Download as pdf or txt
You might also like
- Layton Skyline Owners ManualDocument3 pagesLayton Skyline Owners ManualJeremy EllisNo ratings yet
- 008 GB e Vidas Assay SolutionsDocument4 pages008 GB e Vidas Assay SolutionsvishnupgiNo ratings yet
- Chapter 7. Longitudinal Studies: Nama: Sofia Marcelina NPM: A1E017005 PRODI: Pendidikan FisikaDocument4 pagesChapter 7. Longitudinal Studies: Nama: Sofia Marcelina NPM: A1E017005 PRODI: Pendidikan FisikaSofia MarcelinaNo ratings yet
- Wijsenbeek2015 Treatment of SarcoidosisDocument17 pagesWijsenbeek2015 Treatment of SarcoidosisJohan ArocaNo ratings yet
- FFFGVDocument10 pagesFFFGVyundaNo ratings yet
- Interventions For Pediatric Sepsis and Their Impact On Outcomes - A Brief ReviewDocument9 pagesInterventions For Pediatric Sepsis and Their Impact On Outcomes - A Brief ReviewJean Paúl LópezNo ratings yet
- Clinical Outcome in Children With Chronic Recurrent Multifocal OsteomyelitisDocument4 pagesClinical Outcome in Children With Chronic Recurrent Multifocal OsteomyelitisJiwo SaciladhNo ratings yet
- Epidemiology and Outcomes of Status Epilepticus - PMC PDFDocument18 pagesEpidemiology and Outcomes of Status Epilepticus - PMC PDFCi CiNo ratings yet
- 1908 Clinical Characteristics and Prognosis of Polymyositis and Dermatomyositis Associated With Malignancy - A 25 Year Retrospective StudyDocument7 pages1908 Clinical Characteristics and Prognosis of Polymyositis and Dermatomyositis Associated With Malignancy - A 25 Year Retrospective StudyFlorian LamblinNo ratings yet
- Risk Factors For Drug-Resistant Tuberculosis: Marta Gomes, Ana Correia, Denisa Mendonça, Raquel DuarteDocument9 pagesRisk Factors For Drug-Resistant Tuberculosis: Marta Gomes, Ana Correia, Denisa Mendonça, Raquel DuarteAuliadi AnsharNo ratings yet
- Age As A Risk Factor of Relapse Occurrence in Acute Lymphoblastic Leukemia-L1 (All-L1) in ChildrenDocument4 pagesAge As A Risk Factor of Relapse Occurrence in Acute Lymphoblastic Leukemia-L1 (All-L1) in ChildrenYuliana WiralestariNo ratings yet
- Survival Analysis of Adult Tuberculosis Disease: Olurotimi Bankole Ajagbe, Zubair Kabair, Terry O'ConnorDocument10 pagesSurvival Analysis of Adult Tuberculosis Disease: Olurotimi Bankole Ajagbe, Zubair Kabair, Terry O'ConnorGetachew GemedaNo ratings yet
- Predicting Benign Course and Prolonged Illness in Lower Respiratory Tract Infections: A 13 European Country StudyDocument8 pagesPredicting Benign Course and Prolonged Illness in Lower Respiratory Tract Infections: A 13 European Country Studypanji satryo utomoNo ratings yet
- Jurnal Ria OctoberDocument9 pagesJurnal Ria Octoberria rochmanNo ratings yet
- 3.4 Cross-Sectional StudiesDocument4 pages3.4 Cross-Sectional StudiesRicardo Gomes100% (1)
- Nutritional Status As Cancer Diagnosis PredictorDocument13 pagesNutritional Status As Cancer Diagnosis Predictornutri.analuxavierNo ratings yet
- Guía Trisomía 13Document7 pagesGuía Trisomía 13Galy Crt FlzNo ratings yet
- A Geroscience Perspective On Immune Resilience and Infectious Diseases - A Potential Case For MetforminDocument20 pagesA Geroscience Perspective On Immune Resilience and Infectious Diseases - A Potential Case For MetforminAna Raquel Realista Coelho Dos Santos PedrosaNo ratings yet
- Frequency (Last Year)Document12 pagesFrequency (Last Year)Jehad Ali Al-ammariNo ratings yet
- CAP - PrinaDocument12 pagesCAP - PrinaSalNo ratings yet
- RF RHDDocument3 pagesRF RHDAl- Mondjid LeeNo ratings yet
- Jurnal Perawatan PaliatifDocument16 pagesJurnal Perawatan Paliatifnurwanda hamidaNo ratings yet
- Risk Factors For Extra-Pulmonary Tuberculosis Compared To Pulmonary TuberculosisDocument6 pagesRisk Factors For Extra-Pulmonary Tuberculosis Compared To Pulmonary TuberculosisLily SmithNo ratings yet
- Rheumatology 2008Document3 pagesRheumatology 2008Thelma Cantillo RochaNo ratings yet
- Healthmed 15 1 Damir SecicDocument6 pagesHealthmed 15 1 Damir SecicEdoHNo ratings yet
- DM and TB Abstract.Document17 pagesDM and TB Abstract.Anal PatelNo ratings yet
- Pa Nag Iot Akos 2015Document7 pagesPa Nag Iot Akos 2015Gabriel ParizotoNo ratings yet
- Corticoid-Associated Complications in Elderly: (V1 Ref Status: Not Approved 2, Http://F1000R.Es/Ulnz5M)Document9 pagesCorticoid-Associated Complications in Elderly: (V1 Ref Status: Not Approved 2, Http://F1000R.Es/Ulnz5M)Miranti Dea DoraNo ratings yet
- Risk Factors Associated With Diabetic Retinopathy in Patients With Diabetes Mellitus Type 2Document4 pagesRisk Factors Associated With Diabetic Retinopathy in Patients With Diabetes Mellitus Type 2Trx AntraxNo ratings yet
- Ice Berg Phenomenon of DiseaseDocument50 pagesIce Berg Phenomenon of DiseaseMan BoruahNo ratings yet
- Guia Wao Anafilaxia 2015Document16 pagesGuia Wao Anafilaxia 2015Diego Alexander ChingoNo ratings yet
- Association Between Diabetes Mellitus and TBDocument15 pagesAssociation Between Diabetes Mellitus and TBMade NujitaNo ratings yet
- AJRM MARCH PP 5-7Document3 pagesAJRM MARCH PP 5-7Vito Sahala TobiasNo ratings yet
- Quality of Life of Elderly With Chronic Liver DiseasesDocument7 pagesQuality of Life of Elderly With Chronic Liver DiseasesIOSRjournalNo ratings yet
- Depression and Hopelessness in Patients With Acute LeukemiaDocument11 pagesDepression and Hopelessness in Patients With Acute LeukemiaPedro CampinaNo ratings yet
- Delirium in The Intensive Care Unit: ReviewDocument9 pagesDelirium in The Intensive Care Unit: ReviewCristopher Castro RdNo ratings yet
- 236 468 1 SMDocument17 pages236 468 1 SMAldilla HennyNo ratings yet
- Research Article: Comorbidities of Idiopathic Thrombocytopenic Purpura: A Population-Based StudyDocument13 pagesResearch Article: Comorbidities of Idiopathic Thrombocytopenic Purpura: A Population-Based StudyAns FitriNo ratings yet
- Epidemiology ReviewDocument10 pagesEpidemiology ReviewSaurabhNo ratings yet
- Geriatric Assessment and Prognostic Factors of Mortality in Very Elderly Patients With Community-Acquired PneumoniaDocument18 pagesGeriatric Assessment and Prognostic Factors of Mortality in Very Elderly Patients With Community-Acquired PneumoniaAlya Arakai100% (1)
- SLE DR - Nita Uul PunyaDocument18 pagesSLE DR - Nita Uul PunyaduratulkhNo ratings yet
- Crohn ReviewDocument39 pagesCrohn Reviewdrkoral751No ratings yet
- Coping With Chronic Illness Childhood AdolescenceDocument27 pagesCoping With Chronic Illness Childhood AdolescenceLouisette AgapeNo ratings yet
- Gorantla Synthesis PaperDocument25 pagesGorantla Synthesis Paperapi-464986748No ratings yet
- Respiratory Tract Virus Infections in The Elderly With PneumoniaDocument11 pagesRespiratory Tract Virus Infections in The Elderly With PneumoniatanyasisNo ratings yet
- Type Diabetes and Multiple Myeloma The Latest Insights 2329 6917.1000e110Document2 pagesType Diabetes and Multiple Myeloma The Latest Insights 2329 6917.1000e110Akreditasi InternaNo ratings yet
- Kead 582Document2 pagesKead 582Alberto Sifuentes GiraldoNo ratings yet
- Tuberculosis Treatment Outcome Monitoring in England, Wales and Northern Ireland For Cases Reported in 2001Document6 pagesTuberculosis Treatment Outcome Monitoring in England, Wales and Northern Ireland For Cases Reported in 2001A KusyairiNo ratings yet
- Case Analysis - RRLDocument8 pagesCase Analysis - RRLAila HinlogNo ratings yet
- Criterios EULAR-ACR de AR 2010 PDFDocument11 pagesCriterios EULAR-ACR de AR 2010 PDFMORADOMIANo ratings yet
- Tuberculosis and Diabetes Mellitus - An Underappreciated AssociationDocument9 pagesTuberculosis and Diabetes Mellitus - An Underappreciated AssociationNajla rayNo ratings yet
- Novel Therapies For Older Adults With Acute Lymphoblastic LeukemiaDocument9 pagesNovel Therapies For Older Adults With Acute Lymphoblastic LeukemiaKarol CriscuoloNo ratings yet
- Metabolic Syndrome and Risk For Incident Alzheimer's Disease or Vascular DementiaDocument6 pagesMetabolic Syndrome and Risk For Incident Alzheimer's Disease or Vascular DementiaadriricaldeNo ratings yet
- FRAMMINGHAM1605794700Characterization of Cardiovascular Risk Factors and Framingham Score in An HIV 1 Population-1Document4 pagesFRAMMINGHAM1605794700Characterization of Cardiovascular Risk Factors and Framingham Score in An HIV 1 Population-1Asry AinunNo ratings yet
- Geriatrics: Acute Appendicitis in The Elderly: A Literature Review On An Increasingly Frequent Surgical ProblemDocument8 pagesGeriatrics: Acute Appendicitis in The Elderly: A Literature Review On An Increasingly Frequent Surgical ProblemCRISTHIAN CASTILLO JIBAJANo ratings yet
- Nou 297Document5 pagesNou 297ObamaNo ratings yet
- GuiasddddDocument10 pagesGuiasddddKarla CastilloNo ratings yet
- Guidelines For Prevention of NSAID-Related Ulcer ComplicationsDocument11 pagesGuidelines For Prevention of NSAID-Related Ulcer ComplicationsPeet UpNo ratings yet
- Clinical Profile and Outcome of Myasthenic CrisisDocument13 pagesClinical Profile and Outcome of Myasthenic CrisissyahriniNo ratings yet
- J Neurol Neurosurg Psychiatry 2016 Dlouhy 402 13Document13 pagesJ Neurol Neurosurg Psychiatry 2016 Dlouhy 402 13pebinscribdNo ratings yet
- Geriatric Assessment and Prognostic Factors of Mortality in Very Elderly Patients With Community-Acquired PneumoniaDocument18 pagesGeriatric Assessment and Prognostic Factors of Mortality in Very Elderly Patients With Community-Acquired PneumoniaAlya ArakaiNo ratings yet
- Telemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.From EverandTelemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.No ratings yet
- 4 Reasons Why Highly Intelligent People Are Happier With Less Socialization - Learning MindDocument12 pages4 Reasons Why Highly Intelligent People Are Happier With Less Socialization - Learning MindvishnupgiNo ratings yet
- 811 FullDocument11 pages811 FullvishnupgiNo ratings yet
- IndiaPOS PT2622 - User Manual-V1.651Document96 pagesIndiaPOS PT2622 - User Manual-V1.651vishnupgiNo ratings yet
- 1161 FullDocument9 pages1161 FullvishnupgiNo ratings yet
- Chikungunya Final Draft 16052017finalDocument24 pagesChikungunya Final Draft 16052017finalvishnupgiNo ratings yet
- Neprilysn InhibitorsDocument9 pagesNeprilysn InhibitorsvishnupgiNo ratings yet
- 0239Document7 pages0239vishnupgiNo ratings yet
- ICMR Guideline On Celiac Disease-Dec 2016Document62 pagesICMR Guideline On Celiac Disease-Dec 2016vishnupgi100% (2)
- Acquired Hemophilia A Presenting in An Elderly Man: Teaching Case ReportDocument2 pagesAcquired Hemophilia A Presenting in An Elderly Man: Teaching Case ReportvishnupgiNo ratings yet
- Journal of Autoimmune DiseasesDocument7 pagesJournal of Autoimmune DiseasesvishnupgiNo ratings yet
- Review Article: Pathogenic and Epiphenomenal Anti-DNA Antibodies in SLEDocument18 pagesReview Article: Pathogenic and Epiphenomenal Anti-DNA Antibodies in SLEvishnupgiNo ratings yet
- Sjogren 2012 NewDocument18 pagesSjogren 2012 NewvishnupgiNo ratings yet
- IRACON 2011 Highlights - FlyerDocument6 pagesIRACON 2011 Highlights - FlyervishnupgiNo ratings yet
- 44 - 75 - Detection of Autoantibodies Against Platelet Glycoproteins in ... HeDocument21 pages44 - 75 - Detection of Autoantibodies Against Platelet Glycoproteins in ... HevishnupgiNo ratings yet
- A Rose Is A Rose Is A Rose But CVID Is Not CVID - Common Variable Immune Deficiency (CVID) What Do We Know in 2011Document61 pagesA Rose Is A Rose Is A Rose But CVID Is Not CVID - Common Variable Immune Deficiency (CVID) What Do We Know in 2011vishnupgiNo ratings yet
- Thrombotic Thrombocytpenic Purpura - Lupus - Microangiopathic Hemolytic Anemia - PlasmapheresisDocument30 pagesThrombotic Thrombocytpenic Purpura - Lupus - Microangiopathic Hemolytic Anemia - PlasmapheresisvishnupgiNo ratings yet
- Mga Bilang 1-100 Tagalog With Symbol and PronunciationDocument2 pagesMga Bilang 1-100 Tagalog With Symbol and PronunciationJanice Tañedo PancipaneNo ratings yet
- Vocabulary & Grammar Test Unit 6 Test ADocument4 pagesVocabulary & Grammar Test Unit 6 Test AStjepan RasicNo ratings yet
- PARAM Shavak: High Performance Computing (HPC), Grid and Cloud ComputingDocument3 pagesPARAM Shavak: High Performance Computing (HPC), Grid and Cloud ComputingarchikakatiyarNo ratings yet
- Semantics. Abnormality in Syntagmatic Relations. 3 December 2020Document21 pagesSemantics. Abnormality in Syntagmatic Relations. 3 December 2020Marina TanovićNo ratings yet
- Chapter 2 PolynomialsDocument39 pagesChapter 2 PolynomialsRamesh RathoreNo ratings yet
- CH 20 - Program Design and Technique For Aerobic Endurance TrainingDocument20 pagesCH 20 - Program Design and Technique For Aerobic Endurance TrainingMarco RodriguezNo ratings yet
- FBS IntroductionDocument50 pagesFBS IntroductionPerly Algabre PantojanNo ratings yet
- Glued On Gadget Buttons: Digital Distraction and Learning MotivationDocument16 pagesGlued On Gadget Buttons: Digital Distraction and Learning MotivationPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Province Tourist Destinations Festivals: REGION XI - Davao RegionDocument13 pagesProvince Tourist Destinations Festivals: REGION XI - Davao Regionaaron manaogNo ratings yet
- EDI Application in Various FieldsDocument7 pagesEDI Application in Various Fieldsonlinep410No ratings yet
- Threading (Manufacturing) : Threading Is The Process of Creating ADocument16 pagesThreading (Manufacturing) : Threading Is The Process of Creating AAnonymous mRCnYKz7xBNo ratings yet
- FIN-01. Purchasing ProcedureDocument7 pagesFIN-01. Purchasing ProcedureVu Dinh ThietNo ratings yet
- ThorDocument5 pagesThorandreea uNo ratings yet
- Bilkis Bano Case NotesDocument2 pagesBilkis Bano Case NotesGia MaheshNo ratings yet
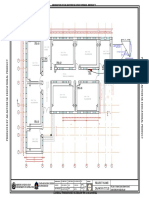
- Electrical of 6 Class Room .Dwg-POWDocument1 pageElectrical of 6 Class Room .Dwg-POWSayed WafiNo ratings yet
- Colour Magazine - London 1Document103 pagesColour Magazine - London 1iccang arsenal100% (1)
- Surveying For Highways: Eng. Suneth Thushara Highwy Design Division RDADocument31 pagesSurveying For Highways: Eng. Suneth Thushara Highwy Design Division RDAzeshan habibNo ratings yet
- Gabion Wall at IntakeDocument13 pagesGabion Wall at IntakeBert EngNo ratings yet
- School Action Plan in NDEP 2019 2020Document1 pageSchool Action Plan in NDEP 2019 2020CHAPEL JUN PACIENTENo ratings yet
- Falta DatabaseDocument72 pagesFalta DatabaseTENDER AWADH GROUPNo ratings yet
- Government of Kerala: Nursery Teachers Education Course Examination MARCH 2013Document11 pagesGovernment of Kerala: Nursery Teachers Education Course Examination MARCH 2013edujobnewsNo ratings yet
- Give The Lord Glory and Honor (Psalm 96)Document1 pageGive The Lord Glory and Honor (Psalm 96)Lionel Valdellon100% (1)
- Application of Value Analysis and Value Engineering For Cost Reduction of Global Pumping UnitDocument8 pagesApplication of Value Analysis and Value Engineering For Cost Reduction of Global Pumping UnitVINOD PAKHARENo ratings yet
- TM 5-277 Fixed Steel Panel Bridge Bailey TypeDocument121 pagesTM 5-277 Fixed Steel Panel Bridge Bailey TypeAdvocate100% (2)
- Dhan Allyn Romero 11 Saturn ABM EAPPDocument7 pagesDhan Allyn Romero 11 Saturn ABM EAPPJhevie RanileNo ratings yet
- ICTDocument4 pagesICTqwertyNo ratings yet
- Nanofiltration of Textile Plant Effluent For Color Removal and Reduction in CODDocument11 pagesNanofiltration of Textile Plant Effluent For Color Removal and Reduction in CODOmaya TariqNo ratings yet
- Assignment 2 MGT501Document1 pageAssignment 2 MGT501Aamir ShahzadNo ratings yet
- Amazon.com_ New Precision 5540 Mobile Workstation Laptop 9th Gen i9-9880H, 8 Core up to 4.80GHz vPro 1TB SSD 64GB Ram Nvidia Quadro P2000 4GB 15.6_ 4K UHD 3840x2160, Touch Display Win 10 Pro_ Computers & AccessoriesDocument12 pagesAmazon.com_ New Precision 5540 Mobile Workstation Laptop 9th Gen i9-9880H, 8 Core up to 4.80GHz vPro 1TB SSD 64GB Ram Nvidia Quadro P2000 4GB 15.6_ 4K UHD 3840x2160, Touch Display Win 10 Pro_ Computers & AccessoriesBirungi NelsonNo ratings yet