Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Leslie Feinberg - Drag King Dreams-Carroll & Graf Publishers (2006)Document324 pagesLeslie Feinberg - Drag King Dreams-Carroll & Graf Publishers (2006)ce100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pi Bu Zonas CutáneasDocument4 pagesPi Bu Zonas CutáneasjjseguinNo ratings yet
- Blood Pressure Levels For Boys by Age and Height PercentileDocument4 pagesBlood Pressure Levels For Boys by Age and Height PercentileNuzla EmiraNo ratings yet
- Nevirapine Clinical PREADocument44 pagesNevirapine Clinical PREAjoelrequenaNo ratings yet
- Office of Clinical Pharmacology ReviewDocument40 pagesOffice of Clinical Pharmacology ReviewjoelrequenaNo ratings yet
- 201153imiquimod ClinPharm PREADocument38 pages201153imiquimod ClinPharm PREAjoelrequenaNo ratings yet
- A6 PDFDocument14 pagesA6 PDFjoelrequenaNo ratings yet
- Clinical Executive Summary: Treatment of Bipolar I DisorderDocument9 pagesClinical Executive Summary: Treatment of Bipolar I DisorderjoelrequenaNo ratings yet
- A16 PDFDocument22 pagesA16 PDFjoelrequenaNo ratings yet
- A1 PDFDocument4 pagesA1 PDFjoelrequenaNo ratings yet
- A2 PDFDocument29 pagesA2 PDFjoelrequenaNo ratings yet
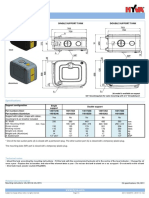
- Hyva Oil Tank: Single Support Tank Double Support TankDocument4 pagesHyva Oil Tank: Single Support Tank Double Support TankPutera Bumi NusantaraNo ratings yet
- FingerprintingDocument36 pagesFingerprintingapi-291003259100% (2)
- Chapter 6 Food Handlers Safety HygieneDocument20 pagesChapter 6 Food Handlers Safety HygieneIrish MalabananNo ratings yet
- Msds Heksana - 2 PDFDocument6 pagesMsds Heksana - 2 PDFGelisaNo ratings yet
- Psychology TheoriesDocument22 pagesPsychology TheoriesErikka S. Atienza100% (3)
- SITREP NUMBER 62 As of 29 January 2020 1100HDocument67 pagesSITREP NUMBER 62 As of 29 January 2020 1100HEdison ManaloNo ratings yet
- Valuing The Suitable Agro-Industrial Wastes For Cultivation of P. Platypus and P. EousDocument4 pagesValuing The Suitable Agro-Industrial Wastes For Cultivation of P. Platypus and P. EousDinesh Babu PugalenthiNo ratings yet
- Botanical Orign: Peppermint OilDocument4 pagesBotanical Orign: Peppermint OilSidra TariqNo ratings yet
- Employee Separation and Retention (Q3)Document2 pagesEmployee Separation and Retention (Q3)BSMA Third YearNo ratings yet
- Evidence From QuranDocument6 pagesEvidence From QuranHaziq Hakeem Ahmad Affandi100% (1)
- Escalator Switches AdjustmentDocument6 pagesEscalator Switches AdjustmentSANAL KUMAR SNo ratings yet
- Iso 50001 Enms - Manual-Procedures-Forms-Matrix - P-XXX NumbersDocument1 pageIso 50001 Enms - Manual-Procedures-Forms-Matrix - P-XXX NumbersAngelo SantiagoNo ratings yet
- Dichotic Listening El 100Document22 pagesDichotic Listening El 100Melody Jane CastroNo ratings yet
- Demonizing Drugmakers: The Political Assault On The Pharmaceutical Industry, Cato Policy Analysis No. 475Document56 pagesDemonizing Drugmakers: The Political Assault On The Pharmaceutical Industry, Cato Policy Analysis No. 475Cato InstituteNo ratings yet
- Abus LightweightDocument2 pagesAbus LightweightGloria RomicNo ratings yet
- Father's of Various FieldsDocument5 pagesFather's of Various FieldsAsad AliNo ratings yet
- SeizureDocument10 pagesSeizureRomeo ReyesNo ratings yet
- Speaking Listening 1Document3 pagesSpeaking Listening 1fara dias safrinaNo ratings yet
- 11 SMAW Q4 Module 2Document11 pages11 SMAW Q4 Module 2Mark Johnson VillaronNo ratings yet
- Half Yearly Portion & Blue Print 2022-23 - STD ViiDocument2 pagesHalf Yearly Portion & Blue Print 2022-23 - STD ViiSsNo ratings yet
- Oxidation of N-Acetyl Alanine by Chloramine-T in Presence of Hydrochloric Acid: A Kinetic and Mechanistic StudyDocument10 pagesOxidation of N-Acetyl Alanine by Chloramine-T in Presence of Hydrochloric Acid: A Kinetic and Mechanistic StudyCentral Asian StudiesNo ratings yet
- A Miracle of Flexibility and Fracture Resistance!: The New Niti File GenerationDocument6 pagesA Miracle of Flexibility and Fracture Resistance!: The New Niti File Generationshamshuddin patelNo ratings yet
- Eat Right For A Healthy Life (PE)Document15 pagesEat Right For A Healthy Life (PE)Yan100% (4)
- Solution Proposal Fleet ManagementDocument3 pagesSolution Proposal Fleet ManagementmasumidbNo ratings yet
- Bombas SumergiblesDocument79 pagesBombas SumergiblesInstinct_brNo ratings yet
- Reading b2 c1Document4 pagesReading b2 c1Karenza ThomasNo ratings yet
- Chiari ExerciseDocument3 pagesChiari ExercisesoliverosteopathyNo ratings yet