Download as pdf or txt
You might also like
- Sample California Complaint To Stop Foreclosure Sale by TrusteeDocument3 pagesSample California Complaint To Stop Foreclosure Sale by TrusteeStan Burman100% (5)
- Masterplan TemplateDocument72 pagesMasterplan TemplateMostafa FawzyNo ratings yet
- Spss 1Document2 pagesSpss 1DebiNo ratings yet
- Case Study On Metro RailDocument8 pagesCase Study On Metro RailSidhant0% (1)
- Tvet in BruneiDocument17 pagesTvet in Bruneiarchim_azymaNo ratings yet
- Pulse PolioDocument99 pagesPulse PolioChulbul Pandey100% (1)
- Faqs 1Document3 pagesFaqs 1api-317489352No ratings yet
- Ocial Arketing: Pulse Polio CampaignDocument20 pagesOcial Arketing: Pulse Polio CampaignArun PandeyNo ratings yet
- ASSESSMENT ON ROLE OF NON-GOVERNMENTAL ORGANIZATION (NGOs) ON THE ERADICATION OF POLIODocument23 pagesASSESSMENT ON ROLE OF NON-GOVERNMENTAL ORGANIZATION (NGOs) ON THE ERADICATION OF POLIOCapitallink cafeNo ratings yet
- Polio Fact or BluffDocument3 pagesPolio Fact or BluffZaira Marie Estrella MendezNo ratings yet
- 14.7pulse Polio ProgrammeDocument5 pages14.7pulse Polio Programmevenkat krishnan100% (1)
- International Perspective On Infectious Diseases: Rahul Gupta, MD, MPH, MBA, FACPDocument41 pagesInternational Perspective On Infectious Diseases: Rahul Gupta, MD, MPH, MBA, FACPNational Press FoundationNo ratings yet
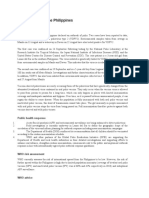
- DSPC 2019 (Article) Polio Outbreak - The PhilippinesDocument5 pagesDSPC 2019 (Article) Polio Outbreak - The PhilippinesDenisse Leonoras-PatersonNo ratings yet
- High Risk of Potent Drug ResistanceDocument2 pagesHigh Risk of Potent Drug ResistanceJxypee Tupas RolloNo ratings yet
- POLIOMYELITISDocument11 pagesPOLIOMYELITISSolomon Fallah Foa SandyNo ratings yet
- Polio Doc 1Document4 pagesPolio Doc 1yogeshdhuri22No ratings yet
- Pulse Polio: From Wikipedia, The Free EncyclopediaDocument3 pagesPulse Polio: From Wikipedia, The Free Encyclopediagunjan2808No ratings yet
- Doh, Who, Unicef To Conduct Nationwide Measles Campaign Starting October 26Document1 pageDoh, Who, Unicef To Conduct Nationwide Measles Campaign Starting October 26Dansoy BitantosNo ratings yet
- Doh, Who, Unicef To Conduct Nationwide Measles Campaign Starting October 26Document1 pageDoh, Who, Unicef To Conduct Nationwide Measles Campaign Starting October 26Dansoy BitantosNo ratings yet
- India Polio Press Release Feb 12Document2 pagesIndia Polio Press Release Feb 12InterActionNo ratings yet
- Public Health Current Affairs 2012 13 Diseases Drugs and Research Part 2 of 3Document17 pagesPublic Health Current Affairs 2012 13 Diseases Drugs and Research Part 2 of 3123F38262No ratings yet
- Polio CampaignDocument10 pagesPolio CampaignSritika PalNo ratings yet
- Vaccines and Global Health: The Week in Review 15 February 2014 Center For Vaccine Ethics & PolicyDocument37 pagesVaccines and Global Health: The Week in Review 15 February 2014 Center For Vaccine Ethics & PolicydavidrcurryNo ratings yet
- Vaccines - The Week in Review - 8 December 2012Document28 pagesVaccines - The Week in Review - 8 December 2012davidrcurryNo ratings yet
- Answers To PolioDocument3 pagesAnswers To PolioYoyoyo 123123No ratings yet
- Puls Polio ImmunizationDocument3 pagesPuls Polio ImmunizationBenoy BoseNo ratings yet
- The Battle Against PolioDocument3 pagesThe Battle Against PolioNerry Endah NazcharyNo ratings yet
- Pulse Polio Immunization IndiaDocument31 pagesPulse Polio Immunization IndiaBhumika RathoreNo ratings yet
- Global and National Health SituationDocument3 pagesGlobal and National Health SituationKathleen LunaNo ratings yet
- Polio Vaccine Is Very Safe,' DOH Reminds Public Amid EpidemicDocument2 pagesPolio Vaccine Is Very Safe,' DOH Reminds Public Amid EpidemicElaizel AlamagNo ratings yet
- Lesson 6 Children's Rights Case Study Hand OutDocument1 pageLesson 6 Children's Rights Case Study Hand OutLauren CavenderNo ratings yet
- Pulse PolioDocument6 pagesPulse Poliopriyankakgp100% (1)
- Rotaviruses Diarrhea: What Are The Benefits of The Rotavirus Vaccine?Document5 pagesRotaviruses Diarrhea: What Are The Benefits of The Rotavirus Vaccine?Mikko ArriesgoddessNo ratings yet
- Health PoliciesDocument5 pagesHealth PoliciesWarren LadrillonoNo ratings yet
- What Is Polio?Document3 pagesWhat Is Polio?Yanna BaptistaNo ratings yet
- National Rabies Prevention and Control Program: Printer-Friendly PDFDocument3 pagesNational Rabies Prevention and Control Program: Printer-Friendly PDFdaryl ann dep-asNo ratings yet
- Paper 1Document25 pagesPaper 1DrAqeel AshrafNo ratings yet
- THW Make Vaccination CompulsoryDocument2 pagesTHW Make Vaccination CompulsoryBenny Chandra PortnoyNo ratings yet
- Pulse PoDocument6 pagesPulse PoJoel Eljo Enciso SaraviaNo ratings yet
- Polio Eradication in Pakistan: Call For Alliance: EditorialDocument2 pagesPolio Eradication in Pakistan: Call For Alliance: EditorialRohmiatul handayaniNo ratings yet
- Topic: DiphtheriaDocument4 pagesTopic: DiphtheriaandreaNo ratings yet
- Artikel PolioDocument7 pagesArtikel PolioQonitah KhaldaNo ratings yet
- Health-WPS OfficeDocument178 pagesHealth-WPS OfficeFayyaz Ahmad AnjumNo ratings yet
- 1 in 10 Infants Worldwide Did Not Receive Any Vaccinations in 2016Document2 pages1 in 10 Infants Worldwide Did Not Receive Any Vaccinations in 2016YennyIrdayaniNasutionNo ratings yet
- Nature PoliomyelitisDocument6 pagesNature PoliomyelitisBolohan BiatriceNo ratings yet
- Rotary Polio Fact Sheet 2021 enDocument2 pagesRotary Polio Fact Sheet 2021 enLucas CavalcanteNo ratings yet
- Polio Phase in Tamil Nadu 2016Document6 pagesPolio Phase in Tamil Nadu 2016Chenthil KumarNo ratings yet
- Covid 19Document4 pagesCovid 19Jayve BasconNo ratings yet
- Polio Facts and FiguresDocument6 pagesPolio Facts and FiguresAmaka Cecilia0% (1)
- Angelica M.docx LFD 3Document2 pagesAngelica M.docx LFD 3Angelica Malacay RevilNo ratings yet
- Polio PDFDocument10 pagesPolio PDFJohn Edward EscoteNo ratings yet
- DiseasesDocument9 pagesDiseasesVenkata Rama RajuNo ratings yet
- LT 6Document1 pageLT 6flw.khozemaNo ratings yet
- Zika Virus Thesis CHAP-1-2-3 8-26-16Document43 pagesZika Virus Thesis CHAP-1-2-3 8-26-16Richard RL100% (3)
- Polio - Eradication, Vaccination, & Access - Bill & Melinda Gates FoundationDocument10 pagesPolio - Eradication, Vaccination, & Access - Bill & Melinda Gates FoundationkelvinkinergyNo ratings yet
- Preventing Polio From Becoming A Reemerging Disease: Conference Panel SummariesDocument2 pagesPreventing Polio From Becoming A Reemerging Disease: Conference Panel SummariesVincentNo ratings yet
- Poliomyelitis Eradication Program in The Philippines: Aida M. SalongaDocument4 pagesPoliomyelitis Eradication Program in The Philippines: Aida M. SalongaEarl OngNo ratings yet
- Position Paper Who ChinaDocument2 pagesPosition Paper Who Chinaapi-307248240No ratings yet
- 795 1027 1 PBDocument10 pages795 1027 1 PBRatri Abdatush SholihahNo ratings yet
- Unicef ContributionsDocument2 pagesUnicef ContributionsalyshaNo ratings yet
- Doh ThrustDocument3 pagesDoh ThrustJei SonNo ratings yet
- Alliance Vision and Mission: A) A Brief History of The World Health OrganizationDocument28 pagesAlliance Vision and Mission: A) A Brief History of The World Health OrganizationPriyanshi MehtaNo ratings yet
- MDG FS 6 enDocument2 pagesMDG FS 6 enSoe Lin HtutNo ratings yet
- Theories in AnthropologyDocument90 pagesTheories in AnthropologyKumar Abhinandan50% (2)
- Key Terms in EthicsDocument177 pagesKey Terms in EthicsKumar AbhinandanNo ratings yet
- Preparing For Safe Travel To High Altitude: by Paul Anderson, M.D. Co-Investigator - ASAP StudyDocument5 pagesPreparing For Safe Travel To High Altitude: by Paul Anderson, M.D. Co-Investigator - ASAP StudyKumar AbhinandanNo ratings yet
- Key Terms in EthicsDocument177 pagesKey Terms in EthicsKumar AbhinandanNo ratings yet
- Election of Students UnionDocument12 pagesElection of Students UnionKumar AbhinandanNo ratings yet
- RaggingDocument209 pagesRaggingRajjoy AdhikaryNo ratings yet
- 15A01510 Fluid Mechanics & Hydraulic MachinesDocument2 pages15A01510 Fluid Mechanics & Hydraulic MachinesarunNo ratings yet
- Account Statement SBI PDFDocument12 pagesAccount Statement SBI PDFUMESH KUMAR YadavNo ratings yet
- Usability Testing Report (ENGLISH Only)Document7 pagesUsability Testing Report (ENGLISH Only)memorphNo ratings yet
- 2 Curriculum Guide Ela PDFDocument269 pages2 Curriculum Guide Ela PDFDele AwodeleNo ratings yet
- Bijections - Zuming Feng - IdeaMath 2008Document4 pagesBijections - Zuming Feng - IdeaMath 2008bruh pogNo ratings yet
- Engineering Economy ProblemsDocument19 pagesEngineering Economy ProblemsEmperor VallenNo ratings yet
- 2014 SIM Annual Report Print FriendlyDocument73 pages2014 SIM Annual Report Print Friendlyzaid chaudry1No ratings yet
- Book 1Document103 pagesBook 1rebeccags1998No ratings yet
- Register of J. L. McElhany Papers Collection 001Document35 pagesRegister of J. L. McElhany Papers Collection 001Ploaia TârzieNo ratings yet
- 723PLUS Digital Control - WoodwardDocument40 pages723PLUS Digital Control - WoodwardMichael TanNo ratings yet
- The Victim's Autopsy ReportDocument2 pagesThe Victim's Autopsy ReportShan KNo ratings yet
- Aonla Cultivation ProjectDocument6 pagesAonla Cultivation ProjectshrishivankarNo ratings yet
- TarzanDocument2 pagesTarzanmaris quilantangNo ratings yet
- Chapter 3 Example ProblemsDocument38 pagesChapter 3 Example ProblemsHana JeonNo ratings yet
- Biology Ecology Revision NotesDocument7 pagesBiology Ecology Revision NotesGeorge ArgyrouNo ratings yet
- Cambridge, 2nd Ed.-Petty Cash BookDocument3 pagesCambridge, 2nd Ed.-Petty Cash BookShannen LyeNo ratings yet
- Gas Supply Agreement 148393.1Document5 pagesGas Supply Agreement 148393.1waking_days100% (1)
- B Com English 2016Document12 pagesB Com English 2016PRIYANK PATEL67% (3)
- Ariston As 600 V DryerDocument40 pagesAriston As 600 V DryermmvdlpNo ratings yet
- Anejom Grammar SketchDocument62 pagesAnejom Grammar Sketchalexandreq100% (1)
- Quick Start GuideDocument21 pagesQuick Start GuiderameshNo ratings yet
- ILMPDocument2 pagesILMPTed Jayson B. GuadamorNo ratings yet
- Chapter 3: Operating-System StructuresDocument31 pagesChapter 3: Operating-System StructuresDiamond MindglanceNo ratings yet
- Go Out in The World - F - Vocal ScoreDocument3 pagesGo Out in The World - F - Vocal ScoreParikNo ratings yet
- Leon Battista Alberti - Sebastino Serlio - Giacomo Barozzi Da Vignola - Andrea Palladio - Philibert de L'ormeDocument32 pagesLeon Battista Alberti - Sebastino Serlio - Giacomo Barozzi Da Vignola - Andrea Palladio - Philibert de L'ormeYsabelle Marie FuentesNo ratings yet