Download as pdf or txt
You might also like
- Therapeutic EquivalenceDocument2 pagesTherapeutic EquivalenceyuppierajNo ratings yet
- BiopharmaceuticsDocument21 pagesBiopharmaceuticsSilvy100% (1)
- AHCC: The Medical Breakthrough in Natural ImmunotherapyFrom EverandAHCC: The Medical Breakthrough in Natural ImmunotherapyRating: 5 out of 5 stars5/5 (1)
- 2016 New Medicare Shared Savings Pogram ACOsDocument19 pages2016 New Medicare Shared Savings Pogram ACOsiggybauNo ratings yet
- Nursing Review Exam Questions FUNDADocument10 pagesNursing Review Exam Questions FUNDAAlibasher MacalnasNo ratings yet
- Definition of BiopharmaceuticsDocument3 pagesDefinition of BiopharmaceuticsvafaashkNo ratings yet
- What Is Biopharmaceutics?: Brand NameDocument10 pagesWhat Is Biopharmaceutics?: Brand NameAhmad Jamal HashmiNo ratings yet
- Bio Availability and Bioequivalane-LastDocument13 pagesBio Availability and Bioequivalane-LastAhmedothman62100% (1)
- Therapeutic EquivalenceDocument2 pagesTherapeutic EquivalenceAngel De la VictoriaNo ratings yet
- Final ProjectDocument119 pagesFinal ProjectSaurabh KumarNo ratings yet
- Ch-3 Bioavailability of Drugs and Bioequivalence-18th BatchDocument30 pagesCh-3 Bioavailability of Drugs and Bioequivalence-18th BatchFerdous Shahriar100% (1)
- Review Article: Barbara Davit, April C. Braddy, Dale P. Conner, and Lawrence X. YuDocument17 pagesReview Article: Barbara Davit, April C. Braddy, Dale P. Conner, and Lawrence X. Yulhthang1990No ratings yet
- Bioequivalence: Faculty of Pharmacy, Nursing and Health Professions Master in Industrial Pharmaceutical TechnologyDocument15 pagesBioequivalence: Faculty of Pharmacy, Nursing and Health Professions Master in Industrial Pharmaceutical TechnologyMayson Bali100% (1)
- Biopharmaceutics: Definitions and TerminologiesDocument30 pagesBiopharmaceutics: Definitions and TerminologiesDanish KamalNo ratings yet
- Thailand BABE GuidelineDocument27 pagesThailand BABE GuidelineDianeNo ratings yet
- Guideline On Bioavailability and BioequivalanceDocument26 pagesGuideline On Bioavailability and BioequivalanceGima Amezia SariNo ratings yet
- Bioequivalence: Faculty of Pharmacy, Nursing and Health Professions Master in Industrial Pharmaceutical TechnologyDocument16 pagesBioequivalence: Faculty of Pharmacy, Nursing and Health Professions Master in Industrial Pharmaceutical TechnologyMayson BaliNo ratings yet
- Bioavailability and BioequivalenceDocument6 pagesBioavailability and BioequivalenceDharmesh PatelNo ratings yet
- Biological Aspects of FormulationsDocument8 pagesBiological Aspects of FormulationsKabirNo ratings yet
- Hemanagadurga2019 Bioavailability StudiesDocument17 pagesHemanagadurga2019 Bioavailability Studiesraghuraj75No ratings yet
- Bioavailability and BioequivalenceDocument47 pagesBioavailability and BioequivalenceGiovanne Buendia100% (1)
- ASEAN BE Guidelines-Amended According To1st BABE TWG15th PPWGDocument29 pagesASEAN BE Guidelines-Amended According To1st BABE TWG15th PPWGTarikNo ratings yet
- Asean Guidelines For: Final Draft: 21 July 2004Document29 pagesAsean Guidelines For: Final Draft: 21 July 2004Jone YingNo ratings yet
- Bioavailability and BioequivalenceDocument53 pagesBioavailability and BioequivalenceWalaa abo foolNo ratings yet
- Bioavailability and Bioequivalence - 2 - Types, Methods, ProtocolDocument36 pagesBioavailability and Bioequivalence - 2 - Types, Methods, Protocolwovefiv466No ratings yet
- Bioequevalance StudiesDocument55 pagesBioequevalance StudiesMubammad MursaleenNo ratings yet
- 8 Ba Be FdaDocument36 pages8 Ba Be Fdaraju narayana padalaNo ratings yet
- Ba-Be PDFDocument30 pagesBa-Be PDFUswatun Hasanah7201No ratings yet
- Bioavailability and Bioequivalence (BABE)Document4 pagesBioavailability and Bioequivalence (BABE)Wingielyn Honculada BaldozaNo ratings yet
- Bioavailability and BioequivalenceDocument56 pagesBioavailability and Bioequivalenceنور الهدى100% (1)
- Bioavailability and Bieq Review ArticleDocument15 pagesBioavailability and Bieq Review ArticlevinayNo ratings yet
- IntroductionDocument71 pagesIntroductionAreenub ArshadNo ratings yet
- 24 13v3i2 5Document9 pages24 13v3i2 5gopalNo ratings yet
- Usp 1151Document10 pagesUsp 1151Karnati PraveenaNo ratings yet
- Bioavailability and BioequivalenceDocument28 pagesBioavailability and Bioequivalencekulbhushan singhNo ratings yet
- Difference Between Bioavailability and BioequivalenceDocument11 pagesDifference Between Bioavailability and Bioequivalenceprakash deshmukhNo ratings yet
- Comparing Generic and Innovator Drugs A Review ofDocument16 pagesComparing Generic and Innovator Drugs A Review ofPrachi PandeyNo ratings yet
- Biopharmaceutics & Pharmacokinetics: 4 ProfessionalDocument163 pagesBiopharmaceutics & Pharmacokinetics: 4 ProfessionalChristianNo ratings yet
- Psychotropic DrugDocument10 pagesPsychotropic DrugAlexandra Elizabeth FloresNo ratings yet
- Bioequivalence StudiesDocument19 pagesBioequivalence StudiesYaqeen Mutan100% (1)
- Bioanalysis NotesDocument7 pagesBioanalysis NoteskeerthiNo ratings yet
- Article On BA&BEDocument7 pagesArticle On BA&BENitin DhimanNo ratings yet
- Note For Guidance On The Investigation of Bioavailability & BioequivalenceDocument19 pagesNote For Guidance On The Investigation of Bioavailability & BioequivalenceAhmed AliNo ratings yet
- Ad. BPPK 16Document119 pagesAd. BPPK 16Sachin BagewadiNo ratings yet
- Bioavailability and Bioequivalence - IntroductionDocument11 pagesBioavailability and Bioequivalence - Introductionwovefiv466No ratings yet
- Bioavailability and Bioequivalence StudiesDocument49 pagesBioavailability and Bioequivalence StudiesvarishNo ratings yet
- Formulary 2009Document51 pagesFormulary 2009Wen ZhuNo ratings yet
- Non Linear PharmacokineticsDocument33 pagesNon Linear PharmacokineticsClaudNo ratings yet
- Bioavailability and BioequivalenceDocument81 pagesBioavailability and BioequivalenceNiharika ModiNo ratings yet
- Daniel Wood Christopher Gregory: Understanding GenericsDocument9 pagesDaniel Wood Christopher Gregory: Understanding Genericsniravpharma21No ratings yet
- تصميم كويزDocument73 pagesتصميم كويزHemo HindiNo ratings yet
- Clinical Pharmacology Answers 2022Document223 pagesClinical Pharmacology Answers 2022nancy voraNo ratings yet
- 20220720 FDA治疗等效性评估【中英对照】Document20 pages20220720 FDA治疗等效性评估【中英对照】lewis liNo ratings yet
- Guideline For Bioequivalence Studies of Generic ProductsDocument23 pagesGuideline For Bioequivalence Studies of Generic ProductschetanjmistryNo ratings yet
- Drug Absorption PDFDocument117 pagesDrug Absorption PDFAndhia DhiyaNo ratings yet
- Pkin08 Soal Biofar Pak BoesroDocument117 pagesPkin08 Soal Biofar Pak Boesroabu_59No ratings yet
- Guidelines For Bioavailability and Bioequivalence Studies: A ReviewDocument6 pagesGuidelines For Bioavailability and Bioequivalence Studies: A ReviewNagabhushanam MaddiNo ratings yet
- Bioavailability: by Abera JDocument59 pagesBioavailability: by Abera JAbera JamboNo ratings yet
- BIOEQUI2Document5 pagesBIOEQUI2Laiba KhalidNo ratings yet
- Drug Delivery Inhalation BioequivalenceDocument12 pagesDrug Delivery Inhalation Bioequivalenceparinaferns0% (1)
- Introduction and Overview: ObjectivesDocument17 pagesIntroduction and Overview: Objectivesandreani temeNo ratings yet
- Competency Assessment QuestionnaireDocument2 pagesCompetency Assessment QuestionnairekurutalaNo ratings yet
- Names To Be Deleted From TracerDocument2 pagesNames To Be Deleted From TracerkurutalaNo ratings yet
- CBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnanDocument2 pagesCBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnankurutalaNo ratings yet
- AnnouncementDocument1 pageAnnouncementkurutalaNo ratings yet
- TOUCH Untrained Status (January 2014)Document2 pagesTOUCH Untrained Status (January 2014)kurutalaNo ratings yet
- DRIVE PROGRAM (2013 - 2014) : Total Total Total TotalDocument1 pageDRIVE PROGRAM (2013 - 2014) : Total Total Total TotalkurutalaNo ratings yet
- Program Name Division Name Date Duration of Days TimeDocument2 pagesProgram Name Division Name Date Duration of Days TimekurutalaNo ratings yet
- La Shield DetailingDocument2 pagesLa Shield DetailingkurutalaNo ratings yet
- SR No Division Brand: Division Wise Brands For Interview PanelDocument1 pageSR No Division Brand: Division Wise Brands For Interview PanelkurutalaNo ratings yet
- Ascoril Expectorant - Detailing Story InterviewsDocument2 pagesAscoril Expectorant - Detailing Story InterviewskurutalaNo ratings yet
- Healtheon DetailingDocument1 pageHealtheon DetailingkurutalaNo ratings yet
- Esoz - Detailing TalkDocument2 pagesEsoz - Detailing TalkkurutalaNo ratings yet
- Critica VAF Detailing TalkDocument1 pageCritica VAF Detailing TalkkurutalaNo ratings yet
- Glenmark CV DetailingDocument1 pageGlenmark CV DetailingkurutalaNo ratings yet
- CTV DetailingDocument1 pageCTV DetailingkurutalaNo ratings yet
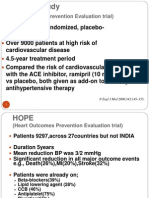
- The HOPE Study: (Heart Outcomes Prevention Evaluation Trial)Document4 pagesThe HOPE Study: (Heart Outcomes Prevention Evaluation Trial)kurutalaNo ratings yet
- 08 Drug ProfileDocument2 pages08 Drug ProfilekurutalaNo ratings yet
- Activity Report & Monthly Planner - Training Manager - April MayDocument4 pagesActivity Report & Monthly Planner - Training Manager - April MaykurutalaNo ratings yet
- Yearly Calender CDG ' 12-13 FinalDocument6 pagesYearly Calender CDG ' 12-13 FinalkurutalaNo ratings yet
- Activity Report & Monthly Planner - Training Manager - AUGUST'12Document4 pagesActivity Report & Monthly Planner - Training Manager - AUGUST'12kurutalaNo ratings yet
- Name of Employee Date of Birth (DD-MM-Yyyy) Contact NumberDocument3 pagesName of Employee Date of Birth (DD-MM-Yyyy) Contact NumberkurutalaNo ratings yet
- Surgical Skin Prep and DrapingDocument30 pagesSurgical Skin Prep and DrapingshyluckmayddpNo ratings yet
- UntitledDocument1 pageUntitledapi-77569240No ratings yet
- Skill Hebefrenic SchizophreniaDocument13 pagesSkill Hebefrenic SchizophreniasaidahrahmatNo ratings yet
- Tinnitus Today June 1989 Vol 14, No 2Document20 pagesTinnitus Today June 1989 Vol 14, No 2American Tinnitus AssociationNo ratings yet
- The Bedside Oral Exam and The Barrow Oral Care ProtocolDocument2 pagesThe Bedside Oral Exam and The Barrow Oral Care ProtocolKarla Katrina CajigalNo ratings yet
- Risk Indicators and Interceptive Treatment Alternatives For Palatally Displaced Canines2010 - 16 - 3 - 186 - 192Document7 pagesRisk Indicators and Interceptive Treatment Alternatives For Palatally Displaced Canines2010 - 16 - 3 - 186 - 192griffone1No ratings yet
- Dialysis ParametersDocument153 pagesDialysis ParametersLungu Adi100% (1)
- Tips From A PD - 2015 Usmle Residency MatchDocument5 pagesTips From A PD - 2015 Usmle Residency MatchPsihoterapija50% (2)
- Fetal DistressDocument32 pagesFetal DistressMadhu Sudhan PandeyaNo ratings yet
- Johnson TheoryDocument57 pagesJohnson TheorySamer H AL-shabatat100% (3)
- Fixation Methods in OrthopaedicsDocument40 pagesFixation Methods in OrthopaedicsBhaskar BorgohainNo ratings yet
- Ventilator PortableDocument1 pageVentilator PortableAamer MumtazNo ratings yet
- Philippine Nursing Seminars and Training November 2010Document5 pagesPhilippine Nursing Seminars and Training November 2010PhilippineNursingDirectory.comNo ratings yet
- Appa Et1Document4 pagesAppa Et1Maria Theresa Deluna MacairanNo ratings yet
- Sample Article in Outpatient DepartmentDocument2 pagesSample Article in Outpatient DepartmentRodney Beltran SubaranNo ratings yet
- Causes of Balance Problems After Stroke: Weakness. Most Stroke Patients Feel Some Kind of WeaknessDocument24 pagesCauses of Balance Problems After Stroke: Weakness. Most Stroke Patients Feel Some Kind of WeaknessSienna JuradoNo ratings yet
- Oakstone Complete ListDocument3 pagesOakstone Complete ListMalone0% (2)
- Mental Health Care Bill 2013Document53 pagesMental Health Care Bill 2013Ankit GuptaNo ratings yet
- Livability Prattville, AL: 2013Document50 pagesLivability Prattville, AL: 2013Journal CommunicationsNo ratings yet
- Patient Transfusion Testing IndustryDocument9 pagesPatient Transfusion Testing IndustryRasagna RajNo ratings yet
- Association of Voiding Dysfunction With Functional ConstipationDocument3 pagesAssociation of Voiding Dysfunction With Functional ConstipationSisca Dwi AgustinaNo ratings yet
- Diagnosis and Treatment of Submucous Myoma of TheDocument18 pagesDiagnosis and Treatment of Submucous Myoma of TheagungratihsdNo ratings yet
- Oral Health Assessment Form For Children, 2013 Annex 2Document1 pageOral Health Assessment Form For Children, 2013 Annex 2naifaNo ratings yet
- Fracture+healing MmsDocument9 pagesFracture+healing MmsArchana MohantyNo ratings yet
- Diabetic Diet: From Wikipedia, The Free EncyclopediaDocument6 pagesDiabetic Diet: From Wikipedia, The Free EncyclopediaMeta BachtiarNo ratings yet
- Care For Mechanical VentilationDocument14 pagesCare For Mechanical Ventilationmaeya186135100% (3)
- Dr. Mohamed Mosaad Hasan MD, MPH, CPHQ, CPPS, GbssDocument48 pagesDr. Mohamed Mosaad Hasan MD, MPH, CPHQ, CPPS, GbssKristine Marie PateñoNo ratings yet
- Alginate Impression MakingDocument28 pagesAlginate Impression MakingBharanijaNo ratings yet