Download as pdf or txt
You might also like
- 1 The Basics 1Document19 pages1 The Basics 11202blackNo ratings yet
- Insulin Drug StudyDocument2 pagesInsulin Drug StudyRai Hanah92% (13)
- Pharmacology Review NotesDocument24 pagesPharmacology Review NotescampbellqueenNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (3)
- Practical Insulin: A Handbook for Prescribing ProvidersFrom EverandPractical Insulin: A Handbook for Prescribing ProvidersRating: 5 out of 5 stars5/5 (2)
- 60-2005 - Pregestational Diabetes MellitusDocument11 pages60-2005 - Pregestational Diabetes MellitusGrupo Atlas100% (1)
- CHAPTER 7 - Inpatient Management of Diabetes and HyperglycemiaDocument6 pagesCHAPTER 7 - Inpatient Management of Diabetes and HyperglycemiaenesNo ratings yet
- Diabetic EssayDocument6 pagesDiabetic Essayreet kaurNo ratings yet
- Effective Use of Insulin Therapy in Type 2 DiabetesDocument7 pagesEffective Use of Insulin Therapy in Type 2 DiabetesmariohuangNo ratings yet
- F. DEABETES MELLITUS Written ReportDocument6 pagesF. DEABETES MELLITUS Written ReportAsuncion CabacangNo ratings yet
- Gestational Diabetes MellitusDocument47 pagesGestational Diabetes MellitusHasan A AsFourNo ratings yet
- Insulin Secretion and FunctionDocument8 pagesInsulin Secretion and FunctionWendy EscalanteNo ratings yet
- Pharmacology Reading Materials On DMDocument19 pagesPharmacology Reading Materials On DMJames SoeNo ratings yet
- Insulin and Antidiabetic Drugs: Prof - DR Asya RehmanDocument23 pagesInsulin and Antidiabetic Drugs: Prof - DR Asya RehmanGareth BaleNo ratings yet
- DR - Rihab Pediatrics 02.pediatric DM Part TwoDocument7 pagesDR - Rihab Pediatrics 02.pediatric DM Part TwoMujtaba JawadNo ratings yet
- Pharmacology ResearchDocument20 pagesPharmacology ResearchaagalhazmiNo ratings yet
- Lesson 15: Drugs For Diabetes: Introduction (ILO-1 - 2)Document38 pagesLesson 15: Drugs For Diabetes: Introduction (ILO-1 - 2)Ralp ManglicmotNo ratings yet
- Gestational DiabetesDocument51 pagesGestational Diabeteskhadzx100% (2)
- All Types of InsulinDocument18 pagesAll Types of Insulinali mohammedNo ratings yet
- Disease Spotlight: Diabetes Mellitus: Insulin Insulin Is A Drug That Is Used To ControlDocument7 pagesDisease Spotlight: Diabetes Mellitus: Insulin Insulin Is A Drug That Is Used To ControlMIR SARTAJNo ratings yet
- Pharmacology Chapter 38Document7 pagesPharmacology Chapter 38languha NgatiNo ratings yet
- Postpartal Diabetes MellitusDocument7 pagesPostpartal Diabetes MellitusLei OrtegaNo ratings yet
- Insulin AdministrationDocument8 pagesInsulin AdministrationskybluealiNo ratings yet
- Postpartal Diabetes MellitusDocument7 pagesPostpartal Diabetes Mellitusnursereview100% (3)
- Common Endocrine Disorders: Iril I. Panes, RN, MANDocument63 pagesCommon Endocrine Disorders: Iril I. Panes, RN, MANJona Phie Domingo MonteroNo ratings yet
- MS3 Review NotesDocument11 pagesMS3 Review NotesPaul Anthony LoricaNo ratings yet
- Drugs For Diabetes (Part 1)Document6 pagesDrugs For Diabetes (Part 1)حوراء عارف الموسويNo ratings yet
- Presented by DR Ashish Sharma Guided by DR Meena PatelDocument74 pagesPresented by DR Ashish Sharma Guided by DR Meena PatelAndrew Surya Putra SccNo ratings yet
- Effective Use of Insulin: PreviewDocument6 pagesEffective Use of Insulin: Previewprad1973No ratings yet
- Neonatal HypoglycemiaDocument5 pagesNeonatal Hypoglycemiadiana rossNo ratings yet
- Maternal DM in LabourDocument8 pagesMaternal DM in LabourYwagar YwagarNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Diabetes Mellitus Key PointsDocument6 pagesLewis: Medical-Surgical Nursing, 10 Edition: Diabetes Mellitus Key PointsDeo FactuarNo ratings yet
- EInsulin RegiemDocument18 pagesEInsulin RegiemzahrabokerNo ratings yet
- Diabetes MellitusDocument16 pagesDiabetes MellitusApril Joy V. QuinoNo ratings yet
- Practice Tips: Insulin Protocols For Hospital Management of DiabetesDocument2 pagesPractice Tips: Insulin Protocols For Hospital Management of DiabetesEen AmaliaNo ratings yet
- DM Presentation NewDocument44 pagesDM Presentation NewKipz JonsNo ratings yet
- Diabetes in PregnencyDocument51 pagesDiabetes in PregnencyMuneeb JanNo ratings yet
- Management of Diabetes in Pregnancy: Naveen Kumar MDocument12 pagesManagement of Diabetes in Pregnancy: Naveen Kumar MNaveenKumarNo ratings yet
- Childhood Diabetes 2016Document64 pagesChildhood Diabetes 2016Awatef AbushhiwaNo ratings yet
- Module 9 ElaborateDocument6 pagesModule 9 ElaborateTrishaNo ratings yet
- Insulin NewDocument41 pagesInsulin NewSheikNo ratings yet
- Diabetes Mellitus Prepregnancy GestationalDocument11 pagesDiabetes Mellitus Prepregnancy GestationalLei OrtegaNo ratings yet
- Pharmacological Management of Type 1 DiabetesDocument6 pagesPharmacological Management of Type 1 DiabetesMI RFNo ratings yet
- Diabetes Mellitus Prepregnancy GestationalDocument11 pagesDiabetes Mellitus Prepregnancy Gestationalnursereview100% (9)
- Insulin TherapyDocument10 pagesInsulin Therapymandloianand51No ratings yet
- Antidiabetic AgentDocument5 pagesAntidiabetic AgentChamique Gelle Kerlin C LingayoNo ratings yet
- 8.0 Acute Complications of Diabetes: 8.1 RecommendationsDocument5 pages8.0 Acute Complications of Diabetes: 8.1 RecommendationsAdriana Roa BallesterosNo ratings yet
- Analogos de Insulina en DM 1 2017Document15 pagesAnalogos de Insulina en DM 1 2017LaurenArperNo ratings yet
- Module 2 Unit 2 - Pharmacotherapeutics For Endocrine Disorders - Student (Autosaved)Document77 pagesModule 2 Unit 2 - Pharmacotherapeutics For Endocrine Disorders - Student (Autosaved)Filipa EguavoenNo ratings yet
- Recent Advances in Therapy of DiabetesDocument62 pagesRecent Advances in Therapy of DiabetesMohd KhatibNo ratings yet
- Dietetik TerjemahDocument8 pagesDietetik TerjemahAsrori MuhofiNo ratings yet
- Update On Childhood Diabetes MellitusDocument51 pagesUpdate On Childhood Diabetes MellitusJulie Carnetion DNo ratings yet
- How Should We Manage Insulin Therapy Before SurgeryDocument3 pagesHow Should We Manage Insulin Therapy Before Surgerytsiko111No ratings yet
- Anti-Diabetic Drugs InsulinDocument26 pagesAnti-Diabetic Drugs Insulinwissam salimNo ratings yet
- NR 325 Diabetes Power-Student Copy1118Document39 pagesNR 325 Diabetes Power-Student Copy1118John MixerNo ratings yet
- FO-Antidiabetic-27042020-Blok 7Document64 pagesFO-Antidiabetic-27042020-Blok 7Indah NurhalizaNo ratings yet
- DM 22 Part 2 FFFFFDocument10 pagesDM 22 Part 2 FFFFFalhussaintariqNo ratings yet
- Diabetes Mellitus Prepared By: LORI R. LARA, R.NDocument14 pagesDiabetes Mellitus Prepared By: LORI R. LARA, R.NNovie Carla0% (1)
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 18: PsychiatryFrom EverandComplementary and Alternative Medical Lab Testing Part 18: PsychiatryRating: 5 out of 5 stars5/5 (1)
- Insulin Handbook: Understanding the Role and Effects of Insulin in Your BodyFrom EverandInsulin Handbook: Understanding the Role and Effects of Insulin in Your BodyNo ratings yet
- Group 3 CW - Role of NGOs in Socio EconomicDocument9 pagesGroup 3 CW - Role of NGOs in Socio EconomicKisyenene JamusiNo ratings yet
- Toxicon: Tamara Sajevic, Adrijana Leonardi, Igor Kri ZajDocument19 pagesToxicon: Tamara Sajevic, Adrijana Leonardi, Igor Kri Zajaulia rahmahNo ratings yet
- Endurance Test Sit UpDocument2 pagesEndurance Test Sit UpDinyoga Bima WaskitoNo ratings yet
- Sma Negeri 1 Kotabaru: I. Answer The Following Question!Document6 pagesSma Negeri 1 Kotabaru: I. Answer The Following Question!Dian MardhikaNo ratings yet
- Periodontal Ligament-SummerDocument24 pagesPeriodontal Ligament-Summerapi-3775747100% (1)
- Allison Taylor Dissertation Heinrich SchliemannDocument6 pagesAllison Taylor Dissertation Heinrich SchliemannPaperWritingServiceSuperiorpapersSpringfield100% (1)
- MonotropismQuestionnaire 230510Document5 pagesMonotropismQuestionnaire 230510Javiera AlarconNo ratings yet
- Multiple Choice QuestionsDocument6 pagesMultiple Choice QuestionsJamie DayagbilNo ratings yet
- Chapter-3 Motion in Two Dimention ErrorlessDocument58 pagesChapter-3 Motion in Two Dimention Errorlessaditya sureshNo ratings yet
- Ritishree Offer EztruckDocument4 pagesRitishree Offer EztruckKali RathNo ratings yet
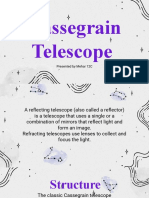
- Cassegrain Telescope: Presented by Mehar 12CDocument10 pagesCassegrain Telescope: Presented by Mehar 12CMehar FathimaNo ratings yet
- Claims and Counter ClaimsDocument13 pagesClaims and Counter ClaimsRk VaitlaNo ratings yet
- ABG Lecture DR Lenora FernandezDocument60 pagesABG Lecture DR Lenora Fernandezapi-19431894No ratings yet
- T5 B68 Craig Unger FDR - 5-21-04 Stull Email - Unger Saudi Flight Docs 616Document6 pagesT5 B68 Craig Unger FDR - 5-21-04 Stull Email - Unger Saudi Flight Docs 6169/11 Document ArchiveNo ratings yet
- Material ManagementDocument48 pagesMaterial Managementwintoday0150% (2)
- Paint Data Sheet - National Synthetic Enamel Gloss IDocument3 pagesPaint Data Sheet - National Synthetic Enamel Gloss Iaakh0% (1)
- City Planning and Neighbourhood Design Case Studies1Document132 pagesCity Planning and Neighbourhood Design Case Studies1shinmiNo ratings yet
- FORM V Abstract Under The Payment of Wages Act, 1936 (English Version)Document2 pagesFORM V Abstract Under The Payment of Wages Act, 1936 (English Version)anant nagvekarsNo ratings yet
- The 2021 EY Scholarship: The Bahamas, Bermuda, British Virgin Islands and The Cayman IslandsDocument3 pagesThe 2021 EY Scholarship: The Bahamas, Bermuda, British Virgin Islands and The Cayman IslandsKingshuk MukherjeeNo ratings yet
- Group 3Document59 pagesGroup 3Grey Sinclair100% (1)
- Unit 3 - Promotion - 27 Aug - ShareDocument38 pagesUnit 3 - Promotion - 27 Aug - SharebansaltulikaNo ratings yet
- DumbDocument10 pagesDumbJura LauraNo ratings yet
- Noninvasive Brain-Computer Interfaces: Gerwin Schalk, Brendan Z. AllisonDocument21 pagesNoninvasive Brain-Computer Interfaces: Gerwin Schalk, Brendan Z. AllisonQuốc ViệtNo ratings yet
- Marketing Management Project: Submitted byDocument41 pagesMarketing Management Project: Submitted byrpotnisNo ratings yet
- MUXDocument5 pagesMUXAmit SahaNo ratings yet
- Data SheetDocument48 pagesData SheetLost HumeraNo ratings yet
- Object Oriented Programming Using C++ Viva Questions Coders LodgeDocument7 pagesObject Oriented Programming Using C++ Viva Questions Coders LodgeGulchetan SinghNo ratings yet
- 5) BL Corrector y Manifiesto de CargaDocument3 pages5) BL Corrector y Manifiesto de CargaKevin Yair FerrerNo ratings yet
- Common Size Statement Analysis PDF Notes 1Document10 pagesCommon Size Statement Analysis PDF Notes 124.7upskill Lakshmi V0% (1)