Download as pdf or txt
You might also like
- Essential Examination, third edition: Step-by-step guides to clinical examination scenarios with practical tips and key facts for OSCEsFrom EverandEssential Examination, third edition: Step-by-step guides to clinical examination scenarios with practical tips and key facts for OSCEsRating: 3 out of 5 stars3/5 (5)
- HyperparathyroidismDocument5 pagesHyperparathyroidismLyra Lorca75% (12)
- Handout1 - Normal Changes of AgingDocument3 pagesHandout1 - Normal Changes of Agingpissednachos0123No ratings yet
- Penilaian Status Gizi Secara Fisik-Klinis: Erni Rukmana, S.GZG., M.SiDocument62 pagesPenilaian Status Gizi Secara Fisik-Klinis: Erni Rukmana, S.GZG., M.SiSyafri UlilNo ratings yet
- CDC - An. Aisah - TB Paru & EmpiemaDocument38 pagesCDC - An. Aisah - TB Paru & Empiemaari yunantoNo ratings yet
- Neli Pastinar, Penkes UE, RPGN, SLE, Duty HannaDocument19 pagesNeli Pastinar, Penkes UE, RPGN, SLE, Duty HannaHanna GustinNo ratings yet
- Cleft Lip PDFDocument47 pagesCleft Lip PDFFaisal BalochNo ratings yet
- NCM101 Lesson Guide 7Document28 pagesNCM101 Lesson Guide 7Yahra DatangNo ratings yet
- Laporan Kasus: Gout ArthritisDocument55 pagesLaporan Kasus: Gout ArthritisikaNo ratings yet
- Geria LecturetteDocument64 pagesGeria LecturetteSVPSNo ratings yet
- Format Lapsus OA RHEUMADocument21 pagesFormat Lapsus OA RHEUMAOcan NizwarNo ratings yet
- Diabetic Ulcus Pedis Sinistra: Maulina Analita, S.KedDocument34 pagesDiabetic Ulcus Pedis Sinistra: Maulina Analita, S.KedSafira Amilia RamadaniNo ratings yet
- A Woman 55 Years Old With: Grade Ii Decubitus Ulcer Glutea Dextra RegionDocument41 pagesA Woman 55 Years Old With: Grade Ii Decubitus Ulcer Glutea Dextra RegionHananiKusumasariNo ratings yet
- "Listen To Your: Bimbao, Elijah Blaise Figueroa, Louie Donnard Villanueva, JustineDocument60 pages"Listen To Your: Bimbao, Elijah Blaise Figueroa, Louie Donnard Villanueva, JustineTee VillanuevaNo ratings yet
- PBL 7 MedDocument79 pagesPBL 7 MedSofea IzyanNo ratings yet
- Neurology Case Report Ptosis Dextra Ec Causa Meningitis TBDocument20 pagesNeurology Case Report Ptosis Dextra Ec Causa Meningitis TBastridya nabilahNo ratings yet
- RICKETS SizovaDocument35 pagesRICKETS SizovaAyeshaNo ratings yet
- Autoimmune Polyglandular SyndromesDocument76 pagesAutoimmune Polyglandular SyndromesSenoAriNo ratings yet
- Cretenism Case StudyDocument8 pagesCretenism Case StudyMonica Marie MoralesNo ratings yet
- Case 1: Dr. E. LimDocument43 pagesCase 1: Dr. E. LimJohn Joshua Lacson MedicineNo ratings yet
- A Case of HypercalcemiaDocument84 pagesA Case of HypercalcemiaJohn Louie EscardaNo ratings yet
- A Case of Ina Young Girl: SeizureDocument55 pagesA Case of Ina Young Girl: Seizuretheresa amarNo ratings yet
- Pemeriksaan Fisik EndokrinDocument47 pagesPemeriksaan Fisik EndokrinMuhamad MaxumNo ratings yet
- Clinical ExDocument123 pagesClinical ExDeepti ChaharNo ratings yet
- Snake BiteDocument66 pagesSnake BiteedfZSEADFsfsafafNo ratings yet
- CASE PRESENTATION On PachydermoperiostosisDocument14 pagesCASE PRESENTATION On PachydermoperiostosispawanNo ratings yet
- End of 4 Year OSCE - SurgeryDocument53 pagesEnd of 4 Year OSCE - SurgerySyed Irfan ArifNo ratings yet
- HIpotiroid MWDocument50 pagesHIpotiroid MWDon SarNo ratings yet
- Case Based Discussion: Cintya Dunihapsari 012116354 Coass Interna - Rsi Sultan Agung SemarangDocument25 pagesCase Based Discussion: Cintya Dunihapsari 012116354 Coass Interna - Rsi Sultan Agung SemarangCintyaNo ratings yet
- One Year Old Boy With Palatal Fistule Post Laibopalatoplasty Et Causa LabiognatopalatoschizisDocument29 pagesOne Year Old Boy With Palatal Fistule Post Laibopalatoplasty Et Causa LabiognatopalatoschizisAqiillah HepyantiNo ratings yet
- CC 22 Januari Gea AllDocument52 pagesCC 22 Januari Gea AlllatifahNo ratings yet
- Laboratory Diagnosis / Detection Techniques: Nurin Syasya Binti Mohamad ZukhiDocument9 pagesLaboratory Diagnosis / Detection Techniques: Nurin Syasya Binti Mohamad ZukhiViknish ArumugamNo ratings yet
- Medicine OSPE Pre AnnualDocument17 pagesMedicine OSPE Pre AnnualMunawarNo ratings yet
- Newborn ScreeningDocument23 pagesNewborn Screeningloglesb1No ratings yet
- Lapsus DHF InternaDocument27 pagesLapsus DHF Internakrismaputri100% (4)
- Morning Report Sunday, July 22 2018 Night ShiftDocument51 pagesMorning Report Sunday, July 22 2018 Night ShiftantogantengbangetzNo ratings yet
- Session 1Document43 pagesSession 1Mntdher EadanNo ratings yet
- Case Report Gout ArthritisDocument31 pagesCase Report Gout ArthritisNurhidayah hasanNo ratings yet
- Vih ReviewerDocument6 pagesVih ReviewerJessica Acierto FabrosNo ratings yet
- Sri Pertiwi, Syok Sepsis CAPDocument14 pagesSri Pertiwi, Syok Sepsis CAPLukman NurhakimNo ratings yet
- Etiology, Pathogenesis, Clinical Features, Diagnostics, Treatment and ProphilaxisDocument35 pagesEtiology, Pathogenesis, Clinical Features, Diagnostics, Treatment and ProphilaxisDr Uvarani Sp Care Rawang TinNo ratings yet
- Case Conference July 25 2017Document41 pagesCase Conference July 25 2017dhania patraNo ratings yet
- Parathyrooid AnsamDocument65 pagesParathyrooid Ansamansam hirbaweNo ratings yet
- CC 2 Okt Hcu NeoDocument26 pagesCC 2 Okt Hcu NeolatifahNo ratings yet
- Future Doctors Presentation Physical Examination SeminarDocument34 pagesFuture Doctors Presentation Physical Examination SeminarsuthansharmNo ratings yet
- History Pe EntDocument44 pagesHistory Pe EntFalling HateNo ratings yet
- Oral Medicine and Radiology Long Case-1Document13 pagesOral Medicine and Radiology Long Case-1NIVEDHA VAITHYANATHAN vNo ratings yet
- Individual Health Care AssessmentDocument7 pagesIndividual Health Care AssessmentDeona Perl LapazNo ratings yet
- Case Presentation SleDocument33 pagesCase Presentation SleJxyp MundoNo ratings yet
- Eci Romalia DR FirmanDocument19 pagesEci Romalia DR FirmanLukman NurhakimNo ratings yet
- DR. Onang Saraf TepiDocument65 pagesDR. Onang Saraf TepiFini AndrianiNo ratings yet
- PetNurse Info ManualDocument4 pagesPetNurse Info ManualChris BernNo ratings yet
- Synapse in My Pocket Neuro Exam & Localization - 1st Ed 2020Document63 pagesSynapse in My Pocket Neuro Exam & Localization - 1st Ed 2020SnowyNo ratings yet
- SclerodermaDocument64 pagesSclerodermaDhito Rodriguez100% (3)
- Lapjag 7 Juli 2019 DrowningDocument25 pagesLapjag 7 Juli 2019 DrowningRahmawan MapiantoNo ratings yet
- Case Review GoutDocument21 pagesCase Review GoutLaras Bani WasesoNo ratings yet
- Case StudyDocument63 pagesCase StudyRita PokharelNo ratings yet
- Toxoplasmosis CaseDocument45 pagesToxoplasmosis CaseWen wenNo ratings yet
- MORENO - Assessing Skin, Hair, Nails, Skull and Face, Eyes, Ears and Hearing, Nose and Sinuses, Mouth and OropharynxDocument11 pagesMORENO - Assessing Skin, Hair, Nails, Skull and Face, Eyes, Ears and Hearing, Nose and Sinuses, Mouth and OropharynxQueen Aiel MorenoNo ratings yet
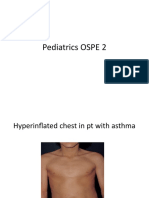
- Pediatrics OSPE 2Document40 pagesPediatrics OSPE 2malaz adilNo ratings yet
- General Approach To Lytic Bone Lesions - University of Iowa Roy J. and Lucille A. Carver College of Medicine, Iowa City, IADocument1 pageGeneral Approach To Lytic Bone Lesions - University of Iowa Roy J. and Lucille A. Carver College of Medicine, Iowa City, IAChoirul WizaNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaChoirul WizaNo ratings yet
- Treatment of Older Patients With Mantle-Cell Lymphoma: Original ArticleDocument12 pagesTreatment of Older Patients With Mantle-Cell Lymphoma: Original ArticleChoirul WizaNo ratings yet
- Asma KabulllllDocument30 pagesAsma KabulllllChoirul WizaNo ratings yet
- Therapy of Thyroid Disease With Iodine-131 v2.0Document8 pagesTherapy of Thyroid Disease With Iodine-131 v2.0Choirul WizaNo ratings yet
- Psychoanalytic CriticismDocument17 pagesPsychoanalytic CriticismChoirul WizaNo ratings yet