Download as doc, pdf, or txt
You might also like
- Philippine Hospital Development Plan 2017-2022Document72 pagesPhilippine Hospital Development Plan 2017-2022joric miranda93% (14)
- Vaccine Refusal Forms and Lots of Backup InformationDocument39 pagesVaccine Refusal Forms and Lots of Backup Informationverumlux100% (7)
- 2019 IFOM CSE SIG English PDFDocument4 pages2019 IFOM CSE SIG English PDFMaram KheerNo ratings yet
- Https/www-Uptodate-Com Consultaremota Upb Edu Co/contents/management-Of-CDocument34 pagesHttps/www-Uptodate-Com Consultaremota Upb Edu Co/contents/management-Of-CMichael Amarillo CorreaNo ratings yet
- 2020 Hypertension Evolving From Standardized To PrecisionDocument4 pages2020 Hypertension Evolving From Standardized To PrecisionPeter Albeiro Falla CortesNo ratings yet
- HTN Guidelines 1Document12 pagesHTN Guidelines 1lakshminivas PingaliNo ratings yet
- Treat To Target': Moving Targets From Hypertension, Hyperlipidaemia and Diabetes To Rheumatoid ArthritisDocument3 pagesTreat To Target': Moving Targets From Hypertension, Hyperlipidaemia and Diabetes To Rheumatoid ArthritisMakhyan JibrilNo ratings yet
- 1 s2.0 S000291491730807X MainDocument11 pages1 s2.0 S000291491730807X MainEndru AngelNo ratings yet
- Advances in Anesthesia: Optimal Perioperative Blood Pressure ManagementDocument13 pagesAdvances in Anesthesia: Optimal Perioperative Blood Pressure Managementfabian arassiNo ratings yet
- Prognostic Factors in Pulmonary Arterial Hypertension: Literature ReviewDocument5 pagesPrognostic Factors in Pulmonary Arterial Hypertension: Literature Reviewhuda riyambodoNo ratings yet
- 10 Curva-JcDocument6 pages10 Curva-Jcchandra9000No ratings yet
- Cardiovascular Risk Assessment and Screening in Diabetes: Yanglu ZhaoDocument6 pagesCardiovascular Risk Assessment and Screening in Diabetes: Yanglu ZhaoEward Rod SalNo ratings yet
- HipertensiDocument37 pagesHipertensiValentina PujiNo ratings yet
- Hipertensión SitémicaDocument12 pagesHipertensión SitémicaIván Alejandro Trejo ValdiviezoNo ratings yet
- Diagnosis and Treatment of HTN in Dialysis PatientsDocument12 pagesDiagnosis and Treatment of HTN in Dialysis PatientsalizanNo ratings yet
- 10.1007@s11906 020 01120 7Document11 pages10.1007@s11906 020 01120 7ivenasabillaNo ratings yet
- Variabilitatea TADocument13 pagesVariabilitatea TADaniel StaniloaieNo ratings yet
- Dci 210017Document3 pagesDci 210017Gloria WuNo ratings yet
- Intensive Blood Pressure Lowering: A Practical ReviewDocument8 pagesIntensive Blood Pressure Lowering: A Practical ReviewJorge David Gamez PeñarandaNo ratings yet
- Kanegae 2017Document9 pagesKanegae 2017Kennard Aristo ArifinNo ratings yet
- Estimation of Cardiovascular DiseaseDocument14 pagesEstimation of Cardiovascular DiseaseShree Narayan YadavNo ratings yet
- Aterosclerosis SubclinicaDocument4 pagesAterosclerosis SubclinicaEnzo GonzalezNo ratings yet
- Optimalmedicaltherapyfor Stableischemicheart Diseasein2024: Focus On Blood Pressure and LipidsDocument13 pagesOptimalmedicaltherapyfor Stableischemicheart Diseasein2024: Focus On Blood Pressure and LipidsCarlos Hernan Castañeda RuizNo ratings yet
- Arterial Hypertension e Clinical Trials Update 2021Document11 pagesArterial Hypertension e Clinical Trials Update 2021Dana MNo ratings yet
- Art 1Document11 pagesArt 1Sheyla Karina De La Cruz EscobarNo ratings yet
- Review Article: Investigation On Cardiovascular Risk Prediction Using Physiological ParametersDocument22 pagesReview Article: Investigation On Cardiovascular Risk Prediction Using Physiological ParametersNnaemeka NwobodoNo ratings yet
- Interdisciplinary Assessment and Diagnostic Algo - 2021 - Diabetes Research andDocument6 pagesInterdisciplinary Assessment and Diagnostic Algo - 2021 - Diabetes Research andprobo asmoroNo ratings yet
- WJC 6 728 PDFDocument17 pagesWJC 6 728 PDFvanathyNo ratings yet
- Predictors of Intradialytic Hypertension in Chronic End Stage Renal Dialysis Patients in A Tertiary Government Hospital in Davao CDocument13 pagesPredictors of Intradialytic Hypertension in Chronic End Stage Renal Dialysis Patients in A Tertiary Government Hospital in Davao CSari ChaerunisahNo ratings yet
- ETG-Australian Therapeutic Guidelines 2020 (Part 2) .PDF - OptimizeDocument1,269 pagesETG-Australian Therapeutic Guidelines 2020 (Part 2) .PDF - OptimizeFlavin AmbroseNo ratings yet
- Cerie Llo 2021Document11 pagesCerie Llo 2021Mădălina MitroiuNo ratings yet
- Framing Cardiovascular Disease Event Risk Prediction: EditorialDocument3 pagesFraming Cardiovascular Disease Event Risk Prediction: EditorialGaluh Kresna BayuNo ratings yet
- Benefits and Risks of Antihypertensive Medications in The ElderlyDocument28 pagesBenefits and Risks of Antihypertensive Medications in The ElderlyNasrull BinHzNo ratings yet
- Diabetes Physical Ecamination (Malik y Ananthakrishnan, 2022)Document12 pagesDiabetes Physical Ecamination (Malik y Ananthakrishnan, 2022)Marcelo TrNo ratings yet
- Impact of Baseline Cardiovascular Risk On The Outcomes of Intensive Blood Pressure Intervention: A Post Hoc Analysis of The China Rural Hypertension Control ProjectDocument12 pagesImpact of Baseline Cardiovascular Risk On The Outcomes of Intensive Blood Pressure Intervention: A Post Hoc Analysis of The China Rural Hypertension Control Projectsoy_humanaNo ratings yet
- Hypertension in End-Stage Renal Disease: Eview RticleDocument6 pagesHypertension in End-Stage Renal Disease: Eview RticleGaema MiripNo ratings yet
- New Frontiers Hipertensi Part2Document8 pagesNew Frontiers Hipertensi Part2Eunike_oisNo ratings yet
- Chronic Heart Failure-Part IDocument18 pagesChronic Heart Failure-Part IdrtpkNo ratings yet
- Acute Congestive Heart Failure in The Emergency DepartmentDocument9 pagesAcute Congestive Heart Failure in The Emergency DepartmentAlanNo ratings yet
- Evaluation and Management of Perioperative HypertensionDocument126 pagesEvaluation and Management of Perioperative HypertensionjoelruizmaNo ratings yet
- HF in ElderlyDocument3 pagesHF in ElderlyHadi M.WNo ratings yet
- Definition and Classification of Hypertension - An UpdateDocument4 pagesDefinition and Classification of Hypertension - An UpdateHaidee JavierNo ratings yet
- Research Paper Congestive Heart FailureDocument6 pagesResearch Paper Congestive Heart Failurelzpyreqhf100% (1)
- Heart Disease Literature ReviewDocument9 pagesHeart Disease Literature Reviewjyzapydigip3100% (1)
- Medscape Cardiology: Authors and DisclosuresDocument29 pagesMedscape Cardiology: Authors and DisclosuresPopo SariNo ratings yet
- Stroke BP VariabilityDocument22 pagesStroke BP Variabilitylakshminivas PingaliNo ratings yet
- Serum Lipid Profile and Its Association With Hypertension in BangladeshDocument6 pagesSerum Lipid Profile and Its Association With Hypertension in BangladeshEvy Afrianti DariseNo ratings yet
- Standards of Medical Care in Diabetesd2020: 10. Cardiovascular Disease and Risk ManagementDocument24 pagesStandards of Medical Care in Diabetesd2020: 10. Cardiovascular Disease and Risk Managementcath lauuuNo ratings yet
- Cardiac Self-Efficacy and Quality of Life in Patients With Coronary Heart Disease: A Cross-Sectional Study From PalestineDocument13 pagesCardiac Self-Efficacy and Quality of Life in Patients With Coronary Heart Disease: A Cross-Sectional Study From Palestineشبلي غرايبهNo ratings yet
- 63 - Original ArticleDocument5 pages63 - Original ArticlechairulNo ratings yet
- 2015 Article 244Document8 pages2015 Article 244nasar adenNo ratings yet
- C-Reactive Protein and Cardiovascular Diseases-Is It Ready For Primetime?Document7 pagesC-Reactive Protein and Cardiovascular Diseases-Is It Ready For Primetime?dastgirrajaNo ratings yet
- Nihms 1520567Document30 pagesNihms 15205672130020043 RIDHO INAYAHNo ratings yet
- Left Ventricular Mass As A Predictor of Cardiovascular DiseaseDocument19 pagesLeft Ventricular Mass As A Predictor of Cardiovascular DiseaseerikafebriyanarNo ratings yet
- Clinicc Intermittent ClaudicationDocument8 pagesClinicc Intermittent ClaudicationTudor DumitrascuNo ratings yet
- Jurnal HipertensiDocument5 pagesJurnal HipertensiRanhie Pen'ned CendhirhieNo ratings yet
- JurnalDocument3 pagesJurnalalvinaevaniaNo ratings yet
- Article 164163-PrintDocument22 pagesArticle 164163-PrintIribuka JonathanNo ratings yet
- BMC Public Health: Beyond Inpatient and Outpatient Care: Alternative Model For Hypertension ManagementDocument3 pagesBMC Public Health: Beyond Inpatient and Outpatient Care: Alternative Model For Hypertension ManagementMarcovicFualeMcdaviesNo ratings yet
- Ashok Sarma DPTDocument36 pagesAshok Sarma DPTprnshsarmaNo ratings yet
- Arterial Stiffness: A Review in Type 2 Diabetes: Mariella Catalano, Giovanni Scandale and Gabriel DimitrovDocument14 pagesArterial Stiffness: A Review in Type 2 Diabetes: Mariella Catalano, Giovanni Scandale and Gabriel DimitrovAnanta SwargiaryNo ratings yet
- Chronic Kidney Disease and Its ComplicationsDocument6 pagesChronic Kidney Disease and Its ComplicationsmedicalNo ratings yet
- Navigating Acute Heart Failure: Comprehensive Insights and Holistic ApproachesFrom EverandNavigating Acute Heart Failure: Comprehensive Insights and Holistic ApproachesNo ratings yet
- Config Measure Tab Aortic Folder LVOT Trace Folder Make Sure LVOT VTI Is TickedDocument1 pageConfig Measure Tab Aortic Folder LVOT Trace Folder Make Sure LVOT VTI Is TickedOnon EssayedNo ratings yet
- The End of Metabolic SyndromeDocument6 pagesThe End of Metabolic SyndromeOnon EssayedNo ratings yet
- SITAGLIPTINDocument15 pagesSITAGLIPTINOnon EssayedNo ratings yet
- Life Style ModificationDocument11 pagesLife Style ModificationOnon Essayed100% (1)
- Surveillance: Budi SetiawanDocument14 pagesSurveillance: Budi SetiawanAnonymous XGE6XwHZNo ratings yet
- Geria Prefinals 1Document5 pagesGeria Prefinals 1BEN-SHARIEF ASULANo ratings yet
- NUR403 Assiginment 2Document8 pagesNUR403 Assiginment 2KwanNingYuNo ratings yet
- Prevalence of Kennedy Classification in Partially Edentulous Patients - A Retrospective StudyDocument7 pagesPrevalence of Kennedy Classification in Partially Edentulous Patients - A Retrospective StudyAnca MocanuNo ratings yet
- Lesson Plan On SinusitisDocument18 pagesLesson Plan On SinusitisVaishali SinghNo ratings yet
- Aer 20180284Document31 pagesAer 20180284Nathalie FytrouNo ratings yet
- PAKET 21 Pengetahuan Dan Pemahaman Umum (Inggris)Document2 pagesPAKET 21 Pengetahuan Dan Pemahaman Umum (Inggris)Felicia MaharaniNo ratings yet
- Basic Principles of Wound ManagementDocument26 pagesBasic Principles of Wound ManagementAlina Nica GurgutaNo ratings yet
- Unintentional Injury Prevention, First Aid and SafetyDocument25 pagesUnintentional Injury Prevention, First Aid and SafetyCasNo ratings yet
- Substance Abuse PDFDocument24 pagesSubstance Abuse PDFABHINAVNo ratings yet
- NURS FPX 6030 Assessment 2 Problem Statement (PICOT)Document7 pagesNURS FPX 6030 Assessment 2 Problem Statement (PICOT)joohnsmith070No ratings yet
- Medication - ALT-Template Polythene GlycolDocument1 pageMedication - ALT-Template Polythene GlycolNancyAmissahNo ratings yet
- Dr. Stephen D, M.D.: CanalplastyDocument1 pageDr. Stephen D, M.D.: CanalplastyMariska KaurranyNo ratings yet
- Primary Biliary Cirrhosis Primary Sclerosing CholangitisDocument44 pagesPrimary Biliary Cirrhosis Primary Sclerosing CholangitisTK RowlingNo ratings yet
- Sympathetic Ophthalmia: Ocular Immunology and InflammationDocument4 pagesSympathetic Ophthalmia: Ocular Immunology and InflammationOskar MartinezNo ratings yet
- Cephalosporins GenerationDocument7 pagesCephalosporins GenerationSam SmileyNo ratings yet
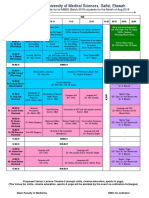
- Lunch: Foundation Course Time Table For Ist MBBS (Batch 2019) Students For The Month of Aug.2019Document2 pagesLunch: Foundation Course Time Table For Ist MBBS (Batch 2019) Students For The Month of Aug.2019Vishal SinghNo ratings yet
- Dr. R. W. Bernard - Science Discovers The Psychological Value of ContinenceDocument31 pagesDr. R. W. Bernard - Science Discovers The Psychological Value of ContinenceOliveros2012No ratings yet
- Economic Burden of Vertigo A Systematic ReviewDocument14 pagesEconomic Burden of Vertigo A Systematic ReviewMartin Ramos AlvaradoNo ratings yet
- Dennie-Morgan Fold Plus Dark Circles: Suspect Atopy at First SightDocument1 pageDennie-Morgan Fold Plus Dark Circles: Suspect Atopy at First Sight2readNo ratings yet
- Top 10 Most Read AORN Journal Articles PDFDocument107 pagesTop 10 Most Read AORN Journal Articles PDFsriyanto ibsNo ratings yet
- Infection ControlDocument19 pagesInfection Controlneven.mortagaNo ratings yet
- Basic Radiation Oncology Beyzadeoglu 2 Ed 2022Document541 pagesBasic Radiation Oncology Beyzadeoglu 2 Ed 2022Alexandr MateașNo ratings yet
- Exam MaterialsDocument5 pagesExam MaterialsMarim Esamy100% (1)
- SIDA. VIRUS O DROGA INDUCIDA-Springer Netherlands (1996)Document353 pagesSIDA. VIRUS O DROGA INDUCIDA-Springer Netherlands (1996)mdn sdmsNo ratings yet
- Talar Cyst: JSM Foot and AnkleDocument2 pagesTalar Cyst: JSM Foot and Anklenpr00No ratings yet
- Sutras of Ashthanga Hrydayam & Ashthanga SangrahaDocument18 pagesSutras of Ashthanga Hrydayam & Ashthanga SangrahasanjeevkryNo ratings yet