
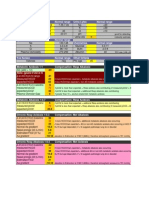
General Tox Approach
General Tox Approach
You might also like
- FRCPath Mock 2014 Model AnswersDocument29 pagesFRCPath Mock 2014 Model Answersmonday125No ratings yet
- Ganong - Physiology Self - Assessment Questions - 03Document46 pagesGanong - Physiology Self - Assessment Questions - 03Anonymous 4txA8N8et100% (3)
- Chemistry of CannabisDocument52 pagesChemistry of Cannabisciborg1978No ratings yet
- Chromatography LabDocument9 pagesChromatography Labjtrumpeter224100% (1)
- Poisoning: Overview of Pediatric Poisoning, Diagnosis and Treatment Summary of The Most Encountered PoisoningDocument46 pagesPoisoning: Overview of Pediatric Poisoning, Diagnosis and Treatment Summary of The Most Encountered PoisoningSergey DukkNo ratings yet
- Poisoning Stage V - 2020Document96 pagesPoisoning Stage V - 2020Sarper Hikmet TAZENo ratings yet
- Poisoning PDFDocument124 pagesPoisoning PDFDawn WRein Legaspi67% (3)
- Alcohol ToxicityDocument81 pagesAlcohol ToxicityKarim RezaNo ratings yet
- Toxic Alcohols - High Yields NEJMDocument21 pagesToxic Alcohols - High Yields NEJMDr. Shanojan Thiyagalingam, FRCPC FACPNo ratings yet
- Approach To Poisoned PatientDocument90 pagesApproach To Poisoned PatientGopi KrishnanNo ratings yet
- UMBC CC-EMTP Class Notes, FLCC Class 2010Document93 pagesUMBC CC-EMTP Class Notes, FLCC Class 2010Marc LaBarberaNo ratings yet
- Toxic AlcoholsDocument4 pagesToxic AlcoholsKaran SandhuNo ratings yet
- Dyah Trifianingsih, S. Kep. Ners. M. KepDocument76 pagesDyah Trifianingsih, S. Kep. Ners. M. KepSiprianus S SNo ratings yet
- Alcohol & Glycols: Group # 5 Aranas, Roxette Louraine Ardivilla, Gazel Myrrh Hugo, KevinDocument30 pagesAlcohol & Glycols: Group # 5 Aranas, Roxette Louraine Ardivilla, Gazel Myrrh Hugo, KevinRoxette Louraine R. AranasNo ratings yet
- AlcoholsDocument23 pagesAlcoholsdhaineyNo ratings yet
- Tox CasesDocument7 pagesTox CasesNeo Mervyn Monaheng100% (1)
- Drug Toxicology: Agung Nova Mahendra Department of Pharmacology & Therapy Faculty of Medicine, Udayana UniversityDocument27 pagesDrug Toxicology: Agung Nova Mahendra Department of Pharmacology & Therapy Faculty of Medicine, Udayana Universitywayan lentaraNo ratings yet
- 41 Clinical Cases in Biochemistry UKDocument2 pages41 Clinical Cases in Biochemistry UKAlexandra Ioana MoatarNo ratings yet
- Toxicology Lecture 10 (Chapter 7 Volatiles)Document22 pagesToxicology Lecture 10 (Chapter 7 Volatiles)MowlidAbdirahman Ali madaaleNo ratings yet
- Respiratory Acidosis Is Characterized by An Increase in The pCODocument3 pagesRespiratory Acidosis Is Characterized by An Increase in The pCOMwanja MosesNo ratings yet
- 5 2015 Farmako-ToxicologyDocument71 pages5 2015 Farmako-ToxicologyIkhzan PriolaksanaNo ratings yet
- Chemical Pathology Practical ExamDocument46 pagesChemical Pathology Practical ExamAbdulsamad AfolabiNo ratings yet
- Michael Chansky Acid Base Made Easy HandoutDocument18 pagesMichael Chansky Acid Base Made Easy HandoutTeguh RamadhanNo ratings yet
- Alcohols Ethanol, MethanolDocument55 pagesAlcohols Ethanol, MethanoljayNo ratings yet
- Acid Base Disorders Peter SehaDocument29 pagesAcid Base Disorders Peter SehaPeter SehaNo ratings yet
- Respiratory Assessment FindingsDocument197 pagesRespiratory Assessment Findingsannatw100% (2)
- Adi - IntoxicationDocument52 pagesAdi - IntoxicationAdi WidanaNo ratings yet
- Questions To Consider:: Ethylene Glycol Poisoning. Ethylene Glycol Chemically Occupies A Position Between EthylDocument4 pagesQuestions To Consider:: Ethylene Glycol Poisoning. Ethylene Glycol Chemically Occupies A Position Between EthylJeanette Miña GrajoNo ratings yet
- Anion Gap Metabolic Acidosis: More Then Just A Mud PileDocument21 pagesAnion Gap Metabolic Acidosis: More Then Just A Mud PileFarah SyazanaNo ratings yet
- Management of Poisoned PatientsDocument56 pagesManagement of Poisoned PatientsAmmarah TaimurNo ratings yet
- Acid Base PhysiologyDocument4 pagesAcid Base PhysiologyGhadeer EbraheemNo ratings yet
- ABG Algorithm PDFDocument2 pagesABG Algorithm PDFamin2014No ratings yet
- Module Iii Lab Manual (2024)Document20 pagesModule Iii Lab Manual (2024)ur.yared21No ratings yet
- Rat PoisonDocument41 pagesRat Poisonkhizra mumtazNo ratings yet
- Approach To Acid-Base Problems: DR Frank DalyDocument57 pagesApproach To Acid-Base Problems: DR Frank DalyscanutdNo ratings yet
- Fluid and ElectrolytesDocument14 pagesFluid and Electrolytesstring44100% (2)
- Moderator: Dr. R. K. Yadav (MD) Presented By: Ashish JaisawalDocument47 pagesModerator: Dr. R. K. Yadav (MD) Presented By: Ashish Jaisawalimranqazi11No ratings yet
- Final Exam Focus SheetDocument9 pagesFinal Exam Focus SheetDane WrightNo ratings yet
- Acid-Base Interpretation: APRIL 4, 2017Document9 pagesAcid-Base Interpretation: APRIL 4, 2017mohamedsmnNo ratings yet
- General Principles and Management of PoisonsDocument5 pagesGeneral Principles and Management of PoisonsOkpetah Chioma christabelNo ratings yet
- Drug OverdoseDocument94 pagesDrug Overdosemicheal1960No ratings yet
- Student Tox LectureDocument49 pagesStudent Tox Lecturelenin_villaltaNo ratings yet
- ABG MMHG InterpretationDocument92 pagesABG MMHG InterpretationManmeet SNo ratings yet
- Acid Base Disorders DR Kwaifa - PPTX 1Document99 pagesAcid Base Disorders DR Kwaifa - PPTX 1DICKSONNo ratings yet
- Ethylene Glycol Toxicosis in Animals - Toxicology - MSD Veterinary ManualDocument6 pagesEthylene Glycol Toxicosis in Animals - Toxicology - MSD Veterinary ManualMuhammad AgussalimNo ratings yet
- Synthesis Final ReviewDocument20 pagesSynthesis Final ReviewSamNo ratings yet
- Poisoning in ChildrenDocument11 pagesPoisoning in ChildrenAndriana HalfienNo ratings yet
- Body Fluids and ElectrolytesDocument42 pagesBody Fluids and ElectrolytesQusaiBadr100% (1)
- Tugas GinjalDocument22 pagesTugas GinjalAnastasia MargaretNo ratings yet
- Acid Base EquationsDocument21 pagesAcid Base EquationsBen JonesNo ratings yet
- Assignment: ToxicologyDocument8 pagesAssignment: ToxicologyAyesha LiaqatNo ratings yet
- Anion Gap Metabolic Acidemia Case BasedDocument4 pagesAnion Gap Metabolic Acidemia Case Basedspiros.a.markouNo ratings yet
- Case Report: An Unconscious Man With Profound Drug-Induced HypoglycaemiaDocument6 pagesCase Report: An Unconscious Man With Profound Drug-Induced Hypoglycaemiagevowo3277No ratings yet
- Acute Poisoning of Therapeutic Agents: by Alemayehu TomaDocument42 pagesAcute Poisoning of Therapeutic Agents: by Alemayehu TomaYohannis AsefaNo ratings yet
- Mnemonics: Do Not Adsorb To CharcoalDocument25 pagesMnemonics: Do Not Adsorb To CharcoalJiaYee GoNo ratings yet
- ABG Interpretation 1Document59 pagesABG Interpretation 1Sura KwakNo ratings yet
- Chapter Four: Chemical Analysis of UrineDocument174 pagesChapter Four: Chemical Analysis of UrineRebuma BeleteNo ratings yet
- AlcohoDocument32 pagesAlcohoVaibhav KaroliyaNo ratings yet
- Enzyme-summary (1)Document7 pagesEnzyme-summary (1)Aira Jane GamboaNo ratings yet
- ELECTROLYTES (Na & K)Document3 pagesELECTROLYTES (Na & K)Alondra SagarioNo ratings yet
- Alcohol Toxicity PDFDocument20 pagesAlcohol Toxicity PDFNabila Fatmayday UdiyahNo ratings yet
- The Impact Of Alcohol On The Brain - Based On The Teachings Of Dr. Andrew Huberman: Examining The Complex Interplay Between Alcohol And NeurobiologyFrom EverandThe Impact Of Alcohol On The Brain - Based On The Teachings Of Dr. Andrew Huberman: Examining The Complex Interplay Between Alcohol And NeurobiologyNo ratings yet
- Pass Paces EbDocument10 pagesPass Paces EbAnonymous 4txA8N8etNo ratings yet
- H IsselbacherDocument5 pagesH IsselbacherAnonymous 4txA8N8etNo ratings yet
- Topics Runtime: Subjects AnatomyDocument2 pagesTopics Runtime: Subjects AnatomyAnonymous 4txA8N8etNo ratings yet
- Hp165-02b-Nash (FF 050816v) ProtegidoDocument9 pagesHp165-02b-Nash (FF 050816v) ProtegidoAnonymous 4txA8N8etNo ratings yet
- Adpkd: Autosomal Dominant Polycystic Kidney DiseaseDocument7 pagesAdpkd: Autosomal Dominant Polycystic Kidney DiseaseAnonymous 4txA8N8etNo ratings yet
- Hanzi Pinyin English: HSK Level 2Document5 pagesHanzi Pinyin English: HSK Level 2Anonymous 4txA8N8etNo ratings yet
- Genetics 50qDocument62 pagesGenetics 50qAnonymous 4txA8N8etNo ratings yet
- Radiology Reviewed Meds Reviewed Pathology Reviewed Micro Reviewed "FASTHUG" CheckedDocument1 pageRadiology Reviewed Meds Reviewed Pathology Reviewed Micro Reviewed "FASTHUG" CheckedAnonymous 4txA8N8etNo ratings yet
- 6 Steps in Assisting in Cardiac Rhythm InterpretationDocument1 page6 Steps in Assisting in Cardiac Rhythm InterpretationAnonymous 4txA8N8etNo ratings yet
- EMQExample RacpDocument5 pagesEMQExample RacpAnonymous 4txA8N8etNo ratings yet
- Brunicardi-1996-Time Management - A RDocument7 pagesBrunicardi-1996-Time Management - A RAnonymous 4txA8N8etNo ratings yet
- Abdominal Exam DATEDocument3 pagesAbdominal Exam DATEAnonymous 4txA8N8etNo ratings yet
- Effective Feedback Skills: Sally Santen MD, PHDDocument9 pagesEffective Feedback Skills: Sally Santen MD, PHDAnonymous 4txA8N8etNo ratings yet
- Lymphoproliferative Disorders Part 2Document7 pagesLymphoproliferative Disorders Part 2Anonymous 4txA8N8etNo ratings yet
- Previous PLE QuestionsDocument3 pagesPrevious PLE QuestionsGrace Benero Pequero0% (1)
- Analytical Methods For Amino Acid Determination in OrganismsDocument18 pagesAnalytical Methods For Amino Acid Determination in OrganismsVeneta GizdakovaNo ratings yet
- A General Procedure For Mitsunobu Inversion of Sterically Hindered Alcohols - Inversion of Menthol. (1S, 2S, 5R) - 5-Methyl-2 - (1-Methylethyl) Cyclohexyl 4-Nitrobenzoate PDFDocument4 pagesA General Procedure For Mitsunobu Inversion of Sterically Hindered Alcohols - Inversion of Menthol. (1S, 2S, 5R) - 5-Methyl-2 - (1-Methylethyl) Cyclohexyl 4-Nitrobenzoate PDFthamtusieuquayNo ratings yet
- Oxford GR 10 Topic 1 Matter & ClassificationDocument54 pagesOxford GR 10 Topic 1 Matter & ClassificationkhotsoNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaAudry YuniarNo ratings yet
- Uncertainty Related To The Use Of: Relative Retention Times in Pharmaceutical AnalysisDocument7 pagesUncertainty Related To The Use Of: Relative Retention Times in Pharmaceutical AnalysisnmmMJKJNo ratings yet
- Gas Chromatography, GCDocument85 pagesGas Chromatography, GCShaise Jacob67% (3)
- Adenosine Injection: 2348 Adenosine / Official Monographs USP 39Document2 pagesAdenosine Injection: 2348 Adenosine / Official Monographs USP 39Luz De MarNo ratings yet
- Science7 Q1 WK5Document3 pagesScience7 Q1 WK5hannahsofiapreyesNo ratings yet
- PrefaceDocument566 pagesPrefaceNurlaini NasutionNo ratings yet
- Poster B12Document1 pagePoster B12Vikas GoyalNo ratings yet
- New Trends in Forced Degradation StudiesDocument10 pagesNew Trends in Forced Degradation StudiesLina SakellariouNo ratings yet
- HPLC Column Phenomenex LunaDocument34 pagesHPLC Column Phenomenex LunaShiraz Khan0% (1)
- Separation, Electroanalytical and Spectrometric TechniquesDocument115 pagesSeparation, Electroanalytical and Spectrometric TechniquesRicardo SimõesNo ratings yet
- Chromatography PharmacyDocument41 pagesChromatography PharmacyfarisaNo ratings yet
- Analytical Tasks - Efficiently Solved by HPTLC: Camag Bibliography ServiceDocument68 pagesAnalytical Tasks - Efficiently Solved by HPTLC: Camag Bibliography ServiceDarian HerascuNo ratings yet
- MS Solutions: Tech TipDocument11 pagesMS Solutions: Tech TipKelumNo ratings yet
- Extension of The QuEChERS Method For Pesticide Residues Cereals, PeanutsDocument9 pagesExtension of The QuEChERS Method For Pesticide Residues Cereals, PeanutsrumitpashaNo ratings yet
- International Biodeterioration & Biodegradation: Daiyong Deng, Jun Guo, Guoqu Zeng, Guoping SunDocument7 pagesInternational Biodeterioration & Biodegradation: Daiyong Deng, Jun Guo, Guoqu Zeng, Guoping SunVenny SandjajaNo ratings yet
- ICW-3000 Water Purification System - MerckmilliporeDocument2 pagesICW-3000 Water Purification System - MerckmilliporeMerck IndiaNo ratings yet
- HPLC 2015Document102 pagesHPLC 2015Ojan FauzanNo ratings yet
- Applications of High Performance Liquid ChromatographyDocument3 pagesApplications of High Performance Liquid ChromatographyKavisa GhoshNo ratings yet
- Course Outline CEV444 (Sep 2017-Jan 2018)Document7 pagesCourse Outline CEV444 (Sep 2017-Jan 2018)Solehah OmarNo ratings yet
- Cbiescco 02Document7 pagesCbiescco 02Rishabh Bhati100% (1)
- pdf01 PDFDocument44 pagespdf01 PDFRafi IqbalNo ratings yet
- Kelebihan Kekurangan Kromatografi KolomDocument8 pagesKelebihan Kekurangan Kromatografi KolomFendy FendyNo ratings yet
- High Performance Liquid Chromatography (HPLC) : Presenter: Nandit P BDocument39 pagesHigh Performance Liquid Chromatography (HPLC) : Presenter: Nandit P BNandit BanawalikarNo ratings yet
- s00226 018 1057 3Document15 pagess00226 018 1057 3Aeric HalzNo ratings yet







































































































Download as pdf or txt
You might also like
- FRCPath Mock 2014 Model AnswersDocument29 pagesFRCPath Mock 2014 Model Answersmonday125No ratings yet
- Ganong - Physiology Self - Assessment Questions - 03Document46 pagesGanong - Physiology Self - Assessment Questions - 03Anonymous 4txA8N8et100% (3)
- Chemistry of CannabisDocument52 pagesChemistry of Cannabisciborg1978No ratings yet
- Chromatography LabDocument9 pagesChromatography Labjtrumpeter224100% (1)
- Poisoning: Overview of Pediatric Poisoning, Diagnosis and Treatment Summary of The Most Encountered PoisoningDocument46 pagesPoisoning: Overview of Pediatric Poisoning, Diagnosis and Treatment Summary of The Most Encountered PoisoningSergey DukkNo ratings yet
- Poisoning Stage V - 2020Document96 pagesPoisoning Stage V - 2020Sarper Hikmet TAZENo ratings yet
- Poisoning PDFDocument124 pagesPoisoning PDFDawn WRein Legaspi67% (3)
- Alcohol ToxicityDocument81 pagesAlcohol ToxicityKarim RezaNo ratings yet
- Toxic Alcohols - High Yields NEJMDocument21 pagesToxic Alcohols - High Yields NEJMDr. Shanojan Thiyagalingam, FRCPC FACPNo ratings yet
- Approach To Poisoned PatientDocument90 pagesApproach To Poisoned PatientGopi KrishnanNo ratings yet
- UMBC CC-EMTP Class Notes, FLCC Class 2010Document93 pagesUMBC CC-EMTP Class Notes, FLCC Class 2010Marc LaBarberaNo ratings yet
- Toxic AlcoholsDocument4 pagesToxic AlcoholsKaran SandhuNo ratings yet
- Dyah Trifianingsih, S. Kep. Ners. M. KepDocument76 pagesDyah Trifianingsih, S. Kep. Ners. M. KepSiprianus S SNo ratings yet
- Alcohol & Glycols: Group # 5 Aranas, Roxette Louraine Ardivilla, Gazel Myrrh Hugo, KevinDocument30 pagesAlcohol & Glycols: Group # 5 Aranas, Roxette Louraine Ardivilla, Gazel Myrrh Hugo, KevinRoxette Louraine R. AranasNo ratings yet
- AlcoholsDocument23 pagesAlcoholsdhaineyNo ratings yet
- Tox CasesDocument7 pagesTox CasesNeo Mervyn Monaheng100% (1)
- Drug Toxicology: Agung Nova Mahendra Department of Pharmacology & Therapy Faculty of Medicine, Udayana UniversityDocument27 pagesDrug Toxicology: Agung Nova Mahendra Department of Pharmacology & Therapy Faculty of Medicine, Udayana Universitywayan lentaraNo ratings yet
- 41 Clinical Cases in Biochemistry UKDocument2 pages41 Clinical Cases in Biochemistry UKAlexandra Ioana MoatarNo ratings yet
- Toxicology Lecture 10 (Chapter 7 Volatiles)Document22 pagesToxicology Lecture 10 (Chapter 7 Volatiles)MowlidAbdirahman Ali madaaleNo ratings yet
- Respiratory Acidosis Is Characterized by An Increase in The pCODocument3 pagesRespiratory Acidosis Is Characterized by An Increase in The pCOMwanja MosesNo ratings yet
- 5 2015 Farmako-ToxicologyDocument71 pages5 2015 Farmako-ToxicologyIkhzan PriolaksanaNo ratings yet
- Chemical Pathology Practical ExamDocument46 pagesChemical Pathology Practical ExamAbdulsamad AfolabiNo ratings yet
- Michael Chansky Acid Base Made Easy HandoutDocument18 pagesMichael Chansky Acid Base Made Easy HandoutTeguh RamadhanNo ratings yet
- Alcohols Ethanol, MethanolDocument55 pagesAlcohols Ethanol, MethanoljayNo ratings yet
- Acid Base Disorders Peter SehaDocument29 pagesAcid Base Disorders Peter SehaPeter SehaNo ratings yet
- Respiratory Assessment FindingsDocument197 pagesRespiratory Assessment Findingsannatw100% (2)
- Adi - IntoxicationDocument52 pagesAdi - IntoxicationAdi WidanaNo ratings yet
- Questions To Consider:: Ethylene Glycol Poisoning. Ethylene Glycol Chemically Occupies A Position Between EthylDocument4 pagesQuestions To Consider:: Ethylene Glycol Poisoning. Ethylene Glycol Chemically Occupies A Position Between EthylJeanette Miña GrajoNo ratings yet
- Anion Gap Metabolic Acidosis: More Then Just A Mud PileDocument21 pagesAnion Gap Metabolic Acidosis: More Then Just A Mud PileFarah SyazanaNo ratings yet
- Management of Poisoned PatientsDocument56 pagesManagement of Poisoned PatientsAmmarah TaimurNo ratings yet
- Acid Base PhysiologyDocument4 pagesAcid Base PhysiologyGhadeer EbraheemNo ratings yet
- ABG Algorithm PDFDocument2 pagesABG Algorithm PDFamin2014No ratings yet
- Module Iii Lab Manual (2024)Document20 pagesModule Iii Lab Manual (2024)ur.yared21No ratings yet
- Rat PoisonDocument41 pagesRat Poisonkhizra mumtazNo ratings yet
- Approach To Acid-Base Problems: DR Frank DalyDocument57 pagesApproach To Acid-Base Problems: DR Frank DalyscanutdNo ratings yet
- Fluid and ElectrolytesDocument14 pagesFluid and Electrolytesstring44100% (2)
- Moderator: Dr. R. K. Yadav (MD) Presented By: Ashish JaisawalDocument47 pagesModerator: Dr. R. K. Yadav (MD) Presented By: Ashish Jaisawalimranqazi11No ratings yet
- Final Exam Focus SheetDocument9 pagesFinal Exam Focus SheetDane WrightNo ratings yet
- Acid-Base Interpretation: APRIL 4, 2017Document9 pagesAcid-Base Interpretation: APRIL 4, 2017mohamedsmnNo ratings yet
- General Principles and Management of PoisonsDocument5 pagesGeneral Principles and Management of PoisonsOkpetah Chioma christabelNo ratings yet
- Drug OverdoseDocument94 pagesDrug Overdosemicheal1960No ratings yet
- Student Tox LectureDocument49 pagesStudent Tox Lecturelenin_villaltaNo ratings yet
- ABG MMHG InterpretationDocument92 pagesABG MMHG InterpretationManmeet SNo ratings yet
- Acid Base Disorders DR Kwaifa - PPTX 1Document99 pagesAcid Base Disorders DR Kwaifa - PPTX 1DICKSONNo ratings yet
- Ethylene Glycol Toxicosis in Animals - Toxicology - MSD Veterinary ManualDocument6 pagesEthylene Glycol Toxicosis in Animals - Toxicology - MSD Veterinary ManualMuhammad AgussalimNo ratings yet
- Synthesis Final ReviewDocument20 pagesSynthesis Final ReviewSamNo ratings yet
- Poisoning in ChildrenDocument11 pagesPoisoning in ChildrenAndriana HalfienNo ratings yet
- Body Fluids and ElectrolytesDocument42 pagesBody Fluids and ElectrolytesQusaiBadr100% (1)
- Tugas GinjalDocument22 pagesTugas GinjalAnastasia MargaretNo ratings yet
- Acid Base EquationsDocument21 pagesAcid Base EquationsBen JonesNo ratings yet
- Assignment: ToxicologyDocument8 pagesAssignment: ToxicologyAyesha LiaqatNo ratings yet
- Anion Gap Metabolic Acidemia Case BasedDocument4 pagesAnion Gap Metabolic Acidemia Case Basedspiros.a.markouNo ratings yet
- Case Report: An Unconscious Man With Profound Drug-Induced HypoglycaemiaDocument6 pagesCase Report: An Unconscious Man With Profound Drug-Induced Hypoglycaemiagevowo3277No ratings yet
- Acute Poisoning of Therapeutic Agents: by Alemayehu TomaDocument42 pagesAcute Poisoning of Therapeutic Agents: by Alemayehu TomaYohannis AsefaNo ratings yet
- Mnemonics: Do Not Adsorb To CharcoalDocument25 pagesMnemonics: Do Not Adsorb To CharcoalJiaYee GoNo ratings yet
- ABG Interpretation 1Document59 pagesABG Interpretation 1Sura KwakNo ratings yet
- Chapter Four: Chemical Analysis of UrineDocument174 pagesChapter Four: Chemical Analysis of UrineRebuma BeleteNo ratings yet
- AlcohoDocument32 pagesAlcohoVaibhav KaroliyaNo ratings yet
- Enzyme-summary (1)Document7 pagesEnzyme-summary (1)Aira Jane GamboaNo ratings yet
- ELECTROLYTES (Na & K)Document3 pagesELECTROLYTES (Na & K)Alondra SagarioNo ratings yet
- Alcohol Toxicity PDFDocument20 pagesAlcohol Toxicity PDFNabila Fatmayday UdiyahNo ratings yet
- The Impact Of Alcohol On The Brain - Based On The Teachings Of Dr. Andrew Huberman: Examining The Complex Interplay Between Alcohol And NeurobiologyFrom EverandThe Impact Of Alcohol On The Brain - Based On The Teachings Of Dr. Andrew Huberman: Examining The Complex Interplay Between Alcohol And NeurobiologyNo ratings yet
- Pass Paces EbDocument10 pagesPass Paces EbAnonymous 4txA8N8etNo ratings yet
- H IsselbacherDocument5 pagesH IsselbacherAnonymous 4txA8N8etNo ratings yet
- Topics Runtime: Subjects AnatomyDocument2 pagesTopics Runtime: Subjects AnatomyAnonymous 4txA8N8etNo ratings yet
- Hp165-02b-Nash (FF 050816v) ProtegidoDocument9 pagesHp165-02b-Nash (FF 050816v) ProtegidoAnonymous 4txA8N8etNo ratings yet
- Adpkd: Autosomal Dominant Polycystic Kidney DiseaseDocument7 pagesAdpkd: Autosomal Dominant Polycystic Kidney DiseaseAnonymous 4txA8N8etNo ratings yet
- Hanzi Pinyin English: HSK Level 2Document5 pagesHanzi Pinyin English: HSK Level 2Anonymous 4txA8N8etNo ratings yet
- Genetics 50qDocument62 pagesGenetics 50qAnonymous 4txA8N8etNo ratings yet
- Radiology Reviewed Meds Reviewed Pathology Reviewed Micro Reviewed "FASTHUG" CheckedDocument1 pageRadiology Reviewed Meds Reviewed Pathology Reviewed Micro Reviewed "FASTHUG" CheckedAnonymous 4txA8N8etNo ratings yet
- 6 Steps in Assisting in Cardiac Rhythm InterpretationDocument1 page6 Steps in Assisting in Cardiac Rhythm InterpretationAnonymous 4txA8N8etNo ratings yet
- EMQExample RacpDocument5 pagesEMQExample RacpAnonymous 4txA8N8etNo ratings yet
- Brunicardi-1996-Time Management - A RDocument7 pagesBrunicardi-1996-Time Management - A RAnonymous 4txA8N8etNo ratings yet
- Abdominal Exam DATEDocument3 pagesAbdominal Exam DATEAnonymous 4txA8N8etNo ratings yet
- Effective Feedback Skills: Sally Santen MD, PHDDocument9 pagesEffective Feedback Skills: Sally Santen MD, PHDAnonymous 4txA8N8etNo ratings yet
- Lymphoproliferative Disorders Part 2Document7 pagesLymphoproliferative Disorders Part 2Anonymous 4txA8N8etNo ratings yet
- Previous PLE QuestionsDocument3 pagesPrevious PLE QuestionsGrace Benero Pequero0% (1)
- Analytical Methods For Amino Acid Determination in OrganismsDocument18 pagesAnalytical Methods For Amino Acid Determination in OrganismsVeneta GizdakovaNo ratings yet
- A General Procedure For Mitsunobu Inversion of Sterically Hindered Alcohols - Inversion of Menthol. (1S, 2S, 5R) - 5-Methyl-2 - (1-Methylethyl) Cyclohexyl 4-Nitrobenzoate PDFDocument4 pagesA General Procedure For Mitsunobu Inversion of Sterically Hindered Alcohols - Inversion of Menthol. (1S, 2S, 5R) - 5-Methyl-2 - (1-Methylethyl) Cyclohexyl 4-Nitrobenzoate PDFthamtusieuquayNo ratings yet
- Oxford GR 10 Topic 1 Matter & ClassificationDocument54 pagesOxford GR 10 Topic 1 Matter & ClassificationkhotsoNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaAudry YuniarNo ratings yet
- Uncertainty Related To The Use Of: Relative Retention Times in Pharmaceutical AnalysisDocument7 pagesUncertainty Related To The Use Of: Relative Retention Times in Pharmaceutical AnalysisnmmMJKJNo ratings yet
- Gas Chromatography, GCDocument85 pagesGas Chromatography, GCShaise Jacob67% (3)
- Adenosine Injection: 2348 Adenosine / Official Monographs USP 39Document2 pagesAdenosine Injection: 2348 Adenosine / Official Monographs USP 39Luz De MarNo ratings yet
- Science7 Q1 WK5Document3 pagesScience7 Q1 WK5hannahsofiapreyesNo ratings yet
- PrefaceDocument566 pagesPrefaceNurlaini NasutionNo ratings yet
- Poster B12Document1 pagePoster B12Vikas GoyalNo ratings yet
- New Trends in Forced Degradation StudiesDocument10 pagesNew Trends in Forced Degradation StudiesLina SakellariouNo ratings yet
- HPLC Column Phenomenex LunaDocument34 pagesHPLC Column Phenomenex LunaShiraz Khan0% (1)
- Separation, Electroanalytical and Spectrometric TechniquesDocument115 pagesSeparation, Electroanalytical and Spectrometric TechniquesRicardo SimõesNo ratings yet
- Chromatography PharmacyDocument41 pagesChromatography PharmacyfarisaNo ratings yet
- Analytical Tasks - Efficiently Solved by HPTLC: Camag Bibliography ServiceDocument68 pagesAnalytical Tasks - Efficiently Solved by HPTLC: Camag Bibliography ServiceDarian HerascuNo ratings yet
- MS Solutions: Tech TipDocument11 pagesMS Solutions: Tech TipKelumNo ratings yet
- Extension of The QuEChERS Method For Pesticide Residues Cereals, PeanutsDocument9 pagesExtension of The QuEChERS Method For Pesticide Residues Cereals, PeanutsrumitpashaNo ratings yet
- International Biodeterioration & Biodegradation: Daiyong Deng, Jun Guo, Guoqu Zeng, Guoping SunDocument7 pagesInternational Biodeterioration & Biodegradation: Daiyong Deng, Jun Guo, Guoqu Zeng, Guoping SunVenny SandjajaNo ratings yet
- ICW-3000 Water Purification System - MerckmilliporeDocument2 pagesICW-3000 Water Purification System - MerckmilliporeMerck IndiaNo ratings yet
- HPLC 2015Document102 pagesHPLC 2015Ojan FauzanNo ratings yet
- Applications of High Performance Liquid ChromatographyDocument3 pagesApplications of High Performance Liquid ChromatographyKavisa GhoshNo ratings yet
- Course Outline CEV444 (Sep 2017-Jan 2018)Document7 pagesCourse Outline CEV444 (Sep 2017-Jan 2018)Solehah OmarNo ratings yet
- Cbiescco 02Document7 pagesCbiescco 02Rishabh Bhati100% (1)
- pdf01 PDFDocument44 pagespdf01 PDFRafi IqbalNo ratings yet
- Kelebihan Kekurangan Kromatografi KolomDocument8 pagesKelebihan Kekurangan Kromatografi KolomFendy FendyNo ratings yet
- High Performance Liquid Chromatography (HPLC) : Presenter: Nandit P BDocument39 pagesHigh Performance Liquid Chromatography (HPLC) : Presenter: Nandit P BNandit BanawalikarNo ratings yet
- s00226 018 1057 3Document15 pagess00226 018 1057 3Aeric HalzNo ratings yet