Download as pdf or txt
You might also like
- Nephrology MCQ PDFDocument7 pagesNephrology MCQ PDFreenarachelgeorge100% (4)
- Concept Map - HyponatremiaDocument9 pagesConcept Map - HyponatremiaElleNo ratings yet
- Pediatrics in Review. Dehydration 2015Document14 pagesPediatrics in Review. Dehydration 2015Jorge Eduardo Espinoza Rios100% (2)
- Lab Monitoring For Common Medications: Pharmacist'S Letter / Prescriber'S LetterDocument22 pagesLab Monitoring For Common Medications: Pharmacist'S Letter / Prescriber'S Letterddandan_2No ratings yet
- Syndrome of Inappropriate Secretion of Anti Diuretic HormoneDocument39 pagesSyndrome of Inappropriate Secretion of Anti Diuretic Hormonefarmasi_hmNo ratings yet
- Lab Values: Interpreting Chemistry and Hematology For Adult PatientsDocument36 pagesLab Values: Interpreting Chemistry and Hematology For Adult PatientsBrian Johnson100% (1)
- Diarrhea in ChildrenDocument35 pagesDiarrhea in ChildrenNugrah Tri Amiranti100% (2)
- Diabetes InsipidusDocument4 pagesDiabetes Insipidusshelly_shellyNo ratings yet
- Diabetes InsipidusDocument5 pagesDiabetes InsipidusFazalJaturieNo ratings yet
- Electrolytes & FluidimbalancesDocument80 pagesElectrolytes & FluidimbalancesDennis Nyambane MomanyiNo ratings yet
- 10.1 Water IntoxicationDocument20 pages10.1 Water IntoxicationDareRaymond100% (2)
- Dan L Ellsbury, MD, FAAPDocument8 pagesDan L Ellsbury, MD, FAAPfaruuukNo ratings yet
- Hyperglycemic H-WPS OfficeDocument4 pagesHyperglycemic H-WPS OfficeShiehan Mae ForroNo ratings yet
- DehydrationDocument17 pagesDehydrationLaura Anghel-MocanuNo ratings yet
- KMB Diabetes InsipidusDocument24 pagesKMB Diabetes InsipidusNur Rofikoh Bil Karomah100% (1)
- Diagnosis of Polyuria and Diabetes Insipidus - UP To DATEDocument15 pagesDiagnosis of Polyuria and Diabetes Insipidus - UP To DATELuis Fernando Arias VillalobosNo ratings yet
- Case Report ..Document69 pagesCase Report ..sashadilanNo ratings yet
- Electrolyte CompleteDocument6 pagesElectrolyte CompleteTofan Ana100% (2)
- Fluid N Electrolyte BalanceDocument60 pagesFluid N Electrolyte BalanceAnusha Verghese67% (3)
- Dehydration: Paul R. EarlDocument26 pagesDehydration: Paul R. EarlAndreeaHumaNo ratings yet
- REVALIDADocument53 pagesREVALIDAMercy Anne EcatNo ratings yet
- REVALIDADocument53 pagesREVALIDAMercy Anne EcatNo ratings yet
- Fluid and Electrolyte BalanceDocument52 pagesFluid and Electrolyte BalanceFrancis Appau100% (1)
- Diabetes Case Study Fall 2016 1Document7 pagesDiabetes Case Study Fall 2016 1api-284823421No ratings yet
- 110-Dehydration and Disorders of Sodium BalanceDocument5 pages110-Dehydration and Disorders of Sodium BalancepelinNo ratings yet
- DeshidratacionDocument14 pagesDeshidratacionAlvaro Andres Flores JimenezNo ratings yet
- Medical Surgical Fluid and Electrolytes FVD FVEDocument7 pagesMedical Surgical Fluid and Electrolytes FVD FVEMichaelaKatrinaTrinidadNo ratings yet
- Lesson 4 - Electrolyte Imbalances Part 1Document74 pagesLesson 4 - Electrolyte Imbalances Part 1Clark SavageNo ratings yet
- Alteration in Fluid and Electrolyte ImbalanceDocument118 pagesAlteration in Fluid and Electrolyte ImbalanceRenuga SureshNo ratings yet
- Dehydration: Paul R. EarlDocument31 pagesDehydration: Paul R. EarlJaya Prabha100% (1)
- Electrolyte Imbalance: Sodium: Submitted By: Milosantos, John Francis D. Tuibeo, Ma. Arlyn P. Yu, Aldrin Anthony LDocument6 pagesElectrolyte Imbalance: Sodium: Submitted By: Milosantos, John Francis D. Tuibeo, Ma. Arlyn P. Yu, Aldrin Anthony Lnospekiko21No ratings yet
- Fluids and ElectrolytesDocument26 pagesFluids and ElectrolytesRahul K. JagaNo ratings yet
- Diabetes Insipidus: Done By: Farah Suhimat Sereen MajaliDocument23 pagesDiabetes Insipidus: Done By: Farah Suhimat Sereen Majaliraed faisalNo ratings yet
- Pediatrics in Review 2013 HiponatremiaDocument5 pagesPediatrics in Review 2013 HiponatremiaCarlos Elio Polo Vargas100% (1)
- DKADocument5 pagesDKAMariel BernabeNo ratings yet
- What's To Know About Diabetes Insipidus?: Last Updated Fri 19 January 2018 byDocument5 pagesWhat's To Know About Diabetes Insipidus?: Last Updated Fri 19 January 2018 byCindy Mae Flores UtlegNo ratings yet
- Dehydration Isonatremic, Hyponatremic, andDocument15 pagesDehydration Isonatremic, Hyponatremic, andalfredoibcNo ratings yet
- Diabetes Mellitus, Disorder Of: Institute For BiotechnologyDocument10 pagesDiabetes Mellitus, Disorder Of: Institute For BiotechnologyAndre Jonathan Siàńsàkà IINo ratings yet
- Paper ElektifDocument10 pagesPaper Elektifamyliadwi22No ratings yet
- Electrolytes Slide 21Document111 pagesElectrolytes Slide 21Elaisha Mae C. CarsulaNo ratings yet
- REVALIDADocument49 pagesREVALIDAMercy Anne EcatNo ratings yet
- Endocrine and MetabolicDocument30 pagesEndocrine and Metabolicjamaica faith ramonNo ratings yet
- Diabetes InsipidusDocument81 pagesDiabetes InsipidusMurugesh BabuNo ratings yet
- Diabetes and MassageDocument23 pagesDiabetes and MassagemassagekevinNo ratings yet
- Kedaruratan MetabolikDocument26 pagesKedaruratan MetabolikAstri Novia RizqiNo ratings yet
- Unit II Water and ElectrolytesDocument8 pagesUnit II Water and ElectrolytesSantosh P JosephNo ratings yet
- ToolDocument1 pageToolHakim RazalanNo ratings yet
- A Systematic Approach To The Hyponatremic Patient: Iva Ratkoviê-Gusiê, Petar Kes And Vanja Baπiê-KesDocument10 pagesA Systematic Approach To The Hyponatremic Patient: Iva Ratkoviê-Gusiê, Petar Kes And Vanja Baπiê-KesTio Prima SNo ratings yet
- Electrolyte DisordersDocument10 pagesElectrolyte DisordersSlavicaNo ratings yet
- Project 1Document26 pagesProject 1sanju ShreeNo ratings yet
- Case Study On DehydrationDocument4 pagesCase Study On DehydrationDustin Dela CruzNo ratings yet
- Case Study On Diabetes MellitusDocument12 pagesCase Study On Diabetes Mellitusferdz02No ratings yet
- There Are Two Main Types of GastritisDocument11 pagesThere Are Two Main Types of GastritisMike Faustino SolangonNo ratings yet
- Diabetes INSIPIDUSDocument6 pagesDiabetes INSIPIDUSavinash dhameriya100% (1)
- GROUP 4 - HyperglikemiDocument5 pagesGROUP 4 - Hyperglikemiamyliadwi22No ratings yet
- BIODocument3 pagesBIObisayushman2009No ratings yet
- What Are The Symptoms of Diabetes Insipidus?Document5 pagesWhat Are The Symptoms of Diabetes Insipidus?Lutfi AuliaNo ratings yet
- M5 - Electrolyte AbnormalitiesDocument44 pagesM5 - Electrolyte AbnormalitiesVishal KumarNo ratings yet
- Treatment of Hypernatremia in Adults - UpToDateDocument35 pagesTreatment of Hypernatremia in Adults - UpToDateJuLio Czar Carmona100% (1)
- Fluid Volume Deficit Nursing ManagementDocument5 pagesFluid Volume Deficit Nursing ManagementA.No ratings yet
- Diabetes InsipidusDocument14 pagesDiabetes InsipidusTom BiusoNo ratings yet
- Water MetabolismDocument13 pagesWater MetabolismarmyNo ratings yet
- Diabetes Insipidus HandoutDocument4 pagesDiabetes Insipidus HandoutllianNo ratings yet
- Hypernatremic DehydrationDocument17 pagesHypernatremic DehydrationMihraban OmerNo ratings yet
- Low Blood Sugar: The Nutritional Plan to Overcome Hypoglycaemia, with 60 RecipesFrom EverandLow Blood Sugar: The Nutritional Plan to Overcome Hypoglycaemia, with 60 RecipesNo ratings yet
- Algorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFDocument6 pagesAlgorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFFurqon AfandriNo ratings yet
- October Sodium DisordersDocument20 pagesOctober Sodium DisordersAngel GarciaNo ratings yet
- Etiology and Evaluation of Hypernatremia in Adults - UpToDateDocument26 pagesEtiology and Evaluation of Hypernatremia in Adults - UpToDateMihaela Alexandra RepeziNo ratings yet
- Mini RinDocument5 pagesMini Rinlovely_dyaNo ratings yet
- Acute GastroenteritisDocument51 pagesAcute GastroenteritisuouoNo ratings yet
- Case Study - Excretory System EssayDocument3 pagesCase Study - Excretory System EssayTatjana SaphiraNo ratings yet
- MCQs in Fluid and Electrolyte Balance With AnswersDocument50 pagesMCQs in Fluid and Electrolyte Balance With AnswersAbdulkadir Waliyy Musa100% (2)
- Racgp GuideDocument28 pagesRacgp Guidemyat252100% (1)
- Cerebral Salt Wasting SyndromeDocument6 pagesCerebral Salt Wasting SyndromeAbi ArifiNo ratings yet
- Electrolyte DisturbanceDocument21 pagesElectrolyte DisturbanceLuke TosingaNo ratings yet
- Diagnosis and Treatment of Hyponatremia .7Document10 pagesDiagnosis and Treatment of Hyponatremia .7Arista RachmaNo ratings yet
- Electrolytes & FluidimbalancesDocument80 pagesElectrolytes & FluidimbalancesDennis Nyambane MomanyiNo ratings yet
- M 2Document8 pagesM 2Aijem RyanNo ratings yet
- Fluid and ElectrolyteDocument46 pagesFluid and Electrolyteapi-76740522No ratings yet
- NUR 300 - Final Exam Study Guide - 2016Document548 pagesNUR 300 - Final Exam Study Guide - 2016MSU_nursing_4_lifeNo ratings yet
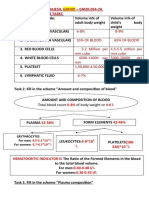
- Name - Soni Ritika Rajesh, Group - GM20-054-2A Physiology Week 03 TasksDocument10 pagesName - Soni Ritika Rajesh, Group - GM20-054-2A Physiology Week 03 TasksRitika SoniNo ratings yet
- AIS Sports NutritionDocument3 pagesAIS Sports NutritionArnel VillasinNo ratings yet
- Fluid Electrolytes Bablance 150308Document17 pagesFluid Electrolytes Bablance 150308Laura ReyesNo ratings yet
- Journal HyponatremiaDocument39 pagesJournal HyponatremiadharmaNo ratings yet
- Letters To The Editor: Misconceptions in The Treatment of Dehydration in ChildrenDocument5 pagesLetters To The Editor: Misconceptions in The Treatment of Dehydration in ChildrenViridiana VegaNo ratings yet
- Fluid GuidelinesDocument8 pagesFluid GuidelinesAya SalahNo ratings yet
- Postoperative Pituitary Management Ausiello 2008Document11 pagesPostoperative Pituitary Management Ausiello 2008api-229617613No ratings yet
- FLUID & Electrolyte ManagementDocument49 pagesFLUID & Electrolyte ManagementYovitaNo ratings yet
- Potassium Chloride Injection: Product MonographDocument18 pagesPotassium Chloride Injection: Product MonographMatthew ParsonsNo ratings yet
- Dr. Maulik Vaja Moderator: Dr. C. S. NAIDUDocument106 pagesDr. Maulik Vaja Moderator: Dr. C. S. NAIDUDilip Kumar MNo ratings yet