
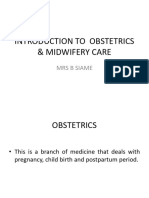
Vacuum Extraction
Vacuum Extraction
You might also like
- Placenta PreviaDocument33 pagesPlacenta PreviaKinjal VasavaNo ratings yet
- Reading Test 01 - E2Lang PDFDocument25 pagesReading Test 01 - E2Lang PDFMuhammad Haneef100% (12)
- Partograph PPT 1Document55 pagesPartograph PPT 1Maria Lejani Terencio100% (1)
- Obstetric Emergencies and Anesthetic Management: Co-Ordinator: DR - Navab Singh (M.D.) Speaker: Dr. UdayDocument35 pagesObstetric Emergencies and Anesthetic Management: Co-Ordinator: DR - Navab Singh (M.D.) Speaker: Dr. UdayKutumela MolebogengNo ratings yet
- Forceps Delivery, Vacuum Extraction & Caesarean SectionDocument83 pagesForceps Delivery, Vacuum Extraction & Caesarean SectionannazhelNo ratings yet
- Admission of A Woman in LaborDocument22 pagesAdmission of A Woman in LaborRed Williams100% (2)
- Art TherapyDocument21 pagesArt TherapyIem Evan67% (3)
- Glanders in HorseDocument43 pagesGlanders in HorseWerner AlbuquerqueNo ratings yet
- Current Trends in ObstetricsDocument6 pagesCurrent Trends in ObstetricsShyrra Edades Pinder100% (1)
- Ethics in Midwifery PowerpointDocument24 pagesEthics in Midwifery PowerpointEden NatividadNo ratings yet
- Shoulder DystociaDocument14 pagesShoulder Dystociarake sardevaNo ratings yet
- Intrauterine Fetal DemiseDocument7 pagesIntrauterine Fetal DemiseElaisa Mae Delos SantosNo ratings yet
- Antenatal CareDocument27 pagesAntenatal CareFelaih Binasoy Dela CruzNo ratings yet
- Prolonged PregnancyDocument40 pagesProlonged Pregnancyjan caraNo ratings yet
- Bleeding During PregnancyDocument5 pagesBleeding During PregnancyMaryela Maceda GalozoNo ratings yet
- Introduction To Obstetrics & Midwifery CareDocument18 pagesIntroduction To Obstetrics & Midwifery CareWhirmey ChinyamaNo ratings yet
- Factors Influencing Umbilical Cord Care Practices Among Mothers Attending Infant Welfare Clinic in Selected PrimarDocument58 pagesFactors Influencing Umbilical Cord Care Practices Among Mothers Attending Infant Welfare Clinic in Selected PrimarChukwu SolomonNo ratings yet
- Mechanisms of LaborDocument16 pagesMechanisms of LaborRyan Robert V. Ventolero100% (1)
- 3rd and 4th Stage of LaborDocument8 pages3rd and 4th Stage of LaborMarco Paulo Reyes NaoeNo ratings yet
- Unang YakapDocument45 pagesUnang YakapMarie JhoanaNo ratings yet
- Abnormalities of PuerperiumDocument70 pagesAbnormalities of PuerperiumYasmin SharmaNo ratings yet
- Antepartum Haemorrage (APH) : Dr. Mtumweni, MDDocument42 pagesAntepartum Haemorrage (APH) : Dr. Mtumweni, MDmarco luenaNo ratings yet
- Antenatal CareDocument82 pagesAntenatal Caremdasad18No ratings yet
- EpisiotomyDocument18 pagesEpisiotomyHamss AhmedNo ratings yet
- Vaginal Examination ChecklistDocument2 pagesVaginal Examination ChecklistANNENo ratings yet
- Maternity Nursing Part 1Document12 pagesMaternity Nursing Part 1danica_2956No ratings yet
- Obsteric EmergenciesDocument48 pagesObsteric EmergenciesNurul AshikinNo ratings yet
- Fetal MalpresentationDocument28 pagesFetal MalpresentationAhmed Gh Al-zechrawiNo ratings yet
- Complications in PregnancyDocument81 pagesComplications in PregnancyTia TahniaNo ratings yet
- Roth 10e Nclex Chapter 12Document3 pagesRoth 10e Nclex Chapter 12jennaaahhhNo ratings yet
- Obstetrical Emergency & ManagementDocument38 pagesObstetrical Emergency & ManagementDrPreeti Thakur ChouhanNo ratings yet
- Ceasarian SectionDocument4 pagesCeasarian SectionKeanu ArcillaNo ratings yet
- Multiple PregnancyDocument20 pagesMultiple PregnancySelma FraNo ratings yet
- Breech PresentationDocument35 pagesBreech PresentationPrince Jhessie L. AbellaNo ratings yet
- Management of Breech PresentationDocument13 pagesManagement of Breech Presentationdr.Hansen.SH100% (1)
- Ob 3Document14 pagesOb 3Princess LotusNo ratings yet
- What Is Dilation and Curettage (D&C) ?Document3 pagesWhat Is Dilation and Curettage (D&C) ?jaroh_20No ratings yet
- Abnormal Uterine ActionDocument37 pagesAbnormal Uterine Actionshivangi agarwalNo ratings yet
- Developed by D. Ann Currie, RN, MSNDocument40 pagesDeveloped by D. Ann Currie, RN, MSNtri utamiNo ratings yet
- High Risk PregnancyDocument14 pagesHigh Risk PregnancyJezrael PueblosNo ratings yet
- Active Management of LabourDocument4 pagesActive Management of LabourHytham AtiaNo ratings yet
- Abnormalities of Labour and Delivery and Their Management: Joó József GáborDocument44 pagesAbnormalities of Labour and Delivery and Their Management: Joó József GáborAnnisa Mutiara InsaniNo ratings yet
- Inversion of Uterus 170225210149Document54 pagesInversion of Uterus 170225210149anju kumawatNo ratings yet
- Intrapartal ComplicationsDocument70 pagesIntrapartal ComplicationsRose AnnNo ratings yet
- Ob RN 1Document47 pagesOb RN 1zenaNo ratings yet
- Postpartum Assessment and CareDocument14 pagesPostpartum Assessment and CareGail Chantel Spring PerlasNo ratings yet
- Abnormal LabourDocument21 pagesAbnormal LabourbetablockersNo ratings yet
- Obg Objective QuestionDocument1 pageObg Objective QuestionDESUN Nursing School100% (1)
- Pregnancy Induced Hypertension Case StudyDocument77 pagesPregnancy Induced Hypertension Case StudyATEHAN BORDS100% (1)
- NCM 109 Rle ClinicalDocument20 pagesNCM 109 Rle ClinicalBiway RegalaNo ratings yet
- Newborn CareDocument120 pagesNewborn Carejuly3ciaNo ratings yet
- Presentation 1Document36 pagesPresentation 1madhurima kunduNo ratings yet
- Identifying Clients at RiskDocument57 pagesIdentifying Clients at Riskcoosa liquors100% (1)
- Bleeding During PregnancyDocument4 pagesBleeding During PregnancyCarl Andre ReyesNo ratings yet
- High Risk Prenatal CareDocument4 pagesHigh Risk Prenatal CareKatherine Gayle GuiaNo ratings yet
- Obstetric Nursing Practice Test Part 1Document10 pagesObstetric Nursing Practice Test Part 1yanee06No ratings yet
- Before Starting The Presentation, I Am Requesting You All To Get A HandkerchiefDocument35 pagesBefore Starting The Presentation, I Am Requesting You All To Get A HandkerchiefOng KarlNo ratings yet
- Normal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, VapiDocument48 pagesNormal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, Vapivimmy47100% (1)
- Assessment of The Fetal Well-BeingDocument85 pagesAssessment of The Fetal Well-BeingAlphine DalgoNo ratings yet
- Ectopic PregnancyDocument3 pagesEctopic PregnancyforbiddenleiNo ratings yet
- Nle - High-Risk PregnancyDocument113 pagesNle - High-Risk Pregnancytachycardia01No ratings yet
- Role of Dietary Fibers and Nutraceuticals in Preventing DiseasesFrom EverandRole of Dietary Fibers and Nutraceuticals in Preventing DiseasesRating: 5 out of 5 stars5/5 (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Causes of Spontaneous Abortion 2Document23 pagesCauses of Spontaneous Abortion 2kenNo ratings yet
- Exam For NursesDocument15 pagesExam For Nursesaringkinking100% (2)
- Thailand Southeast AsiaDocument2 pagesThailand Southeast Asiaanne marieNo ratings yet
- Sirosis Hepatis Dan KomplikasiDocument36 pagesSirosis Hepatis Dan KomplikasiMuhammad HafizdNo ratings yet
- Linking Dental With Medical Presentation by Dr. Carl Stoel DDSDocument44 pagesLinking Dental With Medical Presentation by Dr. Carl Stoel DDSShivendra Nath TripathiNo ratings yet
- HQCC Complaint About Brian Senewiratne and Princess Alexandra HospitalDocument4 pagesHQCC Complaint About Brian Senewiratne and Princess Alexandra HospitalDr Romesh Arya Chakravarti0% (1)
- The Body ElectricDocument335 pagesThe Body Electricsuper0sonicNo ratings yet
- KingDocument14 pagesKingNaida DizonNo ratings yet
- Conduction System of Heart and Temporary PacemakerDocument23 pagesConduction System of Heart and Temporary Pacemakersmruti prakash SahuNo ratings yet
- Adhesive Capsulitis: A Sticky IssueDocument9 pagesAdhesive Capsulitis: A Sticky Issuerudhras22No ratings yet
- Acid Base BalanceDocument59 pagesAcid Base BalanceFratila IuliaNo ratings yet
- Flap Basics I Rotation and Transposition FlapsDocument9 pagesFlap Basics I Rotation and Transposition FlapsariskaNo ratings yet
- Unit 8Document34 pagesUnit 8Deta Meila PutriNo ratings yet
- 2012-0020 EMT Practical Exam HandbookDocument122 pages2012-0020 EMT Practical Exam HandbookLuckybryan Abala100% (1)
- Decaf Coffee - Good or BadDocument5 pagesDecaf Coffee - Good or BadAdam70sdNo ratings yet
- 7 3 MR 950 Quick Guide and TroubleshootingDocument7 pages7 3 MR 950 Quick Guide and TroubleshootingsedNo ratings yet
- Electro Cardiograph yDocument215 pagesElectro Cardiograph yToufique KaziNo ratings yet
- PHICS 29th Annual Convention InvitationDocument7 pagesPHICS 29th Annual Convention InvitationsomarjnovagenNo ratings yet
- Prelim Lab With KeyDocument9 pagesPrelim Lab With KeyTuTitNo ratings yet
- Community DentistryDocument11 pagesCommunity DentistryMunir AkhtarNo ratings yet
- DoctorsDocument7 pagesDoctorsbey luNo ratings yet
- Sandeep Patterns of NursingDocument12 pagesSandeep Patterns of NursingKamlesh Kalal100% (1)
- Rsudza: Dr. Bobby H.E Fermi SDocument3 pagesRsudza: Dr. Bobby H.E Fermi Sdarr artNo ratings yet
- Lorne Basskin - Practical PE ArticleDocument5 pagesLorne Basskin - Practical PE ArticleCatalina Dumitru0% (1)
- Lock - Inventing A New DeathDocument20 pagesLock - Inventing A New Deathmaru1981No ratings yet
- Educ763 Chart AlignmentDocument6 pagesEduc763 Chart Alignmentapi-297105278No ratings yet
- ReferencesDocument6 pagesReferencesAndrew MakariosNo ratings yet
























































































Download as doc, pdf, or txt
You might also like
- Placenta PreviaDocument33 pagesPlacenta PreviaKinjal VasavaNo ratings yet
- Reading Test 01 - E2Lang PDFDocument25 pagesReading Test 01 - E2Lang PDFMuhammad Haneef100% (12)
- Partograph PPT 1Document55 pagesPartograph PPT 1Maria Lejani Terencio100% (1)
- Obstetric Emergencies and Anesthetic Management: Co-Ordinator: DR - Navab Singh (M.D.) Speaker: Dr. UdayDocument35 pagesObstetric Emergencies and Anesthetic Management: Co-Ordinator: DR - Navab Singh (M.D.) Speaker: Dr. UdayKutumela MolebogengNo ratings yet
- Forceps Delivery, Vacuum Extraction & Caesarean SectionDocument83 pagesForceps Delivery, Vacuum Extraction & Caesarean SectionannazhelNo ratings yet
- Admission of A Woman in LaborDocument22 pagesAdmission of A Woman in LaborRed Williams100% (2)
- Art TherapyDocument21 pagesArt TherapyIem Evan67% (3)
- Glanders in HorseDocument43 pagesGlanders in HorseWerner AlbuquerqueNo ratings yet
- Current Trends in ObstetricsDocument6 pagesCurrent Trends in ObstetricsShyrra Edades Pinder100% (1)
- Ethics in Midwifery PowerpointDocument24 pagesEthics in Midwifery PowerpointEden NatividadNo ratings yet
- Shoulder DystociaDocument14 pagesShoulder Dystociarake sardevaNo ratings yet
- Intrauterine Fetal DemiseDocument7 pagesIntrauterine Fetal DemiseElaisa Mae Delos SantosNo ratings yet
- Antenatal CareDocument27 pagesAntenatal CareFelaih Binasoy Dela CruzNo ratings yet
- Prolonged PregnancyDocument40 pagesProlonged Pregnancyjan caraNo ratings yet
- Bleeding During PregnancyDocument5 pagesBleeding During PregnancyMaryela Maceda GalozoNo ratings yet
- Introduction To Obstetrics & Midwifery CareDocument18 pagesIntroduction To Obstetrics & Midwifery CareWhirmey ChinyamaNo ratings yet
- Factors Influencing Umbilical Cord Care Practices Among Mothers Attending Infant Welfare Clinic in Selected PrimarDocument58 pagesFactors Influencing Umbilical Cord Care Practices Among Mothers Attending Infant Welfare Clinic in Selected PrimarChukwu SolomonNo ratings yet
- Mechanisms of LaborDocument16 pagesMechanisms of LaborRyan Robert V. Ventolero100% (1)
- 3rd and 4th Stage of LaborDocument8 pages3rd and 4th Stage of LaborMarco Paulo Reyes NaoeNo ratings yet
- Unang YakapDocument45 pagesUnang YakapMarie JhoanaNo ratings yet
- Abnormalities of PuerperiumDocument70 pagesAbnormalities of PuerperiumYasmin SharmaNo ratings yet
- Antepartum Haemorrage (APH) : Dr. Mtumweni, MDDocument42 pagesAntepartum Haemorrage (APH) : Dr. Mtumweni, MDmarco luenaNo ratings yet
- Antenatal CareDocument82 pagesAntenatal Caremdasad18No ratings yet
- EpisiotomyDocument18 pagesEpisiotomyHamss AhmedNo ratings yet
- Vaginal Examination ChecklistDocument2 pagesVaginal Examination ChecklistANNENo ratings yet
- Maternity Nursing Part 1Document12 pagesMaternity Nursing Part 1danica_2956No ratings yet
- Obsteric EmergenciesDocument48 pagesObsteric EmergenciesNurul AshikinNo ratings yet
- Fetal MalpresentationDocument28 pagesFetal MalpresentationAhmed Gh Al-zechrawiNo ratings yet
- Complications in PregnancyDocument81 pagesComplications in PregnancyTia TahniaNo ratings yet
- Roth 10e Nclex Chapter 12Document3 pagesRoth 10e Nclex Chapter 12jennaaahhhNo ratings yet
- Obstetrical Emergency & ManagementDocument38 pagesObstetrical Emergency & ManagementDrPreeti Thakur ChouhanNo ratings yet
- Ceasarian SectionDocument4 pagesCeasarian SectionKeanu ArcillaNo ratings yet
- Multiple PregnancyDocument20 pagesMultiple PregnancySelma FraNo ratings yet
- Breech PresentationDocument35 pagesBreech PresentationPrince Jhessie L. AbellaNo ratings yet
- Management of Breech PresentationDocument13 pagesManagement of Breech Presentationdr.Hansen.SH100% (1)
- Ob 3Document14 pagesOb 3Princess LotusNo ratings yet
- What Is Dilation and Curettage (D&C) ?Document3 pagesWhat Is Dilation and Curettage (D&C) ?jaroh_20No ratings yet
- Abnormal Uterine ActionDocument37 pagesAbnormal Uterine Actionshivangi agarwalNo ratings yet
- Developed by D. Ann Currie, RN, MSNDocument40 pagesDeveloped by D. Ann Currie, RN, MSNtri utamiNo ratings yet
- High Risk PregnancyDocument14 pagesHigh Risk PregnancyJezrael PueblosNo ratings yet
- Active Management of LabourDocument4 pagesActive Management of LabourHytham AtiaNo ratings yet
- Abnormalities of Labour and Delivery and Their Management: Joó József GáborDocument44 pagesAbnormalities of Labour and Delivery and Their Management: Joó József GáborAnnisa Mutiara InsaniNo ratings yet
- Inversion of Uterus 170225210149Document54 pagesInversion of Uterus 170225210149anju kumawatNo ratings yet
- Intrapartal ComplicationsDocument70 pagesIntrapartal ComplicationsRose AnnNo ratings yet
- Ob RN 1Document47 pagesOb RN 1zenaNo ratings yet
- Postpartum Assessment and CareDocument14 pagesPostpartum Assessment and CareGail Chantel Spring PerlasNo ratings yet
- Abnormal LabourDocument21 pagesAbnormal LabourbetablockersNo ratings yet
- Obg Objective QuestionDocument1 pageObg Objective QuestionDESUN Nursing School100% (1)
- Pregnancy Induced Hypertension Case StudyDocument77 pagesPregnancy Induced Hypertension Case StudyATEHAN BORDS100% (1)
- NCM 109 Rle ClinicalDocument20 pagesNCM 109 Rle ClinicalBiway RegalaNo ratings yet
- Newborn CareDocument120 pagesNewborn Carejuly3ciaNo ratings yet
- Presentation 1Document36 pagesPresentation 1madhurima kunduNo ratings yet
- Identifying Clients at RiskDocument57 pagesIdentifying Clients at Riskcoosa liquors100% (1)
- Bleeding During PregnancyDocument4 pagesBleeding During PregnancyCarl Andre ReyesNo ratings yet
- High Risk Prenatal CareDocument4 pagesHigh Risk Prenatal CareKatherine Gayle GuiaNo ratings yet
- Obstetric Nursing Practice Test Part 1Document10 pagesObstetric Nursing Practice Test Part 1yanee06No ratings yet
- Before Starting The Presentation, I Am Requesting You All To Get A HandkerchiefDocument35 pagesBefore Starting The Presentation, I Am Requesting You All To Get A HandkerchiefOng KarlNo ratings yet
- Normal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, VapiDocument48 pagesNormal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, Vapivimmy47100% (1)
- Assessment of The Fetal Well-BeingDocument85 pagesAssessment of The Fetal Well-BeingAlphine DalgoNo ratings yet
- Ectopic PregnancyDocument3 pagesEctopic PregnancyforbiddenleiNo ratings yet
- Nle - High-Risk PregnancyDocument113 pagesNle - High-Risk Pregnancytachycardia01No ratings yet
- Role of Dietary Fibers and Nutraceuticals in Preventing DiseasesFrom EverandRole of Dietary Fibers and Nutraceuticals in Preventing DiseasesRating: 5 out of 5 stars5/5 (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Causes of Spontaneous Abortion 2Document23 pagesCauses of Spontaneous Abortion 2kenNo ratings yet
- Exam For NursesDocument15 pagesExam For Nursesaringkinking100% (2)
- Thailand Southeast AsiaDocument2 pagesThailand Southeast Asiaanne marieNo ratings yet
- Sirosis Hepatis Dan KomplikasiDocument36 pagesSirosis Hepatis Dan KomplikasiMuhammad HafizdNo ratings yet
- Linking Dental With Medical Presentation by Dr. Carl Stoel DDSDocument44 pagesLinking Dental With Medical Presentation by Dr. Carl Stoel DDSShivendra Nath TripathiNo ratings yet
- HQCC Complaint About Brian Senewiratne and Princess Alexandra HospitalDocument4 pagesHQCC Complaint About Brian Senewiratne and Princess Alexandra HospitalDr Romesh Arya Chakravarti0% (1)
- The Body ElectricDocument335 pagesThe Body Electricsuper0sonicNo ratings yet
- KingDocument14 pagesKingNaida DizonNo ratings yet
- Conduction System of Heart and Temporary PacemakerDocument23 pagesConduction System of Heart and Temporary Pacemakersmruti prakash SahuNo ratings yet
- Adhesive Capsulitis: A Sticky IssueDocument9 pagesAdhesive Capsulitis: A Sticky Issuerudhras22No ratings yet
- Acid Base BalanceDocument59 pagesAcid Base BalanceFratila IuliaNo ratings yet
- Flap Basics I Rotation and Transposition FlapsDocument9 pagesFlap Basics I Rotation and Transposition FlapsariskaNo ratings yet
- Unit 8Document34 pagesUnit 8Deta Meila PutriNo ratings yet
- 2012-0020 EMT Practical Exam HandbookDocument122 pages2012-0020 EMT Practical Exam HandbookLuckybryan Abala100% (1)
- Decaf Coffee - Good or BadDocument5 pagesDecaf Coffee - Good or BadAdam70sdNo ratings yet
- 7 3 MR 950 Quick Guide and TroubleshootingDocument7 pages7 3 MR 950 Quick Guide and TroubleshootingsedNo ratings yet
- Electro Cardiograph yDocument215 pagesElectro Cardiograph yToufique KaziNo ratings yet
- PHICS 29th Annual Convention InvitationDocument7 pagesPHICS 29th Annual Convention InvitationsomarjnovagenNo ratings yet
- Prelim Lab With KeyDocument9 pagesPrelim Lab With KeyTuTitNo ratings yet
- Community DentistryDocument11 pagesCommunity DentistryMunir AkhtarNo ratings yet
- DoctorsDocument7 pagesDoctorsbey luNo ratings yet
- Sandeep Patterns of NursingDocument12 pagesSandeep Patterns of NursingKamlesh Kalal100% (1)
- Rsudza: Dr. Bobby H.E Fermi SDocument3 pagesRsudza: Dr. Bobby H.E Fermi Sdarr artNo ratings yet
- Lorne Basskin - Practical PE ArticleDocument5 pagesLorne Basskin - Practical PE ArticleCatalina Dumitru0% (1)
- Lock - Inventing A New DeathDocument20 pagesLock - Inventing A New Deathmaru1981No ratings yet
- Educ763 Chart AlignmentDocument6 pagesEduc763 Chart Alignmentapi-297105278No ratings yet
- ReferencesDocument6 pagesReferencesAndrew MakariosNo ratings yet