDocument26 pages4-1 WatertuNo ratings yet
- Micro ChecklistDocument32 pagesMicro Checklistmasthan6yNo ratings yet
- CLSI M100 32e 2022 - Central Labs SummaryDocument9 pagesCLSI M100 32e 2022 - Central Labs Summaryshimaa khaterNo ratings yet
- 3 EnterococcusDocument15 pages3 Enterococcus01. Akhmad Gilang R - XII MIPA 4No ratings yet
- Infectious Diseases of The Female Genital TractDocument1,111 pagesInfectious Diseases of The Female Genital TractJohn Ntokos100% (2)
- Manual, Bacteria and Yeast Work UpDocument12 pagesManual, Bacteria and Yeast Work UpFilipus HendiantoNo ratings yet