
Spatial Dose Mapping For Individualizing Radioiodine Treatment
Spatial Dose Mapping For Individualizing Radioiodine Treatment
You might also like
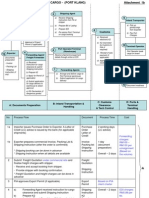
- Export + Import Process Flow - Break Bulk Cargo 27072010Document11 pagesExport + Import Process Flow - Break Bulk Cargo 27072010Ahmad Fauzi Mehat100% (1)
- DHIS Monthly Reporting Form (PHC Facilities)Document4 pagesDHIS Monthly Reporting Form (PHC Facilities)Usman89% (9)
- Developments in The Internal Dosimetry of Radiopharmaceuticals.Document6 pagesDevelopments in The Internal Dosimetry of Radiopharmaceuticals.Edis ĐedovićNo ratings yet
- Personalized Dosimetry in Diagnostic and Therapeutic Nuclear MedicineDocument34 pagesPersonalized Dosimetry in Diagnostic and Therapeutic Nuclear MedicineRafa PopocaNo ratings yet
- Meddos Published ArticleDocument6 pagesMeddos Published Articleapi-350437453No ratings yet
- Version of Record:: ManuscriptDocument22 pagesVersion of Record:: ManuscriptJayane JuliaNo ratings yet
- Analysis of Equivalent Uniform Dose (EUD) and Conventional Radiation Treatment Parameters After Primary and Re-Irradiation of Malignant GliomaDocument7 pagesAnalysis of Equivalent Uniform Dose (EUD) and Conventional Radiation Treatment Parameters After Primary and Re-Irradiation of Malignant GliomaGabriela Silva MartinsNo ratings yet
- J Nucl Med-2009-Bolch-477-84Document9 pagesJ Nucl Med-2009-Bolch-477-84alinaNo ratings yet
- 10 1016@j Ijrobp 2020 08 035Document27 pages10 1016@j Ijrobp 2020 08 035ABDO ELJANo ratings yet
- Taprogge Et Al 2021 A Systematic Review and Meta Analysis of The Relationship Between The Radiation Absorbed Dose ToDocument10 pagesTaprogge Et Al 2021 A Systematic Review and Meta Analysis of The Relationship Between The Radiation Absorbed Dose ToLesly LoachamínNo ratings yet
- Dosimetry of Yttrium-Labelled Radiopharmaceuticals For Internal Therapy: Yor Y Imaging?Document12 pagesDosimetry of Yttrium-Labelled Radiopharmaceuticals For Internal Therapy: Yor Y Imaging?sayed hossein hashemiNo ratings yet
- Comparison Between Four Modalities of Radiotherapy of Prostate CancerDocument5 pagesComparison Between Four Modalities of Radiotherapy of Prostate CancerEdis ĐedovićNo ratings yet
- Radiobiology of Re-IradiationDocument5 pagesRadiobiology of Re-IradiationrobinNo ratings yet
- Ethos 2020Document14 pagesEthos 2020Radu CiprianNo ratings yet
- ICRU Report 89-105-122Document18 pagesICRU Report 89-105-122Sandra Johana Patino LeivaNo ratings yet
- Cytogenetic Biodosimetry and Dose-Rate Effect After Radioiodine Therapy For Thyroid CancerDocument14 pagesCytogenetic Biodosimetry and Dose-Rate Effect After Radioiodine Therapy For Thyroid CancerDian Pratiwi MalikNo ratings yet
- Dose-Fractionation Sensitivity of Prostate Cancer Deduced From Radiotherapy Outcomes of 5969 Patients y Seven International Insttutional DatasetDocument8 pagesDose-Fractionation Sensitivity of Prostate Cancer Deduced From Radiotherapy Outcomes of 5969 Patients y Seven International Insttutional DatasetrgergerNo ratings yet
- Paper Alumnos 5Document14 pagesPaper Alumnos 5Victor Martinez HagenNo ratings yet
- Carrara 2012Document2 pagesCarrara 2012Samuel PernaleteNo ratings yet
- Berger 2007Document9 pagesBerger 2007Benfredj KhalilNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundTatanNo ratings yet
- Ijpr 123825Document12 pagesIjpr 123825personneNo ratings yet
- Clinical InvestigationDocument9 pagesClinical InvestigationOncología CdsNo ratings yet
- 10 14338 - Ijpt-21-00043 1Document10 pages10 14338 - Ijpt-21-00043 1Raul Matute MartinNo ratings yet
- Biij2007 Vol3 Issue2 Article6 JournalDocument14 pagesBiij2007 Vol3 Issue2 Article6 JournalpritikachandNo ratings yet
- Acute Medicine Surgery - 2022 - Miyagawa - Comparison Between Midazolam and Propofol in Acute Phase For VentilatedDocument7 pagesAcute Medicine Surgery - 2022 - Miyagawa - Comparison Between Midazolam and Propofol in Acute Phase For VentilatedteranrobleswaltergabrielNo ratings yet
- 1 s2.0 S245210942100097X MainDocument7 pages1 s2.0 S245210942100097X MainhidayatullahhaqyaarNo ratings yet
- A Phase I Trial of Stereotactic Body Radiation TherapyDocument8 pagesA Phase I Trial of Stereotactic Body Radiation TherapyRaul Matute MartinNo ratings yet
- Cancer - 2013 - Antoun - Skeletal Muscle Density Predicts Prognosis in Patients With Metastatic Renal Cell CarcinomaDocument8 pagesCancer - 2013 - Antoun - Skeletal Muscle Density Predicts Prognosis in Patients With Metastatic Renal Cell CarcinomaRushi ShahNo ratings yet
- Hermani 2019Document1 pageHermani 2019Bruno MendesNo ratings yet
- Reporting and Analyzing Dose Distributions: A Concept of Equivalent Uniform DoseDocument8 pagesReporting and Analyzing Dose Distributions: A Concept of Equivalent Uniform DoseHidajeta ĐedovićNo ratings yet
- ICRP 53 - Radiation Dose To Patients From RadiopharmaceuticalsDocument340 pagesICRP 53 - Radiation Dose To Patients From Radiopharmaceuticalsraymond_lane_7No ratings yet
- Piis0167814023001135 PDFDocument8 pagesPiis0167814023001135 PDFRaul Matute MartinNo ratings yet
- Paper: Y. Yi, M.G. Stabin, M.H. Mckaskle, M.D. Shone, and A.B. JohnsonDocument5 pagesPaper: Y. Yi, M.G. Stabin, M.H. Mckaskle, M.D. Shone, and A.B. JohnsonGoffredo PrincigalliNo ratings yet
- Dose Reduction With Iterative Reconstruction For Coronary CT Angiography: A Systematic Review and Meta-AnalysisDocument9 pagesDose Reduction With Iterative Reconstruction For Coronary CT Angiography: A Systematic Review and Meta-AnalysisHenry MruizNo ratings yet
- Biij 03 E18Document15 pagesBiij 03 E18Lalit GahlotNo ratings yet
- 372 FullDocument8 pages372 FullRaul Matute MartinNo ratings yet
- 2014 - Grassberger - C - Quantification of Proton Dose Calculation AccuracyDocument7 pages2014 - Grassberger - C - Quantification of Proton Dose Calculation AccuracyUmesh GayakeNo ratings yet
- 163 FullDocument3 pages163 FullVola FaurisNo ratings yet
- Human Biodistribution and Internal Dosimetry of 4 - (A PET Radiopharmaceutical For Imaging Muscarinic Acetylcholine Receptors in The Brain and HeartDocument10 pagesHuman Biodistribution and Internal Dosimetry of 4 - (A PET Radiopharmaceutical For Imaging Muscarinic Acetylcholine Receptors in The Brain and HeartNiamatullahNo ratings yet
- UK CONSENSUS - Normal Tissue ConstraintsDocument10 pagesUK CONSENSUS - Normal Tissue ConstraintsjorgeaznarNo ratings yet
- Dosimetry of Internal EmittersDocument8 pagesDosimetry of Internal EmittersأحمدآلزهوNo ratings yet
- Dose Evaluation For Skin and Organ in HepatocellulDocument11 pagesDose Evaluation For Skin and Organ in HepatocellulAnne MbrkNo ratings yet
- Molecular Imaging-Based Dose Painting: A Novel Paradigm For Radiation Therapy PrescriptionDocument10 pagesMolecular Imaging-Based Dose Painting: A Novel Paradigm For Radiation Therapy PrescriptionMaria Petruța DrăghiaNo ratings yet
- Topic 4Document3 pagesTopic 4Rabia BagewadiNo ratings yet
- JPM 11 01311 v2Document11 pagesJPM 11 01311 v2medical HunterNo ratings yet
- Radiotherapy and OncologyDocument7 pagesRadiotherapy and OncologyMichael Steve Camelo GuevaraNo ratings yet
- Cancer - 2019 - Jang - A Phase 2 Multicenter Study of Stereotactic Body Radiotherapy For Hepatocellular Carcinoma SafetyDocument10 pagesCancer - 2019 - Jang - A Phase 2 Multicenter Study of Stereotactic Body Radiotherapy For Hepatocellular Carcinoma SafetyKotolNo ratings yet
- (L) Emami1991Document14 pages(L) Emami1991Rafael Padilla100% (1)
- 1 s2.0 S0360301623077350 MainDocument4 pages1 s2.0 S0360301623077350 Mainjohapatino46No ratings yet
- Wang 2015Document9 pagesWang 2015Gabriela Silva MartinsNo ratings yet
- MeduriDocument4 pagesMeduriSilvia Leticia BrunoNo ratings yet
- BJR 20190845Document10 pagesBJR 20190845Raul Matute MartinNo ratings yet
- The Physics of Radioembolization - 230807 - 113550Document27 pagesThe Physics of Radioembolization - 230807 - 113550seba gNo ratings yet
- Comparison of Carbon Ion and Photon Reirradiation For Recurrent GlioblastomaDocument9 pagesComparison of Carbon Ion and Photon Reirradiation For Recurrent Glioblastomachanmaulana30No ratings yet
- Patient Radiation Dose and Protection From Cone-Beam Computed TomographyDocument7 pagesPatient Radiation Dose and Protection From Cone-Beam Computed TomographydaruNo ratings yet
- Icru Report 83Document103 pagesIcru Report 83Marlon SantosNo ratings yet
- Artigo - Extremity Exposure in Nuc MedDocument6 pagesArtigo - Extremity Exposure in Nuc MedsamuelNo ratings yet
- Practical Dosimetry of Peptide Receptor Radionuclide Therapy With Y-Labeled Somatostatin AnalogsDocument7 pagesPractical Dosimetry of Peptide Receptor Radionuclide Therapy With Y-Labeled Somatostatin AnalogsJaime Andrés Muñoz AguayoNo ratings yet
- Guideline Brachy1Document8 pagesGuideline Brachy1Benfredj KhalilNo ratings yet
- Predicción Longitudinal de La Aptitud Cardiorrespiratoria A Través de Dispositivos Portátiles en Entornos de Vida LibreDocument11 pagesPredicción Longitudinal de La Aptitud Cardiorrespiratoria A Través de Dispositivos Portátiles en Entornos de Vida Libremariojosehurtado3955No ratings yet
- Clinical Applications of Nuclear Medicine Targeted TherapyFrom EverandClinical Applications of Nuclear Medicine Targeted TherapyEmilio BombardieriNo ratings yet
- 4 - Tech Hardware SectorDocument126 pages4 - Tech Hardware SectorgirishrajsNo ratings yet
- ObjectivesDocument7 pagesObjectivesPeeka booNo ratings yet
- Cambridge International AS Level: English General Paper 8021/22 February/March 2022Document11 pagesCambridge International AS Level: English General Paper 8021/22 February/March 2022Pat Patrick100% (1)
- Mulcher TSS: User Maintenance Manual - Spare PartsDocument35 pagesMulcher TSS: User Maintenance Manual - Spare PartsSerdar FildisNo ratings yet
- To Study Well Design Aspects in HPHT EnvironmentDocument40 pagesTo Study Well Design Aspects in HPHT Environmentnikhil_barshettiwat100% (1)
- PHY101A: Home Experiment - 1: Simple Pendulum: PHY101A - Physics Laboratory Ha - 1B Ynm/Ahk/Sub/SdDocument6 pagesPHY101A: Home Experiment - 1: Simple Pendulum: PHY101A - Physics Laboratory Ha - 1B Ynm/Ahk/Sub/SdHarsitNo ratings yet
- Mathematics ECAT (Sir Nasim Zulfiqar) - 1Document134 pagesMathematics ECAT (Sir Nasim Zulfiqar) - 1AYESH qureshiNo ratings yet
- HD Hammock InstDocument4 pagesHD Hammock InstLarry WagarNo ratings yet
- CBT JournalDocument82 pagesCBT JournalPaige Bayly100% (1)
- Rate of Burning And/or Extent and Time of Burning of Plastics in A Horizontal PositionDocument8 pagesRate of Burning And/or Extent and Time of Burning of Plastics in A Horizontal PositionjoseNo ratings yet
- Context CluesDocument7 pagesContext CluesasherNo ratings yet
- Valve SelectionDocument5 pagesValve SelectionmansurNo ratings yet
- Polyurea EbookDocument39 pagesPolyurea EbookJesus De la Rosa100% (1)
- DL24MP HDocument13 pagesDL24MP HTamás SzabóNo ratings yet
- Manual Romi GL 240Document170 pagesManual Romi GL 240FlavioJS10No ratings yet
- Differential Equations MSC MathematicsDocument2 pagesDifferential Equations MSC MathematicsSamadNo ratings yet
- Turbojet EnginesDocument22 pagesTurbojet EnginesAldo SamuelNo ratings yet
- LDDS-H: DC-DC Constant Current Step-Down LED DriverDocument5 pagesLDDS-H: DC-DC Constant Current Step-Down LED Driverfhfgh gjgfhNo ratings yet
- PPDocument15 pagesPPdana angela hernandezNo ratings yet
- Physics of Everyday Phenomena A Conceptual Introduction To Physics 8th Edition Griffith Test BankDocument14 pagesPhysics of Everyday Phenomena A Conceptual Introduction To Physics 8th Edition Griffith Test Bankdavidhallwopkseimgc100% (32)
- 1 - 语法点1Run-On SentenceDocument11 pages1 - 语法点1Run-On Sentenceihmc_cwNo ratings yet
- NIFLECDocument6 pagesNIFLECRonald Ariyanto WiradirnataNo ratings yet
- 3b Domestic Water Meter Installation in Meter Room GuidelinesDocument10 pages3b Domestic Water Meter Installation in Meter Room GuidelinesVinish HARIDAS NAIRNo ratings yet
- Pia Calabarzon 7 Prs (April 12,15, 2013), Dispatch For April 15, 2013 (Monday)Document34 pagesPia Calabarzon 7 Prs (April 12,15, 2013), Dispatch For April 15, 2013 (Monday)Pia QuezonNo ratings yet
- Hypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHDocument6 pagesHypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHLeyla SaabNo ratings yet
- The Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFDocument2 pagesThe Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFMarlui Faith MaglambayanNo ratings yet
- LI L1 Grammar ExtensionDocument15 pagesLI L1 Grammar ExtensionSandra BinstokNo ratings yet
- Kami Export - Text Purpose & Author ToneDocument8 pagesKami Export - Text Purpose & Author ToneIcha SawaliNo ratings yet
























































































Download as pdf or txt
You might also like
- Export + Import Process Flow - Break Bulk Cargo 27072010Document11 pagesExport + Import Process Flow - Break Bulk Cargo 27072010Ahmad Fauzi Mehat100% (1)
- DHIS Monthly Reporting Form (PHC Facilities)Document4 pagesDHIS Monthly Reporting Form (PHC Facilities)Usman89% (9)
- Developments in The Internal Dosimetry of Radiopharmaceuticals.Document6 pagesDevelopments in The Internal Dosimetry of Radiopharmaceuticals.Edis ĐedovićNo ratings yet
- Personalized Dosimetry in Diagnostic and Therapeutic Nuclear MedicineDocument34 pagesPersonalized Dosimetry in Diagnostic and Therapeutic Nuclear MedicineRafa PopocaNo ratings yet
- Meddos Published ArticleDocument6 pagesMeddos Published Articleapi-350437453No ratings yet
- Version of Record:: ManuscriptDocument22 pagesVersion of Record:: ManuscriptJayane JuliaNo ratings yet
- Analysis of Equivalent Uniform Dose (EUD) and Conventional Radiation Treatment Parameters After Primary and Re-Irradiation of Malignant GliomaDocument7 pagesAnalysis of Equivalent Uniform Dose (EUD) and Conventional Radiation Treatment Parameters After Primary and Re-Irradiation of Malignant GliomaGabriela Silva MartinsNo ratings yet
- J Nucl Med-2009-Bolch-477-84Document9 pagesJ Nucl Med-2009-Bolch-477-84alinaNo ratings yet
- 10 1016@j Ijrobp 2020 08 035Document27 pages10 1016@j Ijrobp 2020 08 035ABDO ELJANo ratings yet
- Taprogge Et Al 2021 A Systematic Review and Meta Analysis of The Relationship Between The Radiation Absorbed Dose ToDocument10 pagesTaprogge Et Al 2021 A Systematic Review and Meta Analysis of The Relationship Between The Radiation Absorbed Dose ToLesly LoachamínNo ratings yet
- Dosimetry of Yttrium-Labelled Radiopharmaceuticals For Internal Therapy: Yor Y Imaging?Document12 pagesDosimetry of Yttrium-Labelled Radiopharmaceuticals For Internal Therapy: Yor Y Imaging?sayed hossein hashemiNo ratings yet
- Comparison Between Four Modalities of Radiotherapy of Prostate CancerDocument5 pagesComparison Between Four Modalities of Radiotherapy of Prostate CancerEdis ĐedovićNo ratings yet
- Radiobiology of Re-IradiationDocument5 pagesRadiobiology of Re-IradiationrobinNo ratings yet
- Ethos 2020Document14 pagesEthos 2020Radu CiprianNo ratings yet
- ICRU Report 89-105-122Document18 pagesICRU Report 89-105-122Sandra Johana Patino LeivaNo ratings yet
- Cytogenetic Biodosimetry and Dose-Rate Effect After Radioiodine Therapy For Thyroid CancerDocument14 pagesCytogenetic Biodosimetry and Dose-Rate Effect After Radioiodine Therapy For Thyroid CancerDian Pratiwi MalikNo ratings yet
- Dose-Fractionation Sensitivity of Prostate Cancer Deduced From Radiotherapy Outcomes of 5969 Patients y Seven International Insttutional DatasetDocument8 pagesDose-Fractionation Sensitivity of Prostate Cancer Deduced From Radiotherapy Outcomes of 5969 Patients y Seven International Insttutional DatasetrgergerNo ratings yet
- Paper Alumnos 5Document14 pagesPaper Alumnos 5Victor Martinez HagenNo ratings yet
- Carrara 2012Document2 pagesCarrara 2012Samuel PernaleteNo ratings yet
- Berger 2007Document9 pagesBerger 2007Benfredj KhalilNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundTatanNo ratings yet
- Ijpr 123825Document12 pagesIjpr 123825personneNo ratings yet
- Clinical InvestigationDocument9 pagesClinical InvestigationOncología CdsNo ratings yet
- 10 14338 - Ijpt-21-00043 1Document10 pages10 14338 - Ijpt-21-00043 1Raul Matute MartinNo ratings yet
- Biij2007 Vol3 Issue2 Article6 JournalDocument14 pagesBiij2007 Vol3 Issue2 Article6 JournalpritikachandNo ratings yet
- Acute Medicine Surgery - 2022 - Miyagawa - Comparison Between Midazolam and Propofol in Acute Phase For VentilatedDocument7 pagesAcute Medicine Surgery - 2022 - Miyagawa - Comparison Between Midazolam and Propofol in Acute Phase For VentilatedteranrobleswaltergabrielNo ratings yet
- 1 s2.0 S245210942100097X MainDocument7 pages1 s2.0 S245210942100097X MainhidayatullahhaqyaarNo ratings yet
- A Phase I Trial of Stereotactic Body Radiation TherapyDocument8 pagesA Phase I Trial of Stereotactic Body Radiation TherapyRaul Matute MartinNo ratings yet
- Cancer - 2013 - Antoun - Skeletal Muscle Density Predicts Prognosis in Patients With Metastatic Renal Cell CarcinomaDocument8 pagesCancer - 2013 - Antoun - Skeletal Muscle Density Predicts Prognosis in Patients With Metastatic Renal Cell CarcinomaRushi ShahNo ratings yet
- Hermani 2019Document1 pageHermani 2019Bruno MendesNo ratings yet
- Reporting and Analyzing Dose Distributions: A Concept of Equivalent Uniform DoseDocument8 pagesReporting and Analyzing Dose Distributions: A Concept of Equivalent Uniform DoseHidajeta ĐedovićNo ratings yet
- ICRP 53 - Radiation Dose To Patients From RadiopharmaceuticalsDocument340 pagesICRP 53 - Radiation Dose To Patients From Radiopharmaceuticalsraymond_lane_7No ratings yet
- Piis0167814023001135 PDFDocument8 pagesPiis0167814023001135 PDFRaul Matute MartinNo ratings yet
- Paper: Y. Yi, M.G. Stabin, M.H. Mckaskle, M.D. Shone, and A.B. JohnsonDocument5 pagesPaper: Y. Yi, M.G. Stabin, M.H. Mckaskle, M.D. Shone, and A.B. JohnsonGoffredo PrincigalliNo ratings yet
- Dose Reduction With Iterative Reconstruction For Coronary CT Angiography: A Systematic Review and Meta-AnalysisDocument9 pagesDose Reduction With Iterative Reconstruction For Coronary CT Angiography: A Systematic Review and Meta-AnalysisHenry MruizNo ratings yet
- Biij 03 E18Document15 pagesBiij 03 E18Lalit GahlotNo ratings yet
- 372 FullDocument8 pages372 FullRaul Matute MartinNo ratings yet
- 2014 - Grassberger - C - Quantification of Proton Dose Calculation AccuracyDocument7 pages2014 - Grassberger - C - Quantification of Proton Dose Calculation AccuracyUmesh GayakeNo ratings yet
- 163 FullDocument3 pages163 FullVola FaurisNo ratings yet
- Human Biodistribution and Internal Dosimetry of 4 - (A PET Radiopharmaceutical For Imaging Muscarinic Acetylcholine Receptors in The Brain and HeartDocument10 pagesHuman Biodistribution and Internal Dosimetry of 4 - (A PET Radiopharmaceutical For Imaging Muscarinic Acetylcholine Receptors in The Brain and HeartNiamatullahNo ratings yet
- UK CONSENSUS - Normal Tissue ConstraintsDocument10 pagesUK CONSENSUS - Normal Tissue ConstraintsjorgeaznarNo ratings yet
- Dosimetry of Internal EmittersDocument8 pagesDosimetry of Internal EmittersأحمدآلزهوNo ratings yet
- Dose Evaluation For Skin and Organ in HepatocellulDocument11 pagesDose Evaluation For Skin and Organ in HepatocellulAnne MbrkNo ratings yet
- Molecular Imaging-Based Dose Painting: A Novel Paradigm For Radiation Therapy PrescriptionDocument10 pagesMolecular Imaging-Based Dose Painting: A Novel Paradigm For Radiation Therapy PrescriptionMaria Petruța DrăghiaNo ratings yet
- Topic 4Document3 pagesTopic 4Rabia BagewadiNo ratings yet
- JPM 11 01311 v2Document11 pagesJPM 11 01311 v2medical HunterNo ratings yet
- Radiotherapy and OncologyDocument7 pagesRadiotherapy and OncologyMichael Steve Camelo GuevaraNo ratings yet
- Cancer - 2019 - Jang - A Phase 2 Multicenter Study of Stereotactic Body Radiotherapy For Hepatocellular Carcinoma SafetyDocument10 pagesCancer - 2019 - Jang - A Phase 2 Multicenter Study of Stereotactic Body Radiotherapy For Hepatocellular Carcinoma SafetyKotolNo ratings yet
- (L) Emami1991Document14 pages(L) Emami1991Rafael Padilla100% (1)
- 1 s2.0 S0360301623077350 MainDocument4 pages1 s2.0 S0360301623077350 Mainjohapatino46No ratings yet
- Wang 2015Document9 pagesWang 2015Gabriela Silva MartinsNo ratings yet
- MeduriDocument4 pagesMeduriSilvia Leticia BrunoNo ratings yet
- BJR 20190845Document10 pagesBJR 20190845Raul Matute MartinNo ratings yet
- The Physics of Radioembolization - 230807 - 113550Document27 pagesThe Physics of Radioembolization - 230807 - 113550seba gNo ratings yet
- Comparison of Carbon Ion and Photon Reirradiation For Recurrent GlioblastomaDocument9 pagesComparison of Carbon Ion and Photon Reirradiation For Recurrent Glioblastomachanmaulana30No ratings yet
- Patient Radiation Dose and Protection From Cone-Beam Computed TomographyDocument7 pagesPatient Radiation Dose and Protection From Cone-Beam Computed TomographydaruNo ratings yet
- Icru Report 83Document103 pagesIcru Report 83Marlon SantosNo ratings yet
- Artigo - Extremity Exposure in Nuc MedDocument6 pagesArtigo - Extremity Exposure in Nuc MedsamuelNo ratings yet
- Practical Dosimetry of Peptide Receptor Radionuclide Therapy With Y-Labeled Somatostatin AnalogsDocument7 pagesPractical Dosimetry of Peptide Receptor Radionuclide Therapy With Y-Labeled Somatostatin AnalogsJaime Andrés Muñoz AguayoNo ratings yet
- Guideline Brachy1Document8 pagesGuideline Brachy1Benfredj KhalilNo ratings yet
- Predicción Longitudinal de La Aptitud Cardiorrespiratoria A Través de Dispositivos Portátiles en Entornos de Vida LibreDocument11 pagesPredicción Longitudinal de La Aptitud Cardiorrespiratoria A Través de Dispositivos Portátiles en Entornos de Vida Libremariojosehurtado3955No ratings yet
- Clinical Applications of Nuclear Medicine Targeted TherapyFrom EverandClinical Applications of Nuclear Medicine Targeted TherapyEmilio BombardieriNo ratings yet
- 4 - Tech Hardware SectorDocument126 pages4 - Tech Hardware SectorgirishrajsNo ratings yet
- ObjectivesDocument7 pagesObjectivesPeeka booNo ratings yet
- Cambridge International AS Level: English General Paper 8021/22 February/March 2022Document11 pagesCambridge International AS Level: English General Paper 8021/22 February/March 2022Pat Patrick100% (1)
- Mulcher TSS: User Maintenance Manual - Spare PartsDocument35 pagesMulcher TSS: User Maintenance Manual - Spare PartsSerdar FildisNo ratings yet
- To Study Well Design Aspects in HPHT EnvironmentDocument40 pagesTo Study Well Design Aspects in HPHT Environmentnikhil_barshettiwat100% (1)
- PHY101A: Home Experiment - 1: Simple Pendulum: PHY101A - Physics Laboratory Ha - 1B Ynm/Ahk/Sub/SdDocument6 pagesPHY101A: Home Experiment - 1: Simple Pendulum: PHY101A - Physics Laboratory Ha - 1B Ynm/Ahk/Sub/SdHarsitNo ratings yet
- Mathematics ECAT (Sir Nasim Zulfiqar) - 1Document134 pagesMathematics ECAT (Sir Nasim Zulfiqar) - 1AYESH qureshiNo ratings yet
- HD Hammock InstDocument4 pagesHD Hammock InstLarry WagarNo ratings yet
- CBT JournalDocument82 pagesCBT JournalPaige Bayly100% (1)
- Rate of Burning And/or Extent and Time of Burning of Plastics in A Horizontal PositionDocument8 pagesRate of Burning And/or Extent and Time of Burning of Plastics in A Horizontal PositionjoseNo ratings yet
- Context CluesDocument7 pagesContext CluesasherNo ratings yet
- Valve SelectionDocument5 pagesValve SelectionmansurNo ratings yet
- Polyurea EbookDocument39 pagesPolyurea EbookJesus De la Rosa100% (1)
- DL24MP HDocument13 pagesDL24MP HTamás SzabóNo ratings yet
- Manual Romi GL 240Document170 pagesManual Romi GL 240FlavioJS10No ratings yet
- Differential Equations MSC MathematicsDocument2 pagesDifferential Equations MSC MathematicsSamadNo ratings yet
- Turbojet EnginesDocument22 pagesTurbojet EnginesAldo SamuelNo ratings yet
- LDDS-H: DC-DC Constant Current Step-Down LED DriverDocument5 pagesLDDS-H: DC-DC Constant Current Step-Down LED Driverfhfgh gjgfhNo ratings yet
- PPDocument15 pagesPPdana angela hernandezNo ratings yet
- Physics of Everyday Phenomena A Conceptual Introduction To Physics 8th Edition Griffith Test BankDocument14 pagesPhysics of Everyday Phenomena A Conceptual Introduction To Physics 8th Edition Griffith Test Bankdavidhallwopkseimgc100% (32)
- 1 - 语法点1Run-On SentenceDocument11 pages1 - 语法点1Run-On Sentenceihmc_cwNo ratings yet
- NIFLECDocument6 pagesNIFLECRonald Ariyanto WiradirnataNo ratings yet
- 3b Domestic Water Meter Installation in Meter Room GuidelinesDocument10 pages3b Domestic Water Meter Installation in Meter Room GuidelinesVinish HARIDAS NAIRNo ratings yet
- Pia Calabarzon 7 Prs (April 12,15, 2013), Dispatch For April 15, 2013 (Monday)Document34 pagesPia Calabarzon 7 Prs (April 12,15, 2013), Dispatch For April 15, 2013 (Monday)Pia QuezonNo ratings yet
- Hypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHDocument6 pagesHypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHLeyla SaabNo ratings yet
- The Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFDocument2 pagesThe Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFMarlui Faith MaglambayanNo ratings yet
- LI L1 Grammar ExtensionDocument15 pagesLI L1 Grammar ExtensionSandra BinstokNo ratings yet
- Kami Export - Text Purpose & Author ToneDocument8 pagesKami Export - Text Purpose & Author ToneIcha SawaliNo ratings yet