Download as doc, pdf, or txt
You might also like
- MCB 252 Final Exam Study GuideDocument62 pagesMCB 252 Final Exam Study GuideJay ZNo ratings yet
- NAP Gen. Circular 3 GRDS For LGUsDocument36 pagesNAP Gen. Circular 3 GRDS For LGUsquickmelt03No ratings yet
- 5 Cyto AbnormalDocument9 pages5 Cyto AbnormalMerli Ann Joyce CalditoNo ratings yet
- Pelvis and Perineum Clinical CorrelationDocument4 pagesPelvis and Perineum Clinical CorrelationKeesha Mariel AlimonNo ratings yet
- Pathology of NoaDocument164 pagesPathology of NoaAnonymous milwFDXNo ratings yet
- 1.1 Sensory-Motor Skills Involve The Process of Receiving InformationDocument5 pages1.1 Sensory-Motor Skills Involve The Process of Receiving InformationTshepo MolotoNo ratings yet
- Eppd-A Discourse CommunityDocument11 pagesEppd-A Discourse Communityapi-254655486No ratings yet
- Actinic Keratosis: (Aka Bowen's Disease)Document5 pagesActinic Keratosis: (Aka Bowen's Disease)fadoNo ratings yet
- Commensal AmoebaDocument2 pagesCommensal AmoebaCoy NuñezNo ratings yet
- Bacterial Infections of The SkinDocument9 pagesBacterial Infections of The Skinbeia21No ratings yet
- 2011 07 Microbiology Mycobacterium Skin InfectionDocument6 pages2011 07 Microbiology Mycobacterium Skin InfectionCristinaConcepcionNo ratings yet
- The Complement SystemDocument4 pagesThe Complement SystemExamville.com100% (1)
- Essential Update: FDA Approves First Test To Predict AKI in Critically Ill PatientsDocument5 pagesEssential Update: FDA Approves First Test To Predict AKI in Critically Ill PatientsRika Ariyanti SaputriNo ratings yet
- Chronic Inflammatory Dermatoses Inflammatory Blistering DisordersDocument4 pagesChronic Inflammatory Dermatoses Inflammatory Blistering DisordersspringdingNo ratings yet
- DermDocument10 pagesDermyassrmarwaNo ratings yet
- Nephrotic Syndrome WikipediaDocument10 pagesNephrotic Syndrome WikipediaJohn KevlarNo ratings yet
- Cycle CellDocument16 pagesCycle CellRohingya EnglishNo ratings yet
- Renal SyndromeDocument13 pagesRenal SyndromeAndreas KristianNo ratings yet
- University of Santo Tomas: Faculty of Pharmacy - Department of Medical TechnologyDocument7 pagesUniversity of Santo Tomas: Faculty of Pharmacy - Department of Medical TechnologyWynlor AbarcaNo ratings yet
- Abdominal Wall, Omentum, Mesentery, RetroperitoneumDocument6 pagesAbdominal Wall, Omentum, Mesentery, RetroperitoneumMon Ordona De GuzmanNo ratings yet
- The Immune System OhtDocument6 pagesThe Immune System OhtKa-Shun Leung100% (1)
- Hematology Abnormal White Blood CellDocument4 pagesHematology Abnormal White Blood CellBryan James LinNo ratings yet
- Anterior Abdominal WallDocument5 pagesAnterior Abdominal WallAnonymous 2TzM1ZNo ratings yet
- SYPHYLISDocument1 pageSYPHYLISkhadzxNo ratings yet
- Vertebral Artery DissectionDocument2 pagesVertebral Artery DissectionTom MallinsonNo ratings yet
- Cancer EpigeneticsDocument48 pagesCancer EpigeneticsIqra SultanNo ratings yet
- Screening Test For Phagocytic Engulfment: DiapedesisDocument2 pagesScreening Test For Phagocytic Engulfment: DiapedesisBianca ANo ratings yet
- Midterm Chapter7Document43 pagesMidterm Chapter7Frances FranciscoNo ratings yet
- Haematology SAQDocument16 pagesHaematology SAQPowell KitagwaNo ratings yet
- Chapter 3 Genetic VariationDocument21 pagesChapter 3 Genetic VariationAbdulkarimNo ratings yet
- Iron Metabolism: DR Mukhtiar BaigDocument58 pagesIron Metabolism: DR Mukhtiar BaigdrmukhtiarbaigNo ratings yet
- Goljan Live Notes Day 1Document5 pagesGoljan Live Notes Day 1Daniyal AzmatNo ratings yet
- Hemostasis and Thrombosis: OutlineDocument11 pagesHemostasis and Thrombosis: OutlineManila MedNo ratings yet
- Harrisons: Introduction To Infectious DiseasesDocument3 pagesHarrisons: Introduction To Infectious Diseasesapi-3704562No ratings yet
- (MICROA - 2.1) Myeloid Tissue HistologyDocument6 pages(MICROA - 2.1) Myeloid Tissue HistologyHenryboi CañasNo ratings yet
- CNS PathologyDocument126 pagesCNS PathologyMichael-John FayNo ratings yet
- Anti EpCAM Antibodies For Detection of Metastatic CarcinomaDocument6 pagesAnti EpCAM Antibodies For Detection of Metastatic CarcinomaIulia Alexandra PredaNo ratings yet
- 1 Ana Intro Finals September 16 LaygoDocument3 pages1 Ana Intro Finals September 16 LaygombdelenaNo ratings yet
- Patho CA - Acute PancreatitisDocument1 pagePatho CA - Acute PancreatitisKNo ratings yet
- Pathology B - Gastrointestinal Tract (Esguerra, 2015)Document18 pagesPathology B - Gastrointestinal Tract (Esguerra, 2015)Ars MoriendiNo ratings yet
- Module2 ImmunologyDocument33 pagesModule2 ImmunologyAygul RamankulovaNo ratings yet
- PathologyDocument30 pagesPathologyTenorski baritonNo ratings yet
- Skin PathogensDocument4 pagesSkin PathogensEhi EdialeNo ratings yet
- Anat 4.3 GIT Histo - ZuluetaDocument8 pagesAnat 4.3 GIT Histo - Zuluetalovelots1234No ratings yet
- Introduction To HaemostasisDocument18 pagesIntroduction To Haemostasiswatchme3No ratings yet
- ENDOCRINE PATHOLOGY WebpathDocument35 pagesENDOCRINE PATHOLOGY Webpathapi-3766657No ratings yet
- Lymphoma: Pro - Dr.Ahmed EisaDocument45 pagesLymphoma: Pro - Dr.Ahmed EisaOmar Mohammed100% (1)
- Para Compre 2Document17 pagesPara Compre 2serainie maiNo ratings yet
- Neuropathology: FK UisuDocument28 pagesNeuropathology: FK UisuAnggi WahyuNo ratings yet
- Patho Final Study GuideDocument55 pagesPatho Final Study GuideBritNo ratings yet
- Histology Viscus Flow ChartDocument1 pageHistology Viscus Flow ChartNaser Hamdi ZalloumNo ratings yet
- Cytogenetics Note PDFDocument14 pagesCytogenetics Note PDFMerjema Bahtanović100% (1)
- Structural Biology of HIVDocument31 pagesStructural Biology of HIVLaura TapiaNo ratings yet
- Casts inDocument1 pageCasts ingregoryvoNo ratings yet
- Cytogenetics Course PackDocument29 pagesCytogenetics Course Packanonymous squashNo ratings yet
- Gametogenesis and Fertilization - Bio 30 PDFDocument2 pagesGametogenesis and Fertilization - Bio 30 PDFJoseph Paguio100% (1)
- Leukemias & Lymphomas - HY USMLEDocument87 pagesLeukemias & Lymphomas - HY USMLEMatt McGlothlinNo ratings yet
- Small Intestine 01 PDFDocument9 pagesSmall Intestine 01 PDFfadoNo ratings yet
- Chapter 13 Neoplastic Proliferations of White CellsDocument16 pagesChapter 13 Neoplastic Proliferations of White CellsOmar100% (1)
- Renal BiopsyDocument53 pagesRenal Biopsybusiness onlyyouNo ratings yet
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Case Report: Pulmonary Sequestration: A Case Report and Literature ReviewDocument4 pagesCase Report: Pulmonary Sequestration: A Case Report and Literature Reviewjo_jo_maniaNo ratings yet
- Canadian Contraception ConsensusDocument14 pagesCanadian Contraception Consensusjo_jo_maniaNo ratings yet
- Donordarah PDFDocument1 pageDonordarah PDFjo_jo_maniaNo ratings yet
- Donor DarahDocument1 pageDonor Darahjo_jo_maniaNo ratings yet
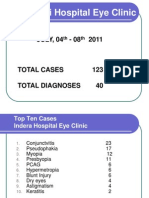
- NEW Weekly Indra 04-08 July 2011Document13 pagesNEW Weekly Indra 04-08 July 2011jo_jo_maniaNo ratings yet
- AnyelirDocument2 pagesAnyelirjo_jo_maniaNo ratings yet
- Structure Content: 1. EXERCISE 1 (Skill 1-2) 2. Toefl Review Exercise (Skill 1-2) 3. Answer KeysDocument3 pagesStructure Content: 1. EXERCISE 1 (Skill 1-2) 2. Toefl Review Exercise (Skill 1-2) 3. Answer Keysjo_jo_mania0% (1)
- OrtoDocument61 pagesOrtojo_jo_maniaNo ratings yet
- International Centre For Eye Health Teaching Set 2 The Eye in Primary Health CareDocument25 pagesInternational Centre For Eye Health Teaching Set 2 The Eye in Primary Health Carejo_jo_maniaNo ratings yet
- Sunday, 26/09 /2010 PT/LN/MG:: Consultant DR Mas Putra SPMDocument6 pagesSunday, 26/09 /2010 PT/LN/MG:: Consultant DR Mas Putra SPMjo_jo_maniaNo ratings yet
- Migraine Prophylaxis: Pharmacotherapy PerspectivesDocument11 pagesMigraine Prophylaxis: Pharmacotherapy Perspectivesjo_jo_maniaNo ratings yet
- Arterial Blood Gas: DR - Made Widia, Sp.A (K)Document19 pagesArterial Blood Gas: DR - Made Widia, Sp.A (K)jo_jo_mania100% (1)
- UveaDocument43 pagesUveajo_jo_mania100% (1)
- Histamin Dan inDocument30 pagesHistamin Dan inNurul FadilaturrahmiNo ratings yet
- Dyslexia: Developmental Dyslexia Is ADocument5 pagesDyslexia: Developmental Dyslexia Is Ajo_jo_mania100% (1)
- X RaysDocument1 pageX Raysjo_jo_maniaNo ratings yet
- An Endometrial Is A Procedure To Remove A Small Sample of The Lining of The UterusDocument2 pagesAn Endometrial Is A Procedure To Remove A Small Sample of The Lining of The Uterusjo_jo_maniaNo ratings yet
- Strategic Managemment Perry Ring AMR Apr 1985Document12 pagesStrategic Managemment Perry Ring AMR Apr 1985Anderson De Oliveira ReisNo ratings yet
- Bawang Merah Bawang PutihDocument3 pagesBawang Merah Bawang Putihzulfarahma50% (2)
- Case Study 2Document3 pagesCase Study 2Shahaneh BalateroNo ratings yet
- The Nehru DynastyV1.1Document7 pagesThe Nehru DynastyV1.1das_ankita0111No ratings yet
- A Presentation Digital T.V-An Innovation by AirtelDocument19 pagesA Presentation Digital T.V-An Innovation by AirtelkdkripaNo ratings yet
- Shifting The Focus From Forms To Form in The EFL ClassroomDocument7 pagesShifting The Focus From Forms To Form in The EFL ClassroomNguyên KanNo ratings yet
- Japanese Greetings For EverydayDocument13 pagesJapanese Greetings For EverydayMarvin MayormenteNo ratings yet
- Sony Corporation-FinalDocument13 pagesSony Corporation-FinalLakshan WeerasekeraNo ratings yet
- The Pentatonic Scale Cheat Sheet The Pentatonic Way LockedDocument10 pagesThe Pentatonic Scale Cheat Sheet The Pentatonic Way LockedfreimannNo ratings yet
- Good Morning Text MessagesDocument7 pagesGood Morning Text MessagesStephan MilesNo ratings yet
- Curriculum Vitae - Eka Devi Wulandari (2019) PDFDocument3 pagesCurriculum Vitae - Eka Devi Wulandari (2019) PDFDipta VioniNo ratings yet
- 100 Best-Selling Cases: The Case For LearningDocument29 pages100 Best-Selling Cases: The Case For LearningSultan KhanNo ratings yet
- EMBA Applied Value Investing (Ajdler) SP2016Document3 pagesEMBA Applied Value Investing (Ajdler) SP2016darwin12No ratings yet
- Manual m2x3 Enm b11Document94 pagesManual m2x3 Enm b11pondokjituNo ratings yet
- MUMONKAN - All 48 Koans With CommentariesDocument22 pagesMUMONKAN - All 48 Koans With CommentariesAhmad AlhourNo ratings yet
- 2013 Psat NMSQT Student GuideDocument56 pages2013 Psat NMSQT Student Guideclementscounsel87250% (1)
- Hem Lab Manual DiffDocument9 pagesHem Lab Manual DiffFatima Mae LusanNo ratings yet
- Dissertation Carl Friedrich GaussDocument6 pagesDissertation Carl Friedrich GaussWriteMyPaperForMeIn3HoursUK100% (1)
- First Metro Investment Vs Este Del Sol Mountain Reserve Inc - 141811 - November 15, 2001 - JDocument9 pagesFirst Metro Investment Vs Este Del Sol Mountain Reserve Inc - 141811 - November 15, 2001 - JulticonNo ratings yet
- Review: I Agree Completely I Agree To Some Extent I Disagree CompletelyDocument1 pageReview: I Agree Completely I Agree To Some Extent I Disagree CompletelynaluzotanNo ratings yet
- Ind As 115 VS Ind As 18Document7 pagesInd As 115 VS Ind As 18Yogendrasinh RaoNo ratings yet
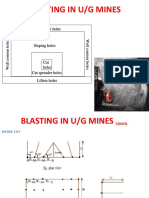
- Blasting in U/G Mines: Roof Contour Holes Roof Contour HolesDocument10 pagesBlasting in U/G Mines: Roof Contour Holes Roof Contour HolesSiddharth MukhillaNo ratings yet
- A Spatial Analysis of Crop-Land Suitability For Sustainable Agricultural Development in Aiyar Basin, Tamil NaduDocument12 pagesA Spatial Analysis of Crop-Land Suitability For Sustainable Agricultural Development in Aiyar Basin, Tamil NaduBala Subramani KNo ratings yet
- Uea Coursework Word CountDocument4 pagesUea Coursework Word Counttgpazszid100% (2)
- Self Worth SpeechDocument1 pageSelf Worth SpeechAbigail Fritz GoloNo ratings yet
- Computer Notes - Scan ConversionDocument7 pagesComputer Notes - Scan Conversionecomputernotes100% (1)
- The Information Apocalypse Rough Draft-1Document6 pagesThe Information Apocalypse Rough Draft-1api-425080738No ratings yet