Download as pdf or txt
You might also like
- Can't Hurt Me by David GogginsDocument5 pagesCan't Hurt Me by David GogginsInfinit1381% (16)
- Glissonean Pedicle Transection Method For Hepatic ResectionDocument171 pagesGlissonean Pedicle Transection Method For Hepatic ResectionandreigustvNo ratings yet
- Local Youth Development PlanDocument7 pagesLocal Youth Development PlanClaire Janiola100% (5)
- Annals of Gastroent Surgery 2018 Yamamoto Glissonean Pedicle ApproachDocument5 pagesAnnals of Gastroent Surgery 2018 Yamamoto Glissonean Pedicle Approachvlad111776No ratings yet
- Glissonean Approach To Liver ResectionDocument5 pagesGlissonean Approach To Liver ResectionBibu CristianNo ratings yet
- JHBP 24 17Document7 pagesJHBP 24 17Yacine Tarik AizelNo ratings yet
- Kowalczyk 5 e CH 5Document35 pagesKowalczyk 5 e CH 5rsnsl7410No ratings yet
- Cholecystectomy 4 PrintingDocument19 pagesCholecystectomy 4 PrintingKyle Punzalan100% (2)
- 062012SCNADocument11 pages062012SCNAMc KobaNo ratings yet
- Anatomy of LiverDocument11 pagesAnatomy of LiverSyed NusrathNo ratings yet
- Laparoscopic Cholecystectomy - StatPearls - NCBI BookshelfDocument1 pageLaparoscopic Cholecystectomy - StatPearls - NCBI BookshelfOmar HamwiNo ratings yet
- Hep Resxn TechDocument33 pagesHep Resxn TechKartikKulshresthaNo ratings yet
- BiliaryDocument41 pagesBiliaryayundyawibowoNo ratings yet
- Liver - WikipediaDocument148 pagesLiver - WikipediaMuhammad HuzaifaNo ratings yet
- Bile Leakage During Laparoscopic Cholecystectomy A Rare Case of Aberrant AnatomyDocument6 pagesBile Leakage During Laparoscopic Cholecystectomy A Rare Case of Aberrant AnatomyEditor IJTSRDNo ratings yet
- Chapter 32: Gallbladder and The Extrahepatic Biliary System: Key PointsDocument43 pagesChapter 32: Gallbladder and The Extrahepatic Biliary System: Key PointsSteven Tapia VillacísNo ratings yet
- Anatomia Laparoscopica A Ficatului - Jurnalul de ChirurgieDocument11 pagesAnatomia Laparoscopica A Ficatului - Jurnalul de ChirurgieDan PintilescuNo ratings yet
- The Gallbladder AnatomyDocument10 pagesThe Gallbladder AnatomyClaudia IlieNo ratings yet
- ZollingerDocument5 pagesZollingerSantiago Xicotencatl MendezNo ratings yet
- Sur - Atlas of Gastrointestinal Surgery (Cameron) NewDocument474 pagesSur - Atlas of Gastrointestinal Surgery (Cameron) Newalisolouki40100% (12)
- Hepato-Biliary System 26.4.2016Document59 pagesHepato-Biliary System 26.4.2016S B SayedNo ratings yet
- Bowel Obstruction Case StudyDocument11 pagesBowel Obstruction Case StudyFatimah Batool NawazNo ratings yet
- Anatomia de Vesicula BiliarDocument5 pagesAnatomia de Vesicula BiliarHumberto CamposNo ratings yet
- 2972-Surgery-Tivers-Reducing Stress and - EngDocument6 pages2972-Surgery-Tivers-Reducing Stress and - EngSilvia RoseNo ratings yet
- Safe Laparoscopic Cholecystectomy: Kavin Raj PDocument18 pagesSafe Laparoscopic Cholecystectomy: Kavin Raj PkavinNo ratings yet
- Hepatic Resection Surgical Techniques: Nathaniel V. Talibong Group 8Document12 pagesHepatic Resection Surgical Techniques: Nathaniel V. Talibong Group 8NateNo ratings yet
- PUT 822 Coursework 1Document19 pagesPUT 822 Coursework 1Stephen KokoNo ratings yet
- Urinary Diversion Following Cystectomy: EAU Update SeriesDocument9 pagesUrinary Diversion Following Cystectomy: EAU Update SeriesmoetazNo ratings yet
- Review Article: Relevant Biliary Anatomy During CholecystectomyDocument11 pagesReview Article: Relevant Biliary Anatomy During CholecystectomyAbrar SabawiNo ratings yet
- A Case Report On Biliary Ileus As A Rare Trigger For Intestinal ObstructionDocument7 pagesA Case Report On Biliary Ileus As A Rare Trigger For Intestinal ObstructionIJAR JOURNALNo ratings yet
- Hepatic Subcapsular BIloma A Rare Complication of Laparoscopic CholecystectomyDocument4 pagesHepatic Subcapsular BIloma A Rare Complication of Laparoscopic CholecystectomyIndra PrimaNo ratings yet
- Bio Artifical LiverDocument8 pagesBio Artifical LiverManikandan MurugesanNo ratings yet
- 2 Biliary Anatomy and EmbrDocument16 pages2 Biliary Anatomy and EmbrShawn GravesNo ratings yet
- Ma 05011Document6 pagesMa 05011drelvNo ratings yet
- Case ReportDocument5 pagesCase ReportAmmar magdyNo ratings yet
- Cholecystectomy With Intraoperative CholangiogramDocument8 pagesCholecystectomy With Intraoperative CholangiogramLourd Andrew VillegasNo ratings yet
- Design and Techniques of Surgical ProceduresDocument70 pagesDesign and Techniques of Surgical Proceduresajmahdi2No ratings yet
- Case Report: Cholecystomegaly: A Case Report and Review of The LiteratureDocument5 pagesCase Report: Cholecystomegaly: A Case Report and Review of The LiteratureAnti TjahyaNo ratings yet
- Total Pelvic ExenterationDocument13 pagesTotal Pelvic ExenterationRirin Wahyuni100% (1)
- Case Report - CholesystitisDocument4 pagesCase Report - CholesystitisBenzoyl BeingNo ratings yet
- Surgery of The Liver Biliary Tract: L. H. B Um ArtDocument27 pagesSurgery of The Liver Biliary Tract: L. H. B Um ArtLiana OpriţăNo ratings yet
- Vago ThomasDocument29 pagesVago ThomasEsti Rahmawati SuryaningrumNo ratings yet
- IntesineDocument13 pagesIntesinedesign bahana bahana proNo ratings yet
- Los Terrybles Book TeamDocument9 pagesLos Terrybles Book TeamWildor Herrera GuevaraNo ratings yet
- Case Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyDocument46 pagesCase Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyAjiMary M. DomingoNo ratings yet
- The LiverDocument13 pagesThe LiverLizbeth QuinteroNo ratings yet
- Doc1 Obstractive JaundiceDocument7 pagesDoc1 Obstractive JaundiceZhy CaluzaNo ratings yet
- CholecystectomyDocument5 pagesCholecystectomyRachelle Maderazo CartinNo ratings yet
- Acute CholecystitisDocument18 pagesAcute CholecystitisOktavia PutriNo ratings yet
- Cholecystectomy: Navigation SearchDocument4 pagesCholecystectomy: Navigation SearchMohammed OmerNo ratings yet
- Right and Extended Right Colectomy - Open Technique - UpToDateDocument44 pagesRight and Extended Right Colectomy - Open Technique - UpToDateDpxeir PapanikolaouNo ratings yet
- Hepatic PackingDocument4 pagesHepatic PackingRESIDENTES CIRUGIA IMSSNo ratings yet
- Choledocal CystDocument11 pagesCholedocal CystBilly JonatanNo ratings yet
- Intestinal Foreign Bodies: Clinical SignsDocument2 pagesIntestinal Foreign Bodies: Clinical SignsSabreen khattakNo ratings yet
- Pi Is 2213576614000049Document3 pagesPi Is 2213576614000049Ditha FadhilaNo ratings yet
- Ultrasound of The Liver: EFSUMB - European Course BookDocument30 pagesUltrasound of The Liver: EFSUMB - European Course BookYuda Arie DharmawanNo ratings yet
- Ligamentele PeritonealeDocument22 pagesLigamentele PeritonealeNicoleta TudorachiNo ratings yet
- Argh - Ms.id.555581, DR Muhammad Zafar Mengal ArticlesDocument4 pagesArgh - Ms.id.555581, DR Muhammad Zafar Mengal ArticlesMuhammad Zafar MengalNo ratings yet
- Anesthesia for Hepatico-Pancreatic-Biliary Surgery and TransplantationFrom EverandAnesthesia for Hepatico-Pancreatic-Biliary Surgery and TransplantationZoka MilanNo ratings yet
- Difficult Acute Cholecystitis: Treatment and Technical IssuesFrom EverandDifficult Acute Cholecystitis: Treatment and Technical IssuesNo ratings yet
- Renal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledFrom EverandRenal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledNo ratings yet
- Log Book: Approved by The European Board and College of Obstetrics and GynaecologyDocument23 pagesLog Book: Approved by The European Board and College of Obstetrics and Gynaecologyyacine26No ratings yet
- Cal Damone 2009Document1 pageCal Damone 2009yacine26No ratings yet
- Hepatic Surgical AnatomyDocument23 pagesHepatic Surgical Anatomyyacine26No ratings yet
- Roux-en-Y Reconstruction After PancreaticoduodenectomyDocument5 pagesRoux-en-Y Reconstruction After Pancreaticoduodenectomyyacine26No ratings yet
- Omentum: On Omentum by W. MayDocument1 pageOmentum: On Omentum by W. Mayyacine26No ratings yet
- Current Opinion On Lymphadenectomy in Pancreatic Cancer SurgeryDocument5 pagesCurrent Opinion On Lymphadenectomy in Pancreatic Cancer Surgeryyacine26No ratings yet
- Radical Surgery For Cancer of The Pancreas: Kothaj PDocument3 pagesRadical Surgery For Cancer of The Pancreas: Kothaj Pyacine26No ratings yet
- Colostomies..: of Sutrgery: of Proctology 135Document7 pagesColostomies..: of Sutrgery: of Proctology 135yacine26No ratings yet
- A Simple Technique of Portal Vein Resection and Reconstruction During PancreaticoduodenectomyDocument6 pagesA Simple Technique of Portal Vein Resection and Reconstruction During Pancreaticoduodenectomyyacine26No ratings yet
- 01 HepatogastroDocument3 pages01 Hepatogastroyacine26No ratings yet
- Surgicalmanagement Ofcervicallymph Nodesindifferentiated ThyroidcancerDocument0 pagesSurgicalmanagement Ofcervicallymph Nodesindifferentiated Thyroidcanceryacine26No ratings yet
- 1 s2.0 S0002961011001097 MainDocument5 pages1 s2.0 S0002961011001097 Mainyacine26No ratings yet
- Manual of Temporal Bone DissectionDocument82 pagesManual of Temporal Bone DissectionBungbu Tn100% (4)
- Caring For Your African American/Biracial Child's HairDocument32 pagesCaring For Your African American/Biracial Child's Hair4kidslikemeNo ratings yet
- Joy Trust Fear Surprise Sadness Disgust Anger AnticipationDocument4 pagesJoy Trust Fear Surprise Sadness Disgust Anger AnticipationsatyakaamsNo ratings yet
- Manual 2 PDFDocument442 pagesManual 2 PDFSebastian CoraisacaNo ratings yet
- CRU-83 Combat Edge RegulatorDocument1 pageCRU-83 Combat Edge RegulatorfuccioniNo ratings yet
- Ethics in Healthcare Setting (Therapy)Document10 pagesEthics in Healthcare Setting (Therapy)Milcah ShabanjiNo ratings yet
- Final DraftDocument37 pagesFinal DraftMorareng MariettaNo ratings yet
- Activity No. 2 Disaster RiskDocument3 pagesActivity No. 2 Disaster RiskBUENAVENTURA, GABRIEL JOVANNo ratings yet
- Barrel Firing - Paul WandlessDocument9 pagesBarrel Firing - Paul WandlessStefan Van Cleemput0% (1)
- DRRR2324 Q4 DRRDocument7 pagesDRRR2324 Q4 DRRh4gtg7n55gNo ratings yet
- Anxiety Among High School StudentsDocument21 pagesAnxiety Among High School StudentsFr. Joseph KattakayamNo ratings yet
- Mpeg 750Document2 pagesMpeg 750sudhir5441No ratings yet
- 27-07-2021 HMB EnglishDocument12 pages27-07-2021 HMB EnglishGyan PrakashNo ratings yet
- D154-85 (2009) Standard Guide For Testing VarnishesDocument4 pagesD154-85 (2009) Standard Guide For Testing VarnishesRonny100% (1)
- Review of Agriculture Robotics: Practicality and FeasibilityDocument6 pagesReview of Agriculture Robotics: Practicality and Feasibilityaldy faleraNo ratings yet
- Metal Oxide Varistor Elbow M o V e Surge Arrester Catalog Ca235025enDocument8 pagesMetal Oxide Varistor Elbow M o V e Surge Arrester Catalog Ca235025enale_1905No ratings yet
- Enfield Saheli: Funding NEWSDocument5 pagesEnfield Saheli: Funding NEWSenfieldclubhouseNo ratings yet
- BilcoDocument16 pagesBilcoruloNo ratings yet
- Definition of Terms Mine SurveyingDocument2 pagesDefinition of Terms Mine Surveyingaquariuspj25100% (3)
- Anxiety DisordersDocument10 pagesAnxiety DisordersAhmed AntarNo ratings yet
- 2-BP-3.5K-5K 220v ManualDocument42 pages2-BP-3.5K-5K 220v ManualEcosenseTechnologies GreenenergyNo ratings yet
- Guidelines For Formulating Sensiva SC 50 Into EmulsionsDocument16 pagesGuidelines For Formulating Sensiva SC 50 Into EmulsionsLogdi JamesNo ratings yet
- Partlist Eq114Document16 pagesPartlist Eq114180976No ratings yet
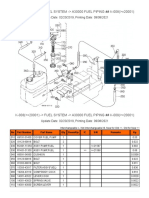
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- LL. B. I Term: Paper - LB - 103 - Law of TortsDocument10 pagesLL. B. I Term: Paper - LB - 103 - Law of TortsFaisal ShahzadNo ratings yet
- Nurse-Patient Interaction Process Recording: College of NursingDocument3 pagesNurse-Patient Interaction Process Recording: College of NursingBianx Flores DosdosNo ratings yet
- International StandardDocument8 pagesInternational Standardnazrul islamNo ratings yet
- A320 Ame Self ExaminationDocument6 pagesA320 Ame Self ExaminationKarwane MuntazireenNo ratings yet