Download as pdf or txt
You might also like
- Metacognitive Therapy For Generalized AnxietyDocument7 pagesMetacognitive Therapy For Generalized AnxietySergio Ignacio VaccaroNo ratings yet
- Well and High ProteinDocument12 pagesWell and High Proteingaurav singhNo ratings yet
- Fat Vs Carb RestrictedDocument4 pagesFat Vs Carb RestrictedGiolla HijabNo ratings yet
- Dietary TX of Obesity 08Document14 pagesDietary TX of Obesity 08chigolinNo ratings yet
- Comparison of High-Fat and High-Protein Diets With A High-Carbohydrate Diet in Insulin-Resistant Obese WomenDocument9 pagesComparison of High-Fat and High-Protein Diets With A High-Carbohydrate Diet in Insulin-Resistant Obese WomenDanielle AliceNo ratings yet
- ASs 2 OriginalDocument13 pagesASs 2 OriginalArushi GuptaNo ratings yet
- Makalah Pi Pangan Kelompok 3Document4 pagesMakalah Pi Pangan Kelompok 3kristina sipayungNo ratings yet
- A Randomized Trial of A Low-Carbohydrate Diet For Obesity - NEJMDocument16 pagesA Randomized Trial of A Low-Carbohydrate Diet For Obesity - NEJMMateo PeychauxNo ratings yet
- Calorie Restriction With or Without Exercise On Insulin Sensitivity Beta Cell Functions Ectopic LipidDocument8 pagesCalorie Restriction With or Without Exercise On Insulin Sensitivity Beta Cell Functions Ectopic Lipidadibahfauzi85No ratings yet
- Original Article The Effect of A Low-Fat, High-Protein or High-Carbohydrate Ad Libitum Diet On Weight Loss Maintenance and Metabolic Risk FactorsDocument9 pagesOriginal Article The Effect of A Low-Fat, High-Protein or High-Carbohydrate Ad Libitum Diet On Weight Loss Maintenance and Metabolic Risk FactorsIyappan SubramaniNo ratings yet
- Evidencia Científica de Dietas para Bajar de Peso Diferente Composición de Macronutrientes, Ayuno Intermitente y Dietas PopularesDocument35 pagesEvidencia Científica de Dietas para Bajar de Peso Diferente Composición de Macronutrientes, Ayuno Intermitente y Dietas PopularesCesar Flores ValleNo ratings yet
- Dietas de Baixa CaloriaDocument11 pagesDietas de Baixa CaloriaDesolation FestNo ratings yet
- Carbohydrates Research-5Document8 pagesCarbohydrates Research-5api-466416222No ratings yet
- The Effect of High-Protein, Low-Carbohydrate Diets in The Treatment of Type 2 Diabetes: A 12 Month Randomised Controlled TrialDocument10 pagesThe Effect of High-Protein, Low-Carbohydrate Diets in The Treatment of Type 2 Diabetes: A 12 Month Randomised Controlled TrialFirda Rizky KhoerunnissaNo ratings yet
- Role of Ketogenic Diets in Neurodegenerative DiseasesDocument11 pagesRole of Ketogenic Diets in Neurodegenerative DiseasesAhmed AmerNo ratings yet
- ArticleDocument9 pagesArticlernvisNo ratings yet
- Ketogenic Diet PDFDocument37 pagesKetogenic Diet PDFVimal KumarNo ratings yet
- Effect of An Energy-Restricted, High-Protein, Low-Fat Diet Relative To A Conventional High-Carbohydrate-Am J Clin Nutr-2005-Noakes-1298-306Document9 pagesEffect of An Energy-Restricted, High-Protein, Low-Fat Diet Relative To A Conventional High-Carbohydrate-Am J Clin Nutr-2005-Noakes-1298-306Ivonne BarrazaNo ratings yet
- Ketogenic Diet IF-Philippine Lipid Society Consensus-Statement-20191108v4Document21 pagesKetogenic Diet IF-Philippine Lipid Society Consensus-Statement-20191108v4donmd98No ratings yet
- Nutrients 11 00586Document12 pagesNutrients 11 00586Meisya Nur'ainiNo ratings yet
- Postul Intermitent (Intermittent Fasting) Pentru SlabireDocument3 pagesPostul Intermitent (Intermittent Fasting) Pentru SlabireSeb SaabNo ratings yet
- Effects of A High-Protein Ketogenic Diet On Hunger, Appetite, and Weight Loss in Obese Men Feeding Ad Libitum-Am J Clin Nutr-2008-Johnstone-44-55Document12 pagesEffects of A High-Protein Ketogenic Diet On Hunger, Appetite, and Weight Loss in Obese Men Feeding Ad Libitum-Am J Clin Nutr-2008-Johnstone-44-55Ivonne BarrazaNo ratings yet
- The Effects of A Low Glycemic Load Diet On Weight Loss and Key Health Risk IndicatorsDocument8 pagesThe Effects of A Low Glycemic Load Diet On Weight Loss and Key Health Risk IndicatorsAnonymous G6zDTD2yNo ratings yet
- A Low-CarbohydrDocument8 pagesA Low-Carbohydrbea.afbNo ratings yet
- Low-Fat Vs Low-CarbDocument8 pagesLow-Fat Vs Low-CarbTrismegisteNo ratings yet
- PDF Philippine-CONSENSUS-STATEMENT-FINAL-BJMeditsDocument21 pagesPDF Philippine-CONSENSUS-STATEMENT-FINAL-BJMeditsElly JoyNo ratings yet
- Weight-Loss Diets For The Prevention and Treatment of ObesityDocument3 pagesWeight-Loss Diets For The Prevention and Treatment of ObesityRupita SitanggangNo ratings yet
- Intermittent Fasting Combined With Calorie Restriction Is Effective For Weight Loss and Cardio-Protection in Obese WomenDocument9 pagesIntermittent Fasting Combined With Calorie Restriction Is Effective For Weight Loss and Cardio-Protection in Obese Womenpriya1832No ratings yet
- Wa0102.Document18 pagesWa0102.천사자No ratings yet
- 1743 7075 7 17 PDFDocument10 pages1743 7075 7 17 PDFmarquelia.jardonNo ratings yet
- Nutrients: A Scientific Perspective of Personalised Gene-Based Dietary Recommendations For Weight ManagementDocument14 pagesNutrients: A Scientific Perspective of Personalised Gene-Based Dietary Recommendations For Weight ManagementMeisya Nur'ainiNo ratings yet
- Wiliam Yancy PDFDocument7 pagesWiliam Yancy PDFDeaz Fazzaura PutriNo ratings yet
- Đánh giá chế độ ăn kiêng: Nhịn ăn gián đoạn để giảm cân- wed HarvardDocument14 pagesĐánh giá chế độ ăn kiêng: Nhịn ăn gián đoạn để giảm cân- wed HarvardNam NguyenHoangNo ratings yet
- Abstrac 2222Document19 pagesAbstrac 2222josephmainam9No ratings yet
- Ketogenic DietsDocument23 pagesKetogenic DietsNorma Edith López DíazGuerreroNo ratings yet
- Detailed Ketogenic Diet For EvryoneDocument16 pagesDetailed Ketogenic Diet For EvryoneAmit Raj100% (1)
- Effect of Fat Intake On Energy BalanceDocument7 pagesEffect of Fat Intake On Energy BalancekarlosNo ratings yet
- Abbasi - 2018 - Interest in The Ketogenic Diet Grows For Weight Loss and Type 2 DiabetesDocument3 pagesAbbasi - 2018 - Interest in The Ketogenic Diet Grows For Weight Loss and Type 2 DiabetesFilipe Brito NutricionistaNo ratings yet
- Ebook To A Ketogenic Diet For Weight Loss and Metabolic DiseaseDocument43 pagesEbook To A Ketogenic Diet For Weight Loss and Metabolic Diseasemerlinchabochi100% (1)
- Final 4Document11 pagesFinal 4api-722911357No ratings yet
- Obesity - Short Scientific Findings to Ameliorate the Body WeightFrom EverandObesity - Short Scientific Findings to Ameliorate the Body WeightNo ratings yet
- A Review On Lowcarbohydrate Diet and Womens HealthDocument7 pagesA Review On Lowcarbohydrate Diet and Womens HealthTyas Asri AnindyaningrumNo ratings yet
- AbstractDocument16 pagesAbstractjosephmainam9No ratings yet
- SalmanDocument13 pagesSalmansalman ahmadNo ratings yet
- Hall, K D Et Al (2018) Weight Loss Maintenance: A Review On Dietary Related StrategiesDocument15 pagesHall, K D Et Al (2018) Weight Loss Maintenance: A Review On Dietary Related Strategiesasdrubal5martinezNo ratings yet
- LCLF 05.12.20 SubmittedDocument79 pagesLCLF 05.12.20 SubmittedJosetomasNo ratings yet
- Moderate CarbohydrateDocument9 pagesModerate CarbohydrateAndrea TorrealdayNo ratings yet
- Aula 1 - Long Term Weight Maintenance After Advice To Consume Low CarbohydratDocument37 pagesAula 1 - Long Term Weight Maintenance After Advice To Consume Low CarbohydratRayane SilvaNo ratings yet
- 10 3390@nu12072005Document19 pages10 3390@nu12072005Maria Isabel LondoñoNo ratings yet
- Rosenbaum Et Al-2019-ObesityDocument12 pagesRosenbaum Et Al-2019-ObesityaloverofdanceNo ratings yet
- Esfahani Et al-2011-IUBMB Life PDFDocument7 pagesEsfahani Et al-2011-IUBMB Life PDFLisiane PerinNo ratings yet
- Chocolate With High Cocoa Content As A Weight-Loss AcceleratorDocument9 pagesChocolate With High Cocoa Content As A Weight-Loss AcceleratorRamshaNo ratings yet
- Fnut 08 640538Document12 pagesFnut 08 640538Douglas RodriguesNo ratings yet
- Increased Consumption of Dairy Foods and Protein During Diet - and Exercise-Induced Weight Loss Promotes Fat Mass Loss and Lean Mass Gain in Overweight and Obese Premenopausal WomenDocument9 pagesIncreased Consumption of Dairy Foods and Protein During Diet - and Exercise-Induced Weight Loss Promotes Fat Mass Loss and Lean Mass Gain in Overweight and Obese Premenopausal Womenines.queiros.nutricionistaNo ratings yet
- Review of LituratureDocument12 pagesReview of Lituraturealive computerNo ratings yet
- Human Nutrition and MetabolismDocument7 pagesHuman Nutrition and MetabolismMisyani MisyaniNo ratings yet
- Principia Ketogenica 2014082901Document289 pagesPrincipia Ketogenica 2014082901erixsparhawk50% (2)
- The Ketogenic DietDocument6 pagesThe Ketogenic DietSOU BRASILEIRO ELEIÇÕESNo ratings yet
- Weight Management Clinical TrialsDocument7 pagesWeight Management Clinical TrialschuariwapoohNo ratings yet
- Effects of Macronutrient Intake in Obesity A Mt-AnalysisDocument16 pagesEffects of Macronutrient Intake in Obesity A Mt-AnalysisJúlia BenckeNo ratings yet
- 2.01 Measures of Disease FrequencyDocument6 pages2.01 Measures of Disease Frequencygene2693No ratings yet
- Hindustan Times Delhi 21 - 6Document44 pagesHindustan Times Delhi 21 - 6Hmbe hmbeNo ratings yet
- Hypoxic-Ischemic Encephalopathy (HIE)Document9 pagesHypoxic-Ischemic Encephalopathy (HIE)Ritu VermaNo ratings yet
- Biological Aspects of Orthodontic Tooth Movement: A Review of LiteratureDocument6 pagesBiological Aspects of Orthodontic Tooth Movement: A Review of LiteratureZulma Moreno HuertasNo ratings yet
- Growth and Development of Temporomandibular JointDocument40 pagesGrowth and Development of Temporomandibular JointSadhu AbhijeetNo ratings yet
- Eutrophication HandoutDocument2 pagesEutrophication HandoutJul Necholie RosalesNo ratings yet
- 2000 Yds Sorusu TestlerDocument116 pages2000 Yds Sorusu TestlerMerve Şahin100% (1)
- ECT Electroconvulsive Therapy Fact SheetDocument4 pagesECT Electroconvulsive Therapy Fact SheetSonali DakhoreNo ratings yet
- Lecture 1 Course Specification of General BacteriologyDocument36 pagesLecture 1 Course Specification of General BacteriologyNedhal Mahmoud KaleefahNo ratings yet
- The Importance of Mineral Elements For Humans, Domestic Animals and Plants: A ReviewDocument3 pagesThe Importance of Mineral Elements For Humans, Domestic Animals and Plants: A ReviewMaricel Canlas MacatoNo ratings yet
- To What Extent Were The World War II Internment Camps On The Isle of Man Total Institutions'? A Case Study of Onchan Camp 1940-41Document46 pagesTo What Extent Were The World War II Internment Camps On The Isle of Man Total Institutions'? A Case Study of Onchan Camp 1940-41thomiddonNo ratings yet
- 38 Feam Ejb EngDocument4 pages38 Feam Ejb EngSaufi YatimNo ratings yet
- Spa SampleDocument2 pagesSpa Samplecathy cardozaNo ratings yet
- Rabies VaccineDocument2 pagesRabies VaccineMichael DharshwinNo ratings yet
- BFR 06 - Scene Assessment and SafetyDocument18 pagesBFR 06 - Scene Assessment and SafetyDex Valdez100% (1)
- Why Kids Need DirtDocument5 pagesWhy Kids Need DirtViraj Shelke100% (1)
- Chapter 40. Nursing Care of A Child With Respiratory Disorder TermsDocument3 pagesChapter 40. Nursing Care of A Child With Respiratory Disorder TermsJœnríčk AzueloNo ratings yet
- Let's Check - Divinagracia N AgravanteDocument2 pagesLet's Check - Divinagracia N AgravanteGladys YaresNo ratings yet
- Home Health Supervision Rating ScaleDocument1 pageHome Health Supervision Rating ScaleCarol WIngfieldNo ratings yet
- NO Facts Ideas Learning Issues Action PlanDocument2 pagesNO Facts Ideas Learning Issues Action PlandharwinNo ratings yet
- Proximal Humerus and Humeral Shaft Fractures in Children: M. Wade Shrader, MDDocument5 pagesProximal Humerus and Humeral Shaft Fractures in Children: M. Wade Shrader, MDRoyman MejiaNo ratings yet
- How Did JoeDocument2 pagesHow Did JoeIvanNo ratings yet
- Facility Health, Safety & Environmental ManagementDocument41 pagesFacility Health, Safety & Environmental ManagementAhmad Saiful Ridzwan Jaharuddin100% (3)
- Allergy & ImmunologyDocument55 pagesAllergy & ImmunologyRaheelaNo ratings yet
- Philippine PovertyDocument2 pagesPhilippine PovertyHannah BarandaNo ratings yet
- Being Silenced Loneliness and Being HeardDocument18 pagesBeing Silenced Loneliness and Being HeardMáytee CastellNo ratings yet
- Herbal Cosmetics: Raheem Bahadar PHD ScholarDocument41 pagesHerbal Cosmetics: Raheem Bahadar PHD ScholarashahmednNo ratings yet
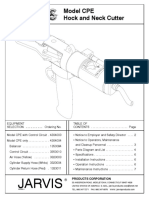
- Manual Corta Pescuezos Jarvis CPEDocument8 pagesManual Corta Pescuezos Jarvis CPEJorge Jimenez100% (1)
- Coral LLC DocumentsDocument8 pagesCoral LLC Documentsfariha farheenNo ratings yet