Download as pdf or txt
You might also like
- Differences Between Biological and Psychosocial Interventions.Document4 pagesDifferences Between Biological and Psychosocial Interventions.aval123No ratings yet
- Tutorial 07-Operations and Productivity PDFDocument2 pagesTutorial 07-Operations and Productivity PDFKhiren Menon100% (1)
- Edo Shonin, William Van Gordon, and Mark D. GriffithsDocument4 pagesEdo Shonin, William Van Gordon, and Mark D. GriffithsDr Edo ShoninNo ratings yet
- The Effectiveness of Behavioural Therapy For The Treatment of Depression in Older Adults: A Meta-AnalysisDocument11 pagesThe Effectiveness of Behavioural Therapy For The Treatment of Depression in Older Adults: A Meta-Analysisnini345No ratings yet
- The Effectiveness of Mindfulness-Based InterventionsDocument16 pagesThe Effectiveness of Mindfulness-Based InterventionsMaria GabrielaNo ratings yet
- 2010 - Hoffman - The Effect of Mindfulness Based Therapy On Anxiety and DepressionDocument15 pages2010 - Hoffman - The Effect of Mindfulness Based Therapy On Anxiety and DepressionFabián MaeroNo ratings yet
- How Social Psychology Can Improve PsychotherapyDocument8 pagesHow Social Psychology Can Improve PsychotherapyNeytiri PamtseoNo ratings yet
- Mindfulness-Based Treatment For Bipolar Disorder: A Systematic Review of The LiteratureDocument27 pagesMindfulness-Based Treatment For Bipolar Disorder: A Systematic Review of The LiteratureFilza RamdhaniNo ratings yet
- Mindfulness-Based Treatment For Bipolar Disorder: A Systematic Review of The LiteratureDocument26 pagesMindfulness-Based Treatment For Bipolar Disorder: A Systematic Review of The Literature290971No ratings yet
- PDF Michalak Et Al 2019 Mindfulness in Individual TherapyDocument13 pagesPDF Michalak Et Al 2019 Mindfulness in Individual Therapyluis.callegarioNo ratings yet
- Safety of MBIsDocument14 pagesSafety of MBIsTony PignoliNo ratings yet
- Wilson Et Al., 2019Document17 pagesWilson Et Al., 2019Administrador ContaNo ratings yet
- The Effects of Mindfulness Meditation - A Meta-Analysis PDFDocument16 pagesThe Effects of Mindfulness Meditation - A Meta-Analysis PDFRoxy Shira AdiNo ratings yet
- How Effective Is Cognitive Behavioural TherapyDocument5 pagesHow Effective Is Cognitive Behavioural TherapyNadia MuhammadNo ratings yet
- 40631665-Review Mindfulness Si Cancer PDFDocument10 pages40631665-Review Mindfulness Si Cancer PDFadri90No ratings yet
- A Feasibility Study of Mindfulness-Based CognitiveDocument17 pagesA Feasibility Study of Mindfulness-Based CognitiveGise MagdaNo ratings yet
- The Impact of Well - Being Therapy On Symptoms of DepressionDocument8 pagesThe Impact of Well - Being Therapy On Symptoms of DepressionEstefany ReyesNo ratings yet
- 2009 Dianne Ledesma - Mindfulness-Based Stress Reduction and CancerDocument10 pages2009 Dianne Ledesma - Mindfulness-Based Stress Reduction and Cancernermal93No ratings yet
- Hayes Et Al (2018) - Process-Based CBT.Document57 pagesHayes Et Al (2018) - Process-Based CBT.leidy7No ratings yet
- BradshawDocument9 pagesBradshawFatur AkhiNo ratings yet
- Antipsychotic Treatment Beyond AntipsychoticsDocument10 pagesAntipsychotic Treatment Beyond AntipsychoticsbssNo ratings yet
- Baer, R., Crane, C., Miller, E., Kuyken, W. (2019) - Doing No Harm in Mindfulness-Based Programs Conceptual Issues and Empirical Findings.Document14 pagesBaer, R., Crane, C., Miller, E., Kuyken, W. (2019) - Doing No Harm in Mindfulness-Based Programs Conceptual Issues and Empirical Findings.kbmatekNo ratings yet
- Long-Term Efficacy of Psychosocial Treatments For Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic ReviewDocument24 pagesLong-Term Efficacy of Psychosocial Treatments For Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Reviewaastha panthNo ratings yet
- MotivtkDocument11 pagesMotivtkReiza IndraNo ratings yet
- Impact of A MindfulnessDocument2 pagesImpact of A MindfulnessValentina Denise Dávila SosaNo ratings yet
- The Effect of Mindfulness-Based Therapy On Symptoms of Anxiety and Depression in Adults Cancer PatientsDocument14 pagesThe Effect of Mindfulness-Based Therapy On Symptoms of Anxiety and Depression in Adults Cancer PatientsAndréa Carolina BenitesNo ratings yet
- Mind Boy MedicineDocument10 pagesMind Boy MedicineCody WilliamsNo ratings yet
- A Systematic Review On The Effectiveness of DialecDocument12 pagesA Systematic Review On The Effectiveness of DialecLarissa AndradeNo ratings yet
- A Sorrow Shared Is A Sorrow Halved A Three-Arm Randomized Controlled Trial Comparing Internet-Based Clinician-Guided Individual Versus Group Treatment For Social Anxiety DisorderDocument45 pagesA Sorrow Shared Is A Sorrow Halved A Three-Arm Randomized Controlled Trial Comparing Internet-Based Clinician-Guided Individual Versus Group Treatment For Social Anxiety DisorderZhewen TangNo ratings yet
- Meditation Mindfulness and Acceptance Methods in Psychotherapy A Systematic ReviewDocument14 pagesMeditation Mindfulness and Acceptance Methods in Psychotherapy A Systematic ReviewFernando Lapuente-GarcíaNo ratings yet
- Evidence-Based Practice PaperDocument16 pagesEvidence-Based Practice Paperapi-599394340No ratings yet
- AAA Early - Response - Review - 2019 - Pre-PrintDocument36 pagesAAA Early - Response - Review - 2019 - Pre-PrintGONZALO SEBASTIAN LOBOS SEPULVEDANo ratings yet
- Running Head: Mechanisms and Outcomes of Metta Meditation 1Document38 pagesRunning Head: Mechanisms and Outcomes of Metta Meditation 1santo sepangNo ratings yet
- Persons Case Formulation ArticleDocument11 pagesPersons Case Formulation ArticleMarco Sousa100% (2)
- 1 s2.0 S0165032721013860 MainDocument9 pages1 s2.0 S0165032721013860 MainElvira FerNo ratings yet
- Clinical Efficacy of A Combined AcceptanDocument16 pagesClinical Efficacy of A Combined AcceptanEmanuel EspinosaNo ratings yet
- Head and Neck CancerDocument15 pagesHead and Neck CancerFlorinaNo ratings yet
- Reyes-Ortega 2019 ACT or DBT or Both - With Borderline Personality DisorderDocument16 pagesReyes-Ortega 2019 ACT or DBT or Both - With Borderline Personality DisorderMario Lopez PadillaNo ratings yet
- Positive Psychology Interventions: A Meta-Analysis of Randomized Controlled StudiesDocument20 pagesPositive Psychology Interventions: A Meta-Analysis of Randomized Controlled StudiesDipin MutrejaNo ratings yet
- Vi Research Proposal Outline 26 June 2019Document6 pagesVi Research Proposal Outline 26 June 2019ninaNo ratings yet
- Research Paper (Final Draft) - MATEO RODRIGUEZDocument10 pagesResearch Paper (Final Draft) - MATEO RODRIGUEZMATEO SEBASTIAN RODRIGUEZ TORRESNo ratings yet
- A Systematic Review On The Effectiveness of Dialectical Behavior Therapy For Improving Mood Symptoms in Bipolar DisordersDocument11 pagesA Systematic Review On The Effectiveness of Dialectical Behavior Therapy For Improving Mood Symptoms in Bipolar DisordersLauraLoaizaNo ratings yet
- Appi Ajp 162 12 2220Document13 pagesAppi Ajp 162 12 2220LosineKrishnaNo ratings yet
- Perfeccionismo Ap y TocDocument15 pagesPerfeccionismo Ap y TocMiriam JaraNo ratings yet
- RCT-Meditation 4 FMSDocument21 pagesRCT-Meditation 4 FMSEnmanuel orellanaNo ratings yet
- .Au-The Effectiveness of Body-Oriented Psychotherapy A Review of The LiteratureDocument22 pages.Au-The Effectiveness of Body-Oriented Psychotherapy A Review of The Literaturealexandra_gomes07No ratings yet
- The Empirical Status of Psychoanalytic Treatment (Article) Author David KealyDocument7 pagesThe Empirical Status of Psychoanalytic Treatment (Article) Author David KealyVi HaNo ratings yet
- UC San Francisco Previously Published WorksDocument10 pagesUC San Francisco Previously Published WorksAisyah T'cungkringNo ratings yet
- Thompson Et Al. (2021) - Internet-Based Acceptance and Commitment TherapyDocument16 pagesThompson Et Al. (2021) - Internet-Based Acceptance and Commitment TherapyDaniel Garvi de Castro100% (1)
- What Is The Impact of Mental Health-Related Stigma On Help-Seeking? A Systematic Review of Quantitative and Qualitative StudiesDocument49 pagesWhat Is The Impact of Mental Health-Related Stigma On Help-Seeking? A Systematic Review of Quantitative and Qualitative Studiesjulia torNo ratings yet
- Estructura, Correlatos y CambiosDocument44 pagesEstructura, Correlatos y CambiosMiriam JaraNo ratings yet
- Effects of Attachment-Based Compassion Therapy (ABCT) On Self-Compassion and Attachment Style in Healthy PeopleDocument12 pagesEffects of Attachment-Based Compassion Therapy (ABCT) On Self-Compassion and Attachment Style in Healthy PeopleAoiNo ratings yet
- Mindfulness-Based Cognitive Therapy For OCD: Stand-Alone and Post-CBT Augmentation ApproachesDocument22 pagesMindfulness-Based Cognitive Therapy For OCD: Stand-Alone and Post-CBT Augmentation ApproachesMiriamNo ratings yet
- Rschgate Psychoisi TX W TherDocument11 pagesRschgate Psychoisi TX W Therscribd4kmhNo ratings yet
- Predicting Individual Preferences in Mindfulness Techniques Using Personality TraitsDocument8 pagesPredicting Individual Preferences in Mindfulness Techniques Using Personality TraitsAndrés Camilo Ramírez AarónNo ratings yet
- Mindfulness For ParentsDocument2 pagesMindfulness For Parents9837589493100% (1)
- Comparing The Efficacy of Acceptance andDocument16 pagesComparing The Efficacy of Acceptance andgoldieavodaNo ratings yet
- Mindfulness Based Interventions in Secondary Education A Qualitative Systematic Review Intervenciones Basadas en Mindfulness en Educaci N SecundariaDocument39 pagesMindfulness Based Interventions in Secondary Education A Qualitative Systematic Review Intervenciones Basadas en Mindfulness en Educaci N SecundariaJoan PozoNo ratings yet
- Measuring MindfulnessDocument22 pagesMeasuring MindfulnessRemy Løw100% (1)
- An Integrative Paradigm for Mental Health Care: Ideas and Methods Shaping the FutureFrom EverandAn Integrative Paradigm for Mental Health Care: Ideas and Methods Shaping the FutureNo ratings yet
- Mandala of The Present MomentDocument5 pagesMandala of The Present MomentDr Edo ShoninNo ratings yet
- The Four Types of PsychologistDocument5 pagesThe Four Types of PsychologistDr Edo Shonin100% (1)
- Mindfulness For DogsDocument6 pagesMindfulness For DogsDr Edo ShoninNo ratings yet
- Do You Know Who I AmDocument3 pagesDo You Know Who I AmDr Edo ShoninNo ratings yet
- Mindfulness in Mental Health: A Critical ReflectionDocument5 pagesMindfulness in Mental Health: A Critical ReflectionDr Edo ShoninNo ratings yet
- Keeping It TogetherDocument4 pagesKeeping It TogetherDr Edo ShoninNo ratings yet
- The Heart of Buddhism - EmptinessDocument7 pagesThe Heart of Buddhism - EmptinessDr Edo ShoninNo ratings yet
- Can A Buddha Become AngryDocument6 pagesCan A Buddha Become AngryDr Edo ShoninNo ratings yet
- Sex - A Buddhist PerspectiveDocument6 pagesSex - A Buddhist PerspectiveDr Edo ShoninNo ratings yet
- Deconstructing SelfDocument4 pagesDeconstructing SelfDr Edo ShoninNo ratings yet
- Practical Tips For Teaching Mindfulness To Children and Adolescents in School-Based SettingsDocument4 pagesPractical Tips For Teaching Mindfulness To Children and Adolescents in School-Based SettingsDr Edo ShoninNo ratings yet
- Letting Go - The Story of Two Monks and A Naked LadyDocument3 pagesLetting Go - The Story of Two Monks and A Naked LadyDr Edo ShoninNo ratings yet
- A Bubble in The WindDocument1 pageA Bubble in The WindDr Edo ShoninNo ratings yet
- Technical Interview Questions - Active DirectoryDocument74 pagesTechnical Interview Questions - Active DirectoryMadhava SwamyNo ratings yet
- Sat Sankalp EnglishDocument2 pagesSat Sankalp Englishrohan100% (1)
- Education Can Become Transformative When Teachers and Students Synthesize Information Across Subjects and Experiences, Critically Weigh SignificantlyDocument5 pagesEducation Can Become Transformative When Teachers and Students Synthesize Information Across Subjects and Experiences, Critically Weigh Significantlydengs leeNo ratings yet
- Ann S Photo Shop Is A Retail Store That Sells CamerasDocument1 pageAnn S Photo Shop Is A Retail Store That Sells CamerasMuhammad ShahidNo ratings yet
- Newborn Studio Guide by Jessica G. PhotographyDocument13 pagesNewborn Studio Guide by Jessica G. PhotographyClau ppNo ratings yet
- MonitersDocument25 pagesMonitersJaveed AhamedNo ratings yet
- Mean, Median and Mode 1 PDFDocument16 pagesMean, Median and Mode 1 PDFMbalieZee0% (1)
- Va 2 19025777Document19 pagesVa 2 19025777api-431932152No ratings yet
- Analogy - Verbal Reasoning Questions and Answers Page 4Document2 pagesAnalogy - Verbal Reasoning Questions and Answers Page 4Palak JioNo ratings yet
- Godrej and Boyce Corporate ProfileDocument2 pagesGodrej and Boyce Corporate ProfileAyushi JainNo ratings yet
- India Data Center OpportunityDocument7 pagesIndia Data Center OpportunitysharatjuturNo ratings yet
- Military Engineer Services Notice Inviting Tender (Nit)Document14 pagesMilitary Engineer Services Notice Inviting Tender (Nit)jatanNo ratings yet
- Fred Review 16Document8 pagesFred Review 16Justin HsuNo ratings yet
- 1 s2.0 S0196890417302509 MainDocument11 pages1 s2.0 S0196890417302509 MainCHELIN_2305No ratings yet
- WHO IVB 11.09 Eng PDFDocument323 pagesWHO IVB 11.09 Eng PDFniaaseepNo ratings yet
- Rehab-Plans-and-Exercises Hip-Arthroscopy Protocol-For-Physiotherapy-Following-SurgeryDocument2 pagesRehab-Plans-and-Exercises Hip-Arthroscopy Protocol-For-Physiotherapy-Following-SurgeryMellow Moon RecordsNo ratings yet
- Gramsci and HegemonyDocument9 pagesGramsci and HegemonyAbdelhak SaddikNo ratings yet
- Coe 2Document8 pagesCoe 2Jean Lindley JosonNo ratings yet
- Jerkins The FounderDocument15 pagesJerkins The FounderRifqi Khairul AnamNo ratings yet
- Purpose RediscoveredDocument102 pagesPurpose RediscoveredErnest NguboNo ratings yet
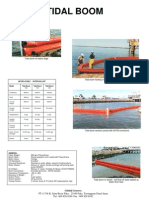
- Tidal Boom at Waters EdgeDocument1 pageTidal Boom at Waters Edgeapi-3703371No ratings yet
- Laporan MekanikDocument23 pagesLaporan MekanikNofrinto FloryNo ratings yet
- Critikon Dinamap Compact - Service Manual 2Document78 pagesCritikon Dinamap Compact - Service Manual 2Ayaovi JorlauNo ratings yet
- Zanskar Expedition Himalaya Com MonkDocument1 pageZanskar Expedition Himalaya Com MonkIvan IvanicNo ratings yet
- Ict4D Project Management Methodology of Sustainable Development GoalsDocument66 pagesIct4D Project Management Methodology of Sustainable Development GoalsJohn J. MacasioNo ratings yet
- CBN BrochureDocument16 pagesCBN BrochuredunnyhalitionNo ratings yet
- 1969 SP-51 RCA Power CircuitsDocument452 pages1969 SP-51 RCA Power CircuitsasccorreaNo ratings yet
- Implementing BenefitsDocument314 pagesImplementing Benefitsmhrao2000100% (1)
- Live Partition Mobility: Power SystemsDocument196 pagesLive Partition Mobility: Power Systemsmevtorres1977No ratings yet