Guideline for Treatment of Cancer Near the End of Life
What are we trying to do? We are trying to ensure the most effective care for patients with very advanced cancers who are on the Oregon Health Plan (OHP). We currently have a guideline which helps doctors and health plans decide when to offer treatment aimed at curing cancer to patients. The HERC has heard concerns from cancer doctors, patients, and health plans that the current guideline (Guideline Note 12) restricts care too much. The history of cancer care coverage by OHP: 1) Early versions of the Prioritized List did not allow payment for ANY care of cancer for patients who had less than a 5% 5 year expected survival due to their cancer. 2) The current Guideline Note 12 was adopted in 2009 to allow payment for more treatment of more cancers for more patients. It outlines restrictions in care for those patients who have a life expectancy of 24 months or less. What has been done so far to update Guideline Note 12? 1) The Value Based Benefits Subcommittee (VBBS) of the Health Evidence Review Commission (HERC) heard from various doctors, patients and health plans that the current guideline was not working. 2) The VBBS convened a workgroup that held 2 public meetings. The workgroup was made up of oncologists (doctors who care for cancer patients), a nurse who works with cancer patients, a doctor who provides palliative care, an attorney who specialized in healthcare law, and a health plan administrator. A patient member was not able to attend the meetings, but had the opportunity to participate in email discussions. The public meetings were very well attended, and testimony was heard from patient advocates, doctors, and others. Other stakeholders were able to provide input via discussions with HERC staff. What does the proposed new guideline say? 1) The new guideline allows payment for curative treatment for nearly all cancer patients. Those patients with very serious, metastatic cancer who have such severe health issues (such as kidney failure or heart failure) that curative chemotherapy would be too toxic for them should not get this type of treatment. Patients who have been given many types of current curative chemotherapy but continue to decline in health and have a very limited ability to care for themselves, should also not get more curative chemotherapy. 2) The new guideline REQUIRES patients and doctors to have a frank and open discussion about the patients goals of care and what can really be expected from various care options, including chemotherapy. This conversation needs to cover the harms and side effects of treatments, and allow the patient to make choices about what treatments he or she wants based on his or her values, in shared decision making with his or her doctor. This type of discussion has been shown in scientific studies to improve cancer patients
Guideline for Treatment of Cancer Near the End of Life
lives and allows these patients to spend more time with their families instead of in hospitals. 3) Cancer care is required to be provided following evidence-based pathways of care devised by leading national cancer expert groups. This ensures that Oregon cancer patients receive the type of care that has been shown to have the best results with the fewest side effects and other problems. What else does OHP do for cancer patients? 1) OHP provides all types of palliative care for cancer patients, to make sure that they live the most pain-free, highest quality life with their cancer. Patients have access to medicines for nausea and pain, acupuncture, home health care, wheelchairs, surgery to relieve a blockage in the gut, radiation to shrink painful tumors in bones, and all other types of palliative care. This palliative care will continue to be provided to all Oregon cancer patients. What happens now? 1) The VBBS will hear testimony from patients, doctors, pharmaceutical companies, and any other interested member of the public today. 2) The committee members will discuss the new guideline and the testimony they hear. They may choose to re-work some or all of the guideline, or they may adopt is as it is written. 3) If the guideline is adopted, it will be reviewed by the entire HERC, which has members from all types of areas in medicine (doctors, nurses, chiropractic, patients, health plan administrators, and more). The HERC may make changes or accept it as the VBBS has approved. 4) If approved, the guideline will start assisting patients, doctors, and health plans in the care of patients with advanced stage cancer beginning in October 2013.
Guideline for Treatment of Cancer Near the End of Life
Proposed New Guideline
GUIDELINE 12 CANCER CARE NEAR THE END OF LIFE Cancer is a complex group of diseases with treatments that vary depending on the specific subtype of cancer and the patients unique medical and social situation. Goals of appropriate cancer therapy can vary from intent to cure, disease burden reduction, disease stabilization and control of symptoms. Cancer care must always take place in the context of the patients support systems, overall heath, and core values. Patients should have access to appropriate peerreviewed clinical trials of cancer therapies. A comprehensive multidisciplinary approach to treatment should be offered including palliative care services (see Statement of Intent 1, Palliative Care). Treatment with intent to prolong survival is not a covered service for patients who have progressive metastatic cancer with 1) severe co-morbidities unrelated to the cancer that result in significant impairment in two or more major organ systems which would affect efficacy and/or toxicity of therapy; OR 2) a continued decline in spite of best available therapy with a non reversible Karnofsky Performance Status or Palliative Performance score of <50% with ECOG performance status of 3 or higher which are not due to a pre-existing disability. Treatment with intent to relieve symptoms or improve quality of life is a covered service as outlined in Statement of Intent 1, Palliative Care. To qualify for treatment coverage, the cancer patient must have a documented discussion about treatment goals, treatment prognosis and the side effects, and knowledge of the realistic expectations of treatment efficacy. This discussion may take place with the patients oncologist, primary care provider, or other health care provider, but preferably in a collaborative interdisciplinary care coordination discussion. Treatment must be provided via evidence-driven pathways (such as NCCN, ASCO, ASH, ASBMT, or NIH Guidelines) when available.
Guideline for Treatment of Cancer Near the End of Life
Current Guideline To Be Replaced
GUIDELINE NOTE 12, TREATMENT OF CANCER WITH LITTLE OR NO BENEFIT PROVIDED NEAR THE END OF LIFE Lines 102,103,123-125,144,159,165,166,170,181,197,198,207,208,218,220, 221,228,229,231, 243,249,252,275-278,280,287,292,310-312,320,339-341,356,459,586,622 This guideline only applies to patients with advanced cancer who have less than 24 months median survival with treatment. All patients receiving end of life care, either with the intent to prolong survival or with the intent to palliate symptoms, should have/be engaged with palliative care providers (for example, have a palliative care consult or be enrolled in a palliative care program). Treatment with intent to prolong survival is not a covered service for patients with any of the following: Median survival of less than 6 months with or without treatment, as supported by the best available published evidence Median survival with treatment of 6-12 months when the treatment is expected to improve median survival by less than 50%, as supported by the best available published evidence Median survival with treatment of more than 12 months when the treatment is expected to improve median survival by less than 30%, as supported by the best available published evidence Poor prognosis with treatment, due to limited physical reserve or the ability to withstand treatment regimen, as indicated by low performance status. Unpublished evidence may be taken into consideration in the case of rare cancers which are universally fatal within six months without treatment. The Health Evidence Review Commission is reluctant to place a strict $/QALY (quality adjusted life-year) or $/LYS (life-year saved) requirement on end-of-life treatments, as such measurements are only approximations and cannot take into account all of the merits of an individual case. However, cost must be taken into consideration when considering treatment options near the end of life. For example, in no instance can it be justified to spend $100,000 in public resources to increase an individuals expected survival by three months when hundreds of thousands of Oregonians are without any form of health insurance. Treatment with the goal to palliate is addressed in Statement of Intent 1, Palliative Care.
You might also like
- A Connection Between A Symbol and A SymptomDocument1 pageA Connection Between A Symbol and A SymptomBasil LipcanNo ratings yet
- Lesson 1Document8 pagesLesson 1Random RandomNo ratings yet
- Palliative Care Tools - Technical Brief 2017 PDFDocument145 pagesPalliative Care Tools - Technical Brief 2017 PDFMas AnggaNo ratings yet
- Choosing Wisely Master ListDocument92 pagesChoosing Wisely Master ListrobertojosesanNo ratings yet
- Foundation Doctor Roles & Responsibilities (Including Minimum Requirements For Clinical Supervision) v2Document8 pagesFoundation Doctor Roles & Responsibilities (Including Minimum Requirements For Clinical Supervision) v2danielNo ratings yet
- Obsessive-Compulsive Disorder (OCD) Symptoms - Mayo ClinicDocument9 pagesObsessive-Compulsive Disorder (OCD) Symptoms - Mayo ClinicNill SalunkeNo ratings yet
- Palliative Care For The Patient With Incurable Cancer or Advanced DiseaseDocument73 pagesPalliative Care For The Patient With Incurable Cancer or Advanced DiseaseArif HameedNo ratings yet
- Palliative Care Assignment.Document6 pagesPalliative Care Assignment.NATHANIEL YERINo ratings yet
- Palliative Care Needs Assessment GuidanceDocument13 pagesPalliative Care Needs Assessment GuidanceDedes SahpitraNo ratings yet
- Palliative Care - Ika Syamsul Huda MZDocument329 pagesPalliative Care - Ika Syamsul Huda MZPapah SajaNo ratings yet
- Kerala State Palliative Care Policy 2019Document24 pagesKerala State Palliative Care Policy 2019ASIF ALI MHNo ratings yet
- Self Study Report: 1 Cycle of AccreditationDocument120 pagesSelf Study Report: 1 Cycle of AccreditationSatya AsatyaNo ratings yet
- Palliative Medicine and Supportive CareDocument12 pagesPalliative Medicine and Supportive CareKaren CárcamoNo ratings yet
- Advance Care PlanningDocument7 pagesAdvance Care PlanningMalcolm Payne0% (1)
- Palliative CareDocument4 pagesPalliative CareJohn Rex Baltazar Jr.No ratings yet
- BDS (CS)Document207 pagesBDS (CS)Aman RajputNo ratings yet
- Palliative Care NotesDocument29 pagesPalliative Care NotesCnette S. Lumbo100% (1)
- EBM 2018 - Head and CancersDocument136 pagesEBM 2018 - Head and CancersChandramohan SettyNo ratings yet
- 1 5141165742682538289Document457 pages1 5141165742682538289Mariângela FigueiredoNo ratings yet
- Bodysnatchers to Livesavers: Three Centuries of Medicine in EdinburghFrom EverandBodysnatchers to Livesavers: Three Centuries of Medicine in EdinburghNo ratings yet
- OWL at Purdue University Printable Handouts Using American Psychological Association (APA) FormatDocument28 pagesOWL at Purdue University Printable Handouts Using American Psychological Association (APA) Formatrryan100% (3)
- Care at The Time of DeathDocument11 pagesCare at The Time of DeathmultiusosvariadosNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, KarnatakaDocument34 pagesRajiv Gandhi University of Health Sciences, Bangalore, KarnatakaYayu AlawiiahNo ratings yet
- Cure Palliative 1Document64 pagesCure Palliative 1Mr. LNo ratings yet
- Facing DeathDocument188 pagesFacing DeathFrancisco MartinezNo ratings yet
- Foot Conditions in HomelessDocument41 pagesFoot Conditions in HomelessLyanne Daisy Duarte-VangNo ratings yet
- NHS Lanarkshire Palliative Care GuidelinesDocument82 pagesNHS Lanarkshire Palliative Care GuidelinesAndi WiraNo ratings yet
- The Imprtance of End of Life Care in Nursing Home Settings Is Not Diminished by A DisasterDocument14 pagesThe Imprtance of End of Life Care in Nursing Home Settings Is Not Diminished by A DisasterIrfan FauziNo ratings yet
- Achieving Cultural Competency: A Case-Based Approach to Training Health ProfessionalsFrom EverandAchieving Cultural Competency: A Case-Based Approach to Training Health ProfessionalsNo ratings yet
- Hospice and End of Life Care PaperDocument6 pagesHospice and End of Life Care Paperapi-570837257No ratings yet
- Improving The Quality of Care in An Acute Care Facility Through RDocument88 pagesImproving The Quality of Care in An Acute Care Facility Through RNor-aine Salazar AccoyNo ratings yet
- Analisis Jurnal End of Life-Tedi&saidDocument5 pagesAnalisis Jurnal End of Life-Tedi&saidYulia JuniartiNo ratings yet
- Forced-To-Care Nanako Glenn PDFDocument269 pagesForced-To-Care Nanako Glenn PDFEli SaNo ratings yet
- Palliative Care 11918Document69 pagesPalliative Care 11918meldelsNo ratings yet
- Ethical Dilemmas in Nursing PDFDocument5 pagesEthical Dilemmas in Nursing PDFtitiNo ratings yet
- BDS Regulations HAND BOOK 2013-14 PDFDocument135 pagesBDS Regulations HAND BOOK 2013-14 PDFSayeeda MohammedNo ratings yet
- Research in Palliative Care PresentationDocument20 pagesResearch in Palliative Care PresentationNICKY SAMBONo ratings yet
- FinalintegrativereviewDocument17 pagesFinalintegrativereviewapi-346349076No ratings yet
- Introduction To Oncology and Palliative Care: Lecturer: Nadia ShamasnahDocument47 pagesIntroduction To Oncology and Palliative Care: Lecturer: Nadia ShamasnahXo Yem100% (1)
- End of Life Literature ReviewDocument4 pagesEnd of Life Literature Reviewnydohavihup2100% (1)
- Lessons You Can Learn From Fitness Classes: 'This Book Below Will Show You Exactly What You Need To Do To Finally Have All The Skills Required for Optimal Health!'From EverandLessons You Can Learn From Fitness Classes: 'This Book Below Will Show You Exactly What You Need To Do To Finally Have All The Skills Required for Optimal Health!'Rating: 5 out of 5 stars5/5 (1)
- Islam and Palliative CareDocument16 pagesIslam and Palliative CareShirakawa AlmiraNo ratings yet
- Action Plan For Oral Health Promotion 2013-2017Document32 pagesAction Plan For Oral Health Promotion 2013-2017bobNo ratings yet
- Successful Doctor Patient Communication PDFDocument6 pagesSuccessful Doctor Patient Communication PDFMak Alisson BorgesNo ratings yet
- ICU MED1 Survival Kits 2009 (Final)Document88 pagesICU MED1 Survival Kits 2009 (Final)Kevin WongNo ratings yet
- Mucositis GuidlinesDocument13 pagesMucositis GuidlinesEman MossanNo ratings yet
- Understanding The Health Care SystemDocument28 pagesUnderstanding The Health Care SystemSbitNo ratings yet
- End of Life Care DissertationDocument8 pagesEnd of Life Care DissertationCustomCollegePapersMadison100% (1)
- Medicine Palliative CareDocument5 pagesMedicine Palliative CareMarco Paulo Reyes NaoeNo ratings yet
- Palliative Care Policy Kerala 109 2008 HFWD Dated 15.4.08Document33 pagesPalliative Care Policy Kerala 109 2008 HFWD Dated 15.4.08jajaja hshsjsNo ratings yet
- WHO Generic Palliative Care (Dr. Rudi)Document26 pagesWHO Generic Palliative Care (Dr. Rudi)Inna RosdyasariNo ratings yet
- NAAC ManualDocument97 pagesNAAC ManualMalagouda PatilNo ratings yet
- Clinical Practice Guidelines For Quality Palliative Care (National Consensus Project)Document76 pagesClinical Practice Guidelines For Quality Palliative Care (National Consensus Project)NCP88% (8)
- Reflection About Palliative Care and End of Life CareDocument5 pagesReflection About Palliative Care and End of Life CareVILLEJO JHOVIALENNo ratings yet
- Lymphatic System (Anaphy)Document27 pagesLymphatic System (Anaphy)Ryan RanasNo ratings yet
- Strategies For Radiation Therapy Treatment PlanningDocument319 pagesStrategies For Radiation Therapy Treatment PlanningRodrigoNo ratings yet
- Letter To Judge Hernandez From Rural Oregon LawmakersDocument4 pagesLetter To Judge Hernandez From Rural Oregon LawmakersStatesman JournalNo ratings yet
- Roads and Trails of Cascade HeadDocument1 pageRoads and Trails of Cascade HeadStatesman JournalNo ratings yet
- Matthieu Lake Map and CampsitesDocument1 pageMatthieu Lake Map and CampsitesStatesman JournalNo ratings yet
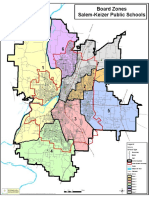
- School Board Zones Map 2021Document1 pageSchool Board Zones Map 2021Statesman JournalNo ratings yet
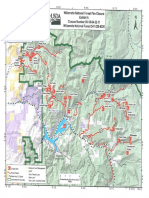
- Cedar Creek Vegitation Burn SeverityDocument1 pageCedar Creek Vegitation Burn SeverityStatesman JournalNo ratings yet
- Mount Hood National Forest Map of Closed and Open RoadsDocument1 pageMount Hood National Forest Map of Closed and Open RoadsStatesman JournalNo ratings yet
- Cedar Creek Fire Soil Burn SeverityDocument1 pageCedar Creek Fire Soil Burn SeverityStatesman JournalNo ratings yet
- Cedar Creek Fire Sept. 3Document1 pageCedar Creek Fire Sept. 3Statesman JournalNo ratings yet
- 2023 Drone Sample MapsDocument6 pages2023 Drone Sample MapsStatesman JournalNo ratings yet
- Complaint Summary Memo To Superintendent Re 8-9 BD Meeting - CB 9-14-22Document4 pagesComplaint Summary Memo To Superintendent Re 8-9 BD Meeting - CB 9-14-22Statesman JournalNo ratings yet
- Revised Closure of The Beachie/Lionshead FiresDocument4 pagesRevised Closure of The Beachie/Lionshead FiresStatesman JournalNo ratings yet
- Salem-Keizer Parent and Guardian Engagement in Education Month ProclamationDocument1 pageSalem-Keizer Parent and Guardian Engagement in Education Month ProclamationStatesman JournalNo ratings yet
- 2021 Ironman 70.3 Oregon Traffic ImpactDocument2 pages2021 Ironman 70.3 Oregon Traffic ImpactStatesman JournalNo ratings yet
- LGBTQ Proclaimation 2022Document1 pageLGBTQ Proclaimation 2022Statesman JournalNo ratings yet
- Proclamation Parent & Guardian Engagement in Education 1-11-22 Final, SignedDocument1 pageProclamation Parent & Guardian Engagement in Education 1-11-22 Final, SignedStatesman JournalNo ratings yet
- Resource List For Trauma Responses: Grounding Breathing Exercises To Take You Out of "Fight/Flight" ModeDocument3 pagesResource List For Trauma Responses: Grounding Breathing Exercises To Take You Out of "Fight/Flight" ModeStatesman JournalNo ratings yet
- Windigo Fire ClosureDocument1 pageWindigo Fire ClosureStatesman JournalNo ratings yet
- Oregon Annual Report Card 2020-21Document71 pagesOregon Annual Report Card 2020-21Statesman JournalNo ratings yet
- Salem-Keizer Discipline Data Dec. 2021Document13 pagesSalem-Keizer Discipline Data Dec. 2021Statesman JournalNo ratings yet
- Crib Midget Day Care Emergency Order of SuspensionDocument6 pagesCrib Midget Day Care Emergency Order of SuspensionStatesman JournalNo ratings yet
- School Board Zone MapDocument1 pageSchool Board Zone MapStatesman JournalNo ratings yet
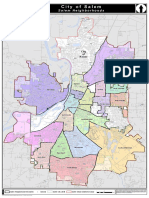
- All Neighborhoods 22X34Document1 pageAll Neighborhoods 22X34Statesman JournalNo ratings yet
- SIA Report 2022 - 21Document10 pagesSIA Report 2022 - 21Statesman JournalNo ratings yet
- Op Ed - Anthony MedinaDocument2 pagesOp Ed - Anthony MedinaStatesman JournalNo ratings yet
- Statement From Marion County Medical Examiner's Office On Heat-Related DeathsDocument1 pageStatement From Marion County Medical Examiner's Office On Heat-Related DeathsStatesman JournalNo ratings yet
- SB Agenda 20210415 EnglishDocument1 pageSB Agenda 20210415 EnglishStatesman JournalNo ratings yet
- City of Salem Photo Red Light Program 2021 Legislative ReportDocument8 pagesCity of Salem Photo Red Light Program 2021 Legislative ReportStatesman JournalNo ratings yet
- Gcab - Personal Electronic Devices and Social Media - StaffDocument2 pagesGcab - Personal Electronic Devices and Social Media - StaffStatesman JournalNo ratings yet
- Schools, Safe Learners (RSSL) Guidance. We Have Established A Statewide Rapid Testing ProgramDocument3 pagesSchools, Safe Learners (RSSL) Guidance. We Have Established A Statewide Rapid Testing ProgramStatesman Journal100% (1)
- 12 Most Annoying Bad Habits of TherapistsDocument7 pages12 Most Annoying Bad Habits of TherapistssalalepeNo ratings yet
- Peritonsillar Abscess DrainageDocument4 pagesPeritonsillar Abscess Drainagesyibz100% (1)
- 6 Contingency Planning Tips For SuccessDocument3 pages6 Contingency Planning Tips For SuccessBudi YunantoNo ratings yet
- "Hand-Off Communication" Sbar: Google Automatically Generates HTML Versions of Documents As We Crawl The WebDocument3 pages"Hand-Off Communication" Sbar: Google Automatically Generates HTML Versions of Documents As We Crawl The WebclarimerNo ratings yet
- PNLE 1 Part 4Document4 pagesPNLE 1 Part 4Ivan LouiseNo ratings yet
- Student Nursing Care Plan TemplateDocument3 pagesStudent Nursing Care Plan TemplateYuni NatasyaNo ratings yet
- Step 1 Guide-2Document16 pagesStep 1 Guide-2Eileen Jin100% (2)
- Lvp-Large Volume ParentralsDocument36 pagesLvp-Large Volume ParentralsRákêsh MãttàNo ratings yet
- Physiotherapy in DementiaDocument4 pagesPhysiotherapy in DementiaNabilla Yuharlina100% (1)
- Term PaperDocument27 pagesTerm PaperKimberly MilaranNo ratings yet
- FijiTimes - January 20 2017Document11 pagesFijiTimes - January 20 2017fijitimescanadaNo ratings yet
- Lewis: Medical-Surgical Nursing, 8 Edition: Chapter 36: Nursing Management: Dysrhythmias Key Points - PrintableDocument6 pagesLewis: Medical-Surgical Nursing, 8 Edition: Chapter 36: Nursing Management: Dysrhythmias Key Points - PrintableMonica100% (1)
- .Dolor Neonato TradDocument10 pages.Dolor Neonato TradAsdrubal MontañoNo ratings yet
- Diagnostic Criteria For 298Document1 pageDiagnostic Criteria For 298Pradeep KumarNo ratings yet
- Liceo de Cagayan University College of Nursing: ST ND RDDocument3 pagesLiceo de Cagayan University College of Nursing: ST ND RDPAUL MICHAEL G. BAGUHINNo ratings yet
- 1.prayudi FNL BDG Clinical Science DiagnoDocument34 pages1.prayudi FNL BDG Clinical Science DiagnoBoy Henri PasaribuNo ratings yet
- Chronic Suppurative Otitis Media PDFDocument3 pagesChronic Suppurative Otitis Media PDFsarahNo ratings yet
- What Is Peritoneal DialysisDocument34 pagesWhat Is Peritoneal DialysisKen MagallanesNo ratings yet
- Shivering in The Postoperative PatientDocument5 pagesShivering in The Postoperative PatientBrian SoesantoNo ratings yet
- Arero Hospital Multidisciplinary Ward RoundsDocument6 pagesArero Hospital Multidisciplinary Ward Roundssami ketema100% (1)
- ACP PocketbookDocument91 pagesACP PocketbookjamesbeaudoinNo ratings yet
- FINAL September 2010 Gazette (Reduced Size)Document16 pagesFINAL September 2010 Gazette (Reduced Size)cedivadenia8084No ratings yet
- Pathophysiology of Severe Mental RetardationDocument4 pagesPathophysiology of Severe Mental RetardationGiancarlo_Gala_4548100% (1)
- The Nursing Assistant and The Care TeamDocument13 pagesThe Nursing Assistant and The Care TeamShannie PadillaNo ratings yet
- A Colour Handbook of Oral Medicine - M. Lewis, R. Jordan (Manson, 2004) WW PDFDocument177 pagesA Colour Handbook of Oral Medicine - M. Lewis, R. Jordan (Manson, 2004) WW PDFAdrian Tirla100% (1)
- Transcript of Stuart Jones HearingDocument36 pagesTranscript of Stuart Jones HearingJacquie ONo ratings yet
- 1GDocument10 pages1GKunj Patel100% (1)
- Diagnostic Test 1Document4 pagesDiagnostic Test 1aryawiraNo ratings yet