Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 5.4 SCADA System Functional RequirementsDocument85 pages5.4 SCADA System Functional RequirementsYinwu ZhaoNo ratings yet
- Geothermal Energy Poster 2Document1 pageGeothermal Energy Poster 2api-298575301100% (2)
- Run-On and FregmentsDocument29 pagesRun-On and FregmentsMushtaq AhmadNo ratings yet
- Surrogacy Contract Sample 070215 PDFDocument26 pagesSurrogacy Contract Sample 070215 PDFBalbir DhimanNo ratings yet
- CACR21 January 2015Document19 pagesCACR21 January 2015maikaNo ratings yet
- 48 Weeks To Total M-Powerment!Document18 pages48 Weeks To Total M-Powerment!sundevil2010usa4605No ratings yet
- NYJC Prelim 2006 P2Document12 pagesNYJC Prelim 2006 P2miiewNo ratings yet
- F1.4 - Marine Sediment Treatment and ReuseDocument14 pagesF1.4 - Marine Sediment Treatment and ReuseKwan Chun SingNo ratings yet
- Experiment 13 Ultrafiltration UnitDocument13 pagesExperiment 13 Ultrafiltration UnitKishen NaniNo ratings yet
- Salvador Sanchez Complaint SignedDocument2 pagesSalvador Sanchez Complaint SignedStephen LoiaconiNo ratings yet
- A Review On The Enhancement of Figure of MeritDocument23 pagesA Review On The Enhancement of Figure of Meritsasa_22No ratings yet
- 5 ElementosDocument3 pages5 ElementosHectorNo ratings yet
- Unit 5. PHCDocument24 pagesUnit 5. PHCFenembar MekonnenNo ratings yet
- Golis University: Faculty of Business and Economics Chapter Four (Part Two) Accounting Information SystemDocument32 pagesGolis University: Faculty of Business and Economics Chapter Four (Part Two) Accounting Information Systemsaed cabdiNo ratings yet
- RS 232 Repeater KFD2-FF-Ex2.RS232: FunctionDocument4 pagesRS 232 Repeater KFD2-FF-Ex2.RS232: FunctionEder AlexandreNo ratings yet
- Dermatology: Professional Certificate inDocument4 pagesDermatology: Professional Certificate inmadimadi11No ratings yet
- Winsem2014-15 Cp0670 17-Apr-2015 Rm01 U4 l4 Rainwater-HarvestingDocument12 pagesWinsem2014-15 Cp0670 17-Apr-2015 Rm01 U4 l4 Rainwater-HarvestingShiv ShivNo ratings yet
- Unfuck Your Anilingus - How To Keep Your Oral Butt Sex Classy - Faith G Harper - 2022 - Microcosm Publishing - 9781648411618 - Anna's ArchiveDocument28 pagesUnfuck Your Anilingus - How To Keep Your Oral Butt Sex Classy - Faith G Harper - 2022 - Microcosm Publishing - 9781648411618 - Anna's Archiverhy4kjgqx6No ratings yet
- Petroleum Refining Notes 1Document5 pagesPetroleum Refining Notes 1api-304149645No ratings yet
- Oxidation of N-Acetyl Alanine by Chloramine-T in Presence of Hydrochloric Acid: A Kinetic and Mechanistic StudyDocument10 pagesOxidation of N-Acetyl Alanine by Chloramine-T in Presence of Hydrochloric Acid: A Kinetic and Mechanistic StudyCentral Asian StudiesNo ratings yet
- Significant Risk RegisterDocument8 pagesSignificant Risk RegisterswestyNo ratings yet
- Upda-Multiple Choice QuestionsDocument39 pagesUpda-Multiple Choice QuestionsAnonymous GllSJsUNo ratings yet
- CP SYSTEM - DESIGN DOCUMENT (Rev.01)Document46 pagesCP SYSTEM - DESIGN DOCUMENT (Rev.01)suman ghosh100% (1)
- Manual Usuario Smart LGDocument36 pagesManual Usuario Smart LGkarl CgcNo ratings yet
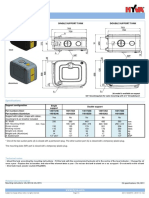
- Hyva Oil Tank: Single Support Tank Double Support TankDocument4 pagesHyva Oil Tank: Single Support Tank Double Support TankPutera Bumi NusantaraNo ratings yet
- Alexandra Marchuk V Faruqi and Faruqi AnswerDocument52 pagesAlexandra Marchuk V Faruqi and Faruqi Answerdavid_latNo ratings yet
- Snowball SamplingDocument3 pagesSnowball SamplingHamza ChNo ratings yet
- AaaaaaaaaaaaaaDocument6 pagesAaaaaaaaaaaaaaCarlos CBNo ratings yet
- UD150L-40E Ope M501-E053GDocument164 pagesUD150L-40E Ope M501-E053GMahmoud Mady100% (3)
- Biology Paper Ib: Maple Leaf International SchoolDocument22 pagesBiology Paper Ib: Maple Leaf International SchoolFcgfht ghkhkujk100% (1)