Download as pdf or txt
You might also like
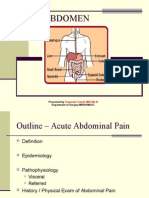
- Acute Abdominal PainDocument72 pagesAcute Abdominal PainJoseph Stans Kasirye100% (1)
- The Radiology Handbook: A Pocket Guide to Medical ImagingFrom EverandThe Radiology Handbook: A Pocket Guide to Medical ImagingRating: 3.5 out of 5 stars3.5/5 (8)
- MechanicalLumbarDisorders RAH AlliedHealth 1201023Document3 pagesMechanicalLumbarDisorders RAH AlliedHealth 1201023Ismail LubisNo ratings yet
- Osteoarthritis of The Knee: By. Dr. Andi PangeranDocument38 pagesOsteoarthritis of The Knee: By. Dr. Andi PangeranPangeran AndiNo ratings yet
- Osteoarthritis: By: Vien HardiyantiDocument37 pagesOsteoarthritis: By: Vien HardiyantiPhannyta CherryNo ratings yet
- Dr. Indarwati Setyaningsih, SP.S (K) Consultant Neurologist Department of Neurology RSUP DR - SardjitoDocument85 pagesDr. Indarwati Setyaningsih, SP.S (K) Consultant Neurologist Department of Neurology RSUP DR - Sardjitoyuyun072015100% (1)
- NCPDocument11 pagesNCPzharienabNo ratings yet
- Family Medicine DepartmentDocument45 pagesFamily Medicine Departmentسليمان فايزNo ratings yet
- Juvenile ArthritisDocument11 pagesJuvenile ArthritisElvisNo ratings yet
- Diagnosis Problem of DefecationDocument36 pagesDiagnosis Problem of DefecationMico Ga Bisa Gendut100% (1)
- Disorder of Musculo - System. LeatestDocument178 pagesDisorder of Musculo - System. LeatestCheru TecheNo ratings yet
- Impaired Gas Exchange Related To Airflow ObstructionDocument6 pagesImpaired Gas Exchange Related To Airflow ObstructionNicole BuenaventuraNo ratings yet
- Name: Biadsi Odey Group:M1560 SUBJECT: Rheumatology (Patenit Presentation) - Data: 31/03/2019Document10 pagesName: Biadsi Odey Group:M1560 SUBJECT: Rheumatology (Patenit Presentation) - Data: 31/03/2019Galina LozovanuNo ratings yet
- NCP CvaDocument7 pagesNCP CvaEmerson SilverioNo ratings yet
- OsteoarthritisDocument35 pagesOsteoarthritisTazqirotul UlaNo ratings yet
- Acute Abdominal Pain 2Document72 pagesAcute Abdominal Pain 2ngockhanh1971No ratings yet
- Acute Abdominal Pain: Presented by Dr. Kolahdouzan Thoracic Surgen Alzahra HospitalDocument77 pagesAcute Abdominal Pain: Presented by Dr. Kolahdouzan Thoracic Surgen Alzahra HospitalGraceline Margaretha Marsintauly SianiparNo ratings yet
- Acute Abdomen: KGD 1 Ns. Siska Natalia, MSN - Palliative CareDocument17 pagesAcute Abdomen: KGD 1 Ns. Siska Natalia, MSN - Palliative Caremuhammad putra hidayatNo ratings yet
- Planning (Nursing Care Plans)Document10 pagesPlanning (Nursing Care Plans)Kier Jucar de GuzmanNo ratings yet
- Osteoarthritis: Uyenvy Pham, M.D. Swedish Geriatric Fellow March 22, 2011Document45 pagesOsteoarthritis: Uyenvy Pham, M.D. Swedish Geriatric Fellow March 22, 2011Saya MenangNo ratings yet
- Basic Human Needs Mobility & The Hazards of ImmobilityDocument54 pagesBasic Human Needs Mobility & The Hazards of ImmobilityZsuzsanna MesterNo ratings yet
- A Case Study of BKA On CKD V Secondary To DM Nephropathy PatientDocument23 pagesA Case Study of BKA On CKD V Secondary To DM Nephropathy PatientSimon Manansala100% (1)
- DengueDocument14 pagesDengueKarenn Joy Concepcion OctubreNo ratings yet
- GADAHDocument7 pagesGADAHelchachel492No ratings yet
- North American Spine Society Public Education SeriesDocument12 pagesNorth American Spine Society Public Education SeriesVanitha Ratha KrishnanNo ratings yet
- Multiple Sclerosis (MS)Document15 pagesMultiple Sclerosis (MS)Arianna Jasmine MabungaNo ratings yet
- Surgery: Low Back PainDocument35 pagesSurgery: Low Back PainMonette Abalos MendovaNo ratings yet
- OsteoarthritisDocument28 pagesOsteoarthritisLydia Lopz MsnrncdNo ratings yet
- Perspectives On The Sacroiliac JointDocument25 pagesPerspectives On The Sacroiliac JointChitra RajanNo ratings yet
- PT For Peripheral Vascular Disorders: Imtiyaz Ali Lecturer, UTARDocument19 pagesPT For Peripheral Vascular Disorders: Imtiyaz Ali Lecturer, UTARSalman KhanNo ratings yet
- Osteoarthritis (NHT)Document25 pagesOsteoarthritis (NHT)nowemgf100% (1)
- PancreatitisDocument18 pagesPancreatitisMihir PatelNo ratings yet
- Medical SurgicalDocument30 pagesMedical SurgicalGulshad AfridiNo ratings yet
- ARTHRITIS TB KNEE HIP BPTDocument84 pagesARTHRITIS TB KNEE HIP BPTMiso100% (1)
- Pubalgia 1Document11 pagesPubalgia 1Carlos Alberto Mac-kay VillagranNo ratings yet
- GS 201-250Document19 pagesGS 201-250Sara Abdul RahmanNo ratings yet
- Manual Therapy (Shs.405) : Dr. Muhamad Rizwan LecturerDocument28 pagesManual Therapy (Shs.405) : Dr. Muhamad Rizwan Lectureraad wwwNo ratings yet
- Nurul Qalby C111 13 064 A. Anisa Nasir C111 13 082 Sitti Magfirah Adnan C111 13 090Document32 pagesNurul Qalby C111 13 064 A. Anisa Nasir C111 13 082 Sitti Magfirah Adnan C111 13 090Nurul Qalby AmiluddinNo ratings yet
- Case StudypcolDocument5 pagesCase StudypcolJoshua AysonNo ratings yet
- Risk For Ineffective Tissue PerfusionDocument5 pagesRisk For Ineffective Tissue PerfusionElle Oranza100% (1)
- AAA Case ReportDocument6 pagesAAA Case Reportfelix_3264_hariantoNo ratings yet
- EcgDocument3 pagesEcgPhilip Royce EmpeñoNo ratings yet
- Achilles TendinopathyDocument9 pagesAchilles TendinopathysynysterbraveNo ratings yet
- Rheumatoid ArthritisDocument30 pagesRheumatoid ArthritisMelisaNo ratings yet
- AbdomenDocument54 pagesAbdomenChaichon PochaiNo ratings yet
- ClaudicationDocument6 pagesClaudicationdvenumohanNo ratings yet
- Ankylosing Spondylitis (Marie-Strümpell Disease/ Bechterew's Disease)Document39 pagesAnkylosing Spondylitis (Marie-Strümpell Disease/ Bechterew's Disease)MoineeNo ratings yet
- Practice EssentialsDocument5 pagesPractice EssentialsSelam LechissaNo ratings yet
- Emergency Nurse Protocol Back PainDocument2 pagesEmergency Nurse Protocol Back PainSimon S. KledenNo ratings yet
- Peripheral Vascular Disease Surgical PresentationDocument26 pagesPeripheral Vascular Disease Surgical Presentationqreen100% (1)
- Knee Osteoarthritis: DefinitionDocument19 pagesKnee Osteoarthritis: DefinitionShrouq BadrNo ratings yet
- Subjective: Goals: - : Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationDocument18 pagesSubjective: Goals: - : Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationJennalyn Padua SevillaNo ratings yet
- ABC Emergency Differential DiagnosisffDocument3 pagesABC Emergency Differential Diagnosisffsharu4291No ratings yet
- Case Study OrthoDocument21 pagesCase Study Orthojoshua_santiago_5No ratings yet
- Osteoarthritis: Uyenvy Pham, M.D. Swedish Geriatric Fellow March 22, 2011Document45 pagesOsteoarthritis: Uyenvy Pham, M.D. Swedish Geriatric Fellow March 22, 2011virupanagoudaNo ratings yet
- Abdominal Pain: Essential Diagnosis and Management in Acute MedicineFrom EverandAbdominal Pain: Essential Diagnosis and Management in Acute MedicineNo ratings yet
- Fast Facts: Perioperative Pain: Effective management has numerous benefitsFrom EverandFast Facts: Perioperative Pain: Effective management has numerous benefitsNo ratings yet
- Hepatic Cirrhosis (肝硬化): Yu BaopingDocument62 pagesHepatic Cirrhosis (肝硬化): Yu BaopingKurbulNo ratings yet
- Idiopathic Thrombocytopenic Purpura Case StudyDocument38 pagesIdiopathic Thrombocytopenic Purpura Case StudyKurbulNo ratings yet
- Chapter 6Document11 pagesChapter 6KurbulNo ratings yet
- Lapkas PP (STEMI)Document68 pagesLapkas PP (STEMI)KurbulNo ratings yet
- Mental BondageDocument424 pagesMental BondageRedza92% (12)
- HLLQP QuickFact FormulaSheet 2016Document2 pagesHLLQP QuickFact FormulaSheet 2016nandhinigrmNo ratings yet
- First Certificate Booklet 2Document89 pagesFirst Certificate Booklet 2Alina TeranNo ratings yet
- Omengan Vs PNBDocument3 pagesOmengan Vs PNBJim de los Santos100% (1)
- 1 - 32 F-16C - ThunderbirdsDocument3 pages1 - 32 F-16C - ThunderbirdsDesmond GracianniNo ratings yet
- 1 s2.0 S0891422221001827 MainDocument9 pages1 s2.0 S0891422221001827 MainCarmelo VillafrancaNo ratings yet
- 2170908Document19 pages2170908bhavikNo ratings yet
- Motor Claim Form THE ORIENTAL INSURANCE CO. LTD.Document4 pagesMotor Claim Form THE ORIENTAL INSURANCE CO. LTD.rajiv.surveyor7145No ratings yet
- Duhamel's PrincipleDocument14 pagesDuhamel's Principlejoel24348584No ratings yet
- Uoc Annual Report 2018Document112 pagesUoc Annual Report 2018GitanjaliNo ratings yet
- CDHA Infection ControlDocument2 pagesCDHA Infection ControlAliaa El WakeelNo ratings yet
- ABB Fittings PlugsDocument204 pagesABB Fittings PlugsjohnNo ratings yet
- The Sound of Music I and IiDocument2 pagesThe Sound of Music I and Iiamjad jr9No ratings yet
- Criminal Law I SyllabusDocument4 pagesCriminal Law I SyllabusNashiba Dida-AgunNo ratings yet
- Facilio State of Operations and Maintenance SoftwareDocument25 pagesFacilio State of Operations and Maintenance Softwarearunkumar277041No ratings yet
- Sarah Butts ResumeDocument2 pagesSarah Butts Resumeapi-743828243No ratings yet
- Research On Process of Raising Funds Through QipDocument5 pagesResearch On Process of Raising Funds Through QipRachit SharmaNo ratings yet
- A Handbook of English Literature by Faizal Risdianto: P Oetr YDocument24 pagesA Handbook of English Literature by Faizal Risdianto: P Oetr YaYu pradhitiyanNo ratings yet
- DB (04.2013) HiromiDocument7 pagesDB (04.2013) HiromiLew Quzmic Baltiysky75% (4)
- OfficialRules-BritneySpearsNYE CRDocument9 pagesOfficialRules-BritneySpearsNYE CRAbelardo Ch.No ratings yet
- Chapter 2Document5 pagesChapter 2anon-668822No ratings yet
- African Literature - WikipediaDocument1 pageAfrican Literature - Wikipediatem ijeNo ratings yet
- Following The Cap Figure by Lydia KievenDocument415 pagesFollowing The Cap Figure by Lydia KievenCatherinNo ratings yet
- Tia HistoryDocument11 pagesTia HistoryTiara AlmeidaNo ratings yet
- Neom 1revDocument8 pagesNeom 1revSanyam JainNo ratings yet
- Covert Extinction TherapyDocument6 pagesCovert Extinction TherapyAnet Augustine AnetNo ratings yet
- Experiment 6: Method of Mixture ObjectiveDocument3 pagesExperiment 6: Method of Mixture Objectiveshark eyeNo ratings yet
- Ancient IndiaDocument9 pagesAncient IndiaAchanger AcherNo ratings yet
- A.1155 (32) - Procedures For Port State Control, 2021Document141 pagesA.1155 (32) - Procedures For Port State Control, 2021Karima BelbraikNo ratings yet
- Q4FY23 HMCL Transcript-230711-085731Document19 pagesQ4FY23 HMCL Transcript-230711-085731vishwesh gautamNo ratings yet
- (A3) The Genuine Marks of The Disciples of ChristDocument7 pages(A3) The Genuine Marks of The Disciples of ChristDenmark SaviduriaNo ratings yet