Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- PubMed Links 20171119Document2 pagesPubMed Links 20171119Scott BermanNo ratings yet
- Shock - Critical Care Medicine - MSD Manual Professional EditionDocument8 pagesShock - Critical Care Medicine - MSD Manual Professional EditionSughosh MitraNo ratings yet
- ccpc15 Shock Syndromes WorkbookDocument40 pagesccpc15 Shock Syndromes WorkbookJeremy HamptonNo ratings yet
- Fishman's Pulmonary Diseases and Disorders, 2008 (Dragged)Document11 pagesFishman's Pulmonary Diseases and Disorders, 2008 (Dragged)nh2411No ratings yet
- Lec 5 Functions of Circulatory SystemDocument8 pagesLec 5 Functions of Circulatory Systemmhma44490No ratings yet
- Division 3: Trauma EmergenciesDocument125 pagesDivision 3: Trauma EmergenciesGaoudam NatarajanNo ratings yet
- User Manual MS-76D1MAXSBDocument81 pagesUser Manual MS-76D1MAXSBMoises Reznik0% (1)
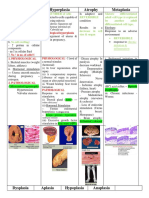
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument20 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- Pathology, Lecture 7 (Lecture Notes)Document15 pagesPathology, Lecture 7 (Lecture Notes)Ali Al-Qudsi100% (3)
- ACUTE INFLAMMATION (Vascular Changes)Document22 pagesACUTE INFLAMMATION (Vascular Changes)Ramesh KumarNo ratings yet
- Boron - Medical PhysiologyDocument13 pagesBoron - Medical PhysiologyOlgaBulat0% (6)
- Kuliah Pakar Modul 3.1Document68 pagesKuliah Pakar Modul 3.1Pramesti DarojahNo ratings yet
- Human Tecar HCR1002Document16 pagesHuman Tecar HCR1002GoranMarkovicNo ratings yet
- Inflammation and RepairDocument70 pagesInflammation and RepairmikeNo ratings yet
- Cosmetice Celulita PDFDocument4 pagesCosmetice Celulita PDFCarmen Amarandei0% (1)
- Medical Physiology Learning Objectives: Robert G. Carroll L. Gabriel Navar Mordecai P. BlausteinDocument75 pagesMedical Physiology Learning Objectives: Robert G. Carroll L. Gabriel Navar Mordecai P. BlausteinirajosephsonNo ratings yet
- Harsh Mohan Quick Review InflammationDocument23 pagesHarsh Mohan Quick Review InflammationTanaya PujareNo ratings yet
- Vasoconstriction in Septic Shock: What'S New in Intensive CareDocument4 pagesVasoconstriction in Septic Shock: What'S New in Intensive CareGabriela PachecoNo ratings yet
- Pathophysiology of Cardiogenic Pulmonary EdemaDocument13 pagesPathophysiology of Cardiogenic Pulmonary EdemaIrina DuceacNo ratings yet
- Macroscopic and Microscopic Analysis of The Cardiovascular SystemDocument117 pagesMacroscopic and Microscopic Analysis of The Cardiovascular SystemJustine Mae OyongNo ratings yet
- Shock Pathophysiology: AbstractDocument9 pagesShock Pathophysiology: AbstractHernan GonzalezNo ratings yet
- Sindrom Multiple Disfungsi OrganDocument8 pagesSindrom Multiple Disfungsi OrganAdi Nugroho MelyanaNo ratings yet
- Modelling The Cardiovascular System - MathematicsDocument226 pagesModelling The Cardiovascular System - MathematicsJosé Roberto LessaNo ratings yet
- Coronary Microvascular Disease Pathogenic Mechanisms and Therapeutic OptionsDocument17 pagesCoronary Microvascular Disease Pathogenic Mechanisms and Therapeutic OptionsZuleynny TellesNo ratings yet
- Resuscitating The Macro-Vs. Microcirculation in Septic ShockDocument8 pagesResuscitating The Macro-Vs. Microcirculation in Septic ShockjohnNo ratings yet
- The circulatory system - Зүрх судасны тогтолцооDocument2 pagesThe circulatory system - Зүрх судасны тогтолцооKhaliun MyagmarNo ratings yet
- Cardiovascular Physiology NodrmDocument528 pagesCardiovascular Physiology NodrmEmmanuel PrahNo ratings yet
- Micros Can 2Document4 pagesMicros Can 2채충일No ratings yet
- Pathogenesis of Periodontal Disease د.فراسDocument11 pagesPathogenesis of Periodontal Disease د.فراسmayssam adnanNo ratings yet
- Andrómeda Shock 2Document13 pagesAndrómeda Shock 2Cristian Daniel Espinoza ValdezNo ratings yet