Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- NS1 23Document119 pagesNS1 23Agnes Jeane Enriquez100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Contingency Plan On Limited f2fDocument36 pagesContingency Plan On Limited f2fJoannie AmparoNo ratings yet
- Terminolohiyang Pampandemya Na Nasa Wikang Ingles at Implikasyon Nito Sa Pag UnawaDocument13 pagesTerminolohiyang Pampandemya Na Nasa Wikang Ingles at Implikasyon Nito Sa Pag UnawaTan KarlNo ratings yet
- Revised Advisory For RGUHS Affiliated InstitutionsDocument54 pagesRevised Advisory For RGUHS Affiliated InstitutionshxjzoqaimeqlzgkfgoNo ratings yet
- A BDRRM Plan Template - English (1) - 220707 - 110132Document44 pagesA BDRRM Plan Template - English (1) - 220707 - 110132Jobert AlegreNo ratings yet
- SOP - Reopening of SchoolDocument7 pagesSOP - Reopening of SchoolAnoop SreedharNo ratings yet
- Reinforcing India'S Fight Against Covid-19: Conventional & New Career Opportunities in Hospital AdministrationDocument72 pagesReinforcing India'S Fight Against Covid-19: Conventional & New Career Opportunities in Hospital AdministrationMohaideen SubaireNo ratings yet
- DEPED DOH JMC No. 01 S. 2021Document27 pagesDEPED DOH JMC No. 01 S. 2021Jaymar MagtibayNo ratings yet
- 5) Sequence of Donning and Doffing of PPE For COVID-19 MOH. Update Version (2) 17.11.2020Document27 pages5) Sequence of Donning and Doffing of PPE For COVID-19 MOH. Update Version (2) 17.11.2020Amalina RazinNo ratings yet
- Covid-19: Negative Pressure Rooms: Anmf Evidence BriefDocument5 pagesCovid-19: Negative Pressure Rooms: Anmf Evidence BriefninesuNo ratings yet
- The Challenges and Lived Experiences of The Barangay Tanods A Phenomenological Qualitative Study in The Philippines During COVID 19 PandemicDocument20 pagesThe Challenges and Lived Experiences of The Barangay Tanods A Phenomenological Qualitative Study in The Philippines During COVID 19 PandemicKristine RilleraNo ratings yet
- COVID-19 - Prevention and Control Measures in CommunityDocument8 pagesCOVID-19 - Prevention and Control Measures in Communitykadoxe1682No ratings yet
- Covid Test Consent Form GoodgDocument3 pagesCovid Test Consent Form GoodgRocky LNo ratings yet
- Ncezid FRM Pass Attest Eng 508Document5 pagesNcezid FRM Pass Attest Eng 508GO STUDY ABROAD OFFICIALNo ratings yet
- Scope and LimitationsDocument4 pagesScope and LimitationsRey Dela PeñaNo ratings yet
- Donning DoffingDocument19 pagesDonning DoffingKristine AnaenNo ratings yet
- Work Method Statement FOR HVAC DuctingCopper PipesDocument9 pagesWork Method Statement FOR HVAC DuctingCopper PipesSameer JogasNo ratings yet
- نسخة اختبارDocument318 pagesنسخة اختبارSami AlanziNo ratings yet
- Journal Format Mental Health Well Being and Coping Strategies of ECE During COVID 19 PandemicDocument13 pagesJournal Format Mental Health Well Being and Coping Strategies of ECE During COVID 19 PandemicJan Carl OrtilanoNo ratings yet
- Chapter 2Document11 pagesChapter 2Niño Dwayne TuboNo ratings yet
- FINISHED Procedures For Mocha and Maisy Amended 15.06.21Document25 pagesFINISHED Procedures For Mocha and Maisy Amended 15.06.21Nathan RiggNo ratings yet
- Review On Smart Sanitizing Robot With Medicine Transport System For Covid-19Document6 pagesReview On Smart Sanitizing Robot With Medicine Transport System For Covid-19IJRASETPublicationsNo ratings yet
- Philippine Society of Nephrology, IncDocument6 pagesPhilippine Society of Nephrology, IncTricia LlorinNo ratings yet
- Universal PrecautionDocument46 pagesUniversal PrecautionJayrelle D. SafranNo ratings yet
- FOS - Package InsertDocument9 pagesFOS - Package InsertAnaNo ratings yet
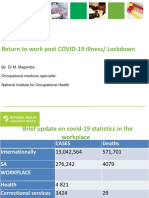
- Return To Work Post COVID-19 Illness/ LockdownDocument20 pagesReturn To Work Post COVID-19 Illness/ LockdownHuynh Luong Huy ThongNo ratings yet
- TLE 9 Organic Agri Q1 M5Document21 pagesTLE 9 Organic Agri Q1 M5Netchie BajeNo ratings yet
- The Bubonic Plague, Spanish Flu and Covid 19Document16 pagesThe Bubonic Plague, Spanish Flu and Covid 19maia harnauthNo ratings yet
- 000-Vasile-Burlui-1 CovidDocument2 pages000-Vasile-Burlui-1 CovidMihaela TuculinaNo ratings yet
- Facility-Based Surveillance Activities For COVID-19 Infection and Outcomes AmongDocument7 pagesFacility-Based Surveillance Activities For COVID-19 Infection and Outcomes AmongDr. CiciNo ratings yet