Download as doc, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Macroeconomics Canadian 5th Edition Mankiw Solutions ManualDocument25 pagesMacroeconomics Canadian 5th Edition Mankiw Solutions ManualMrJosephCruzMDfojy100% (54)
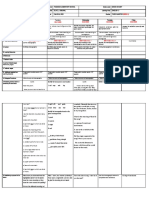
- DLL ENGLISH 3 WEEK 2 Q3 HomographsDocument7 pagesDLL ENGLISH 3 WEEK 2 Q3 HomographsOlive L. Gabunal100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- SWX315 Commander - Shuttlewagon Mobile Railcar MoversDocument54 pagesSWX315 Commander - Shuttlewagon Mobile Railcar MoversJesús Palomares100% (1)
- Prepositions of Place-WorksheetDocument2 pagesPrepositions of Place-Worksheetteresabarbosa94% (104)
- College Pretest PE 1Document7 pagesCollege Pretest PE 1Jelyn Racel Agundo ElmedulanNo ratings yet
- Okonkwo's Suicide: The Aftermath of An Existential CrisisDocument13 pagesOkonkwo's Suicide: The Aftermath of An Existential CrisisRavina ParmarNo ratings yet
- Sailor Moon Amigurumi: By: Bellis1282 On Ravelry: Email: Bellis1282@Document10 pagesSailor Moon Amigurumi: By: Bellis1282 On Ravelry: Email: Bellis1282@Esmeralda ValeraNo ratings yet
- Rephrasing On Tenses PDFDocument1 pageRephrasing On Tenses PDFEsmeralda ValeraNo ratings yet
- ExamDocument3 pagesExamEsmeralda ValeraNo ratings yet
- Submarines Nonfiction Reading Test 1Document3 pagesSubmarines Nonfiction Reading Test 1Esmeralda ValeraNo ratings yet
- Zero Acceptance Number Sampling Plan 57 372 DemoDocument5 pagesZero Acceptance Number Sampling Plan 57 372 DemoBALAJINo ratings yet
- Audit UNIT 4Document14 pagesAudit UNIT 4Nigussie BerhanuNo ratings yet
- New TIP Course 1 DepEd Teacher PDFDocument89 pagesNew TIP Course 1 DepEd Teacher PDFLenie TejadaNo ratings yet
- Des-F1025p-E DSDocument3 pagesDes-F1025p-E DSNaing Win ZawNo ratings yet
- S3F94xx BatteryCharger An REV000 060109-0Document40 pagesS3F94xx BatteryCharger An REV000 060109-0Jack ChanNo ratings yet
- Lesson 1 - Traditions and Locations - The Filipino PoemDocument8 pagesLesson 1 - Traditions and Locations - The Filipino Poemdes oro100% (1)
- Journaling PDFDocument1 pageJournaling PDFMargarita Maria Botero PerezNo ratings yet
- Sample Follow-Up LettersDocument2 pagesSample Follow-Up LettersMhira AlmeroNo ratings yet
- Chartplotter Compatibility Guide: Products Content and FeaturesDocument2 pagesChartplotter Compatibility Guide: Products Content and FeaturesRimantas VaiciusNo ratings yet
- Gas Bill AprilDocument4 pagesGas Bill AprilMozhie OicangiNo ratings yet
- NoN Covalente ForcesDocument528 pagesNoN Covalente ForcesLorena Monterrosas PérezNo ratings yet
- 2volt Powerstack BatteriesDocument4 pages2volt Powerstack BatteriesYasirNo ratings yet
- SSL Stripping Technique DHCP Snooping and ARP Spoofing InspectionDocument7 pagesSSL Stripping Technique DHCP Snooping and ARP Spoofing InspectionRMNo ratings yet
- Marinediesels - Co.uk - Members Section Starting and Reversing Sulzer ZA40 Air Start SystemDocument2 pagesMarinediesels - Co.uk - Members Section Starting and Reversing Sulzer ZA40 Air Start SystemArun SNo ratings yet
- Annotated BibliographyDocument2 pagesAnnotated Bibliographyapi-214882950No ratings yet
- Fire Safety - Wikipedia PDFDocument29 pagesFire Safety - Wikipedia PDFAld rich NuñezNo ratings yet
- Energy Statistics - Power Generation of IPGCL - PPCL: by - Aditi JainDocument16 pagesEnergy Statistics - Power Generation of IPGCL - PPCL: by - Aditi JainknochoutNo ratings yet
- Bba 820 - Managerial Functions - Blended ModuleDocument73 pagesBba 820 - Managerial Functions - Blended Modulemichael kimNo ratings yet
- Fatigue Crack Propagation in Aluminium AlloysDocument3 pagesFatigue Crack Propagation in Aluminium AlloysNils VerkleijNo ratings yet
- Is It Time For You To Say 'I Do' by Rommel N. AngaraDocument1 pageIs It Time For You To Say 'I Do' by Rommel N. AngaraWell-loved Essays100% (2)
- Ultrasound in Obstretics PDFDocument40 pagesUltrasound in Obstretics PDFcarcobe3436100% (1)
- VR-Research Paper: August 2021Document66 pagesVR-Research Paper: August 2021Shashank YadavNo ratings yet
- D C A B: Installation Electronic Vessel Control D4, D6 EVC - CDocument2 pagesD C A B: Installation Electronic Vessel Control D4, D6 EVC - Csivan_sg1800No ratings yet
- TS TR 0075 D PDFDocument2 pagesTS TR 0075 D PDFromanjcNo ratings yet
- Summary of VBA For Scientific Computing 9-25-2013 v1Document19 pagesSummary of VBA For Scientific Computing 9-25-2013 v1lionfierce123No ratings yet