Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
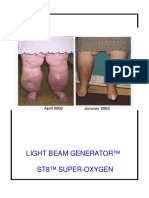
- Wow Light Beam Generator St8 Super-OxygenDocument44 pagesWow Light Beam Generator St8 Super-OxygenMilan Valachovic100% (1)
- Sensory Integration Therapy Auditory Integration Training Ohp PDFDocument10 pagesSensory Integration Therapy Auditory Integration Training Ohp PDFDamayanti ThapaNo ratings yet
- Food Science and Human Nutrition: Undergraduate StudyDocument17 pagesFood Science and Human Nutrition: Undergraduate StudyMulubrhan OkbaiNo ratings yet
- ARANGUEZ NORTH SECONDARY SCHOO1. IIdocxDocument8 pagesARANGUEZ NORTH SECONDARY SCHOO1. IIdocxDevi RambaranNo ratings yet
- 6 Week Lift Like A Girl ProgramDocument15 pages6 Week Lift Like A Girl ProgramGuillaume VingtcentNo ratings yet
- Data Statistics Draftv1Document35 pagesData Statistics Draftv1Jack PNo ratings yet
- Vaidyam For Web Vol5 Issue4Document44 pagesVaidyam For Web Vol5 Issue4SBSGLOBAL100% (1)
- Progress Report Overview: Student: Akileshwar Reddy MenduDocument8 pagesProgress Report Overview: Student: Akileshwar Reddy MenduAkhil ReddyNo ratings yet
- Hematopoietic Acute Radiation Syndrome (Aplastic Anemia, Bone Marrow Syndrome)Document32 pagesHematopoietic Acute Radiation Syndrome (Aplastic Anemia, Bone Marrow Syndrome)Dmitri PopovNo ratings yet
- Zeva 1 - MSDSDocument6 pagesZeva 1 - MSDSRowi ArifudinNo ratings yet
- Individuals' Long Term Use of Cognitive Behavioural Skills To Manage TheirDocument20 pagesIndividuals' Long Term Use of Cognitive Behavioural Skills To Manage TheircawinNo ratings yet
- Types of Cerebral PalsyDocument6 pagesTypes of Cerebral PalsySahil SahniNo ratings yet
- Pre-Requisite Programs (PRP) & Critical Control Points (CCP) PDFDocument55 pagesPre-Requisite Programs (PRP) & Critical Control Points (CCP) PDFVenkat SujithNo ratings yet
- Saurashtra ListDocument200 pagesSaurashtra Listvadoliya umeshNo ratings yet
- The Role of Complementary and Alternative Therapies in Managing Rheumatoid ArthritisDocument1 pageThe Role of Complementary and Alternative Therapies in Managing Rheumatoid Arthritisjelena_bojovic1No ratings yet
- Classification SL - No Disease Rickettsial Agent Insect Vector Mammalian ReservoirsDocument4 pagesClassification SL - No Disease Rickettsial Agent Insect Vector Mammalian ReservoirsGetom NgukirNo ratings yet
- Example Review and Critique of A Qualitative StudyDocument6 pagesExample Review and Critique of A Qualitative StudyWinnifer KongNo ratings yet
- Announcement PKBDocument8 pagesAnnouncement PKBlo tek huiNo ratings yet
- Occupational Stress OcpdDocument49 pagesOccupational Stress Ocpdbakaipkkedah100% (1)
- Open Heart Surgery JournalDocument3 pagesOpen Heart Surgery Journalapi-546517574No ratings yet
- Promoting Nutrtional Health in ToddlersDocument5 pagesPromoting Nutrtional Health in ToddlersMark oliver GonzalesNo ratings yet
- Injury Prevention in Youth Sports.Document5 pagesInjury Prevention in Youth Sports.drmanupvNo ratings yet
- Itzayana Carranza ResumeDocument3 pagesItzayana Carranza Resumeapi-612292594No ratings yet
- Docsity Detailed Lesson Plan 5Document4 pagesDocsity Detailed Lesson Plan 5Sydie MoredoNo ratings yet
- Nation2009 COLISTINDocument9 pagesNation2009 COLISTINSherly CharleneNo ratings yet
- Swansons Family Medicine Review 8E Jul 6 2016 - 032335632X - Mcgraw Hill Alfred F Tallia Full ChapterDocument68 pagesSwansons Family Medicine Review 8E Jul 6 2016 - 032335632X - Mcgraw Hill Alfred F Tallia Full Chapterwilliam.mendez560100% (8)
- HF ArticleDocument14 pagesHF ArticleDR. Shobhit RajNo ratings yet
- Minutes of The Infection Control Committee MeetingDocument3 pagesMinutes of The Infection Control Committee MeetingnanaNo ratings yet
- Ethics, Safety, Society, Environment Assessment RubricDocument2 pagesEthics, Safety, Society, Environment Assessment Rubricjose saucedaNo ratings yet