Download as pdf or txt
You might also like
- Janeway's Immunobiology 8thDocument892 pagesJaneway's Immunobiology 8thSergio Falcon Rivera92% (13)
- Childhood PsioriasisDocument6 pagesChildhood PsioriasisYuliana DaisongNo ratings yet
- Psoriasis: A Comprehensive Review: Nternational Ournal OF Harmacy & IFE CiencesDocument21 pagesPsoriasis: A Comprehensive Review: Nternational Ournal OF Harmacy & IFE Ciences24hintheghettoworkoutNo ratings yet
- Psoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsDocument21 pagesPsoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsMapsNo ratings yet
- Psoriasis - Systemic DiseaseDocument225 pagesPsoriasis - Systemic DiseaseShengping LUONo ratings yet
- Psoriasis: Incurable But Manageable: Luke Clews Principles of NaturopathyDocument3 pagesPsoriasis: Incurable But Manageable: Luke Clews Principles of Naturopathyglenn johnstonNo ratings yet
- 582 880 1 SMDocument11 pages582 880 1 SMJupiter CarlNo ratings yet
- Ethnopharmacological Studies of Argemone Mexicana For The Management of Psoriasis 300Document5 pagesEthnopharmacological Studies of Argemone Mexicana For The Management of Psoriasis 300Jitesh Kumar MaharanaNo ratings yet
- Homoeopathy in A Case of Palmo-Plantar Psoriasis: A Case ReportDocument5 pagesHomoeopathy in A Case of Palmo-Plantar Psoriasis: A Case ReportHomoeopathic PulseNo ratings yet
- SolDocument10 pagesSolTsigereda AberaNo ratings yet
- Behcet Disease AND Toxoplasmosis: by DR Shahzada Khan Tmo Eye A Ward HMCDocument67 pagesBehcet Disease AND Toxoplasmosis: by DR Shahzada Khan Tmo Eye A Ward HMCShahzada KhanNo ratings yet
- Psoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsDocument21 pagesPsoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsOktavianti Prisilia SoumokilNo ratings yet
- Case Report: Xanthoma Disseminatum With Tumor-Like Lesion On FaceDocument5 pagesCase Report: Xanthoma Disseminatum With Tumor-Like Lesion On FaceAgus SyaifudinNo ratings yet
- Ayurvedic Management of Psoriasis (Ek Kustha) - A Case StudyDocument8 pagesAyurvedic Management of Psoriasis (Ek Kustha) - A Case Studybhavana NandakumarNo ratings yet
- Ahri Proposal 2Document28 pagesAhri Proposal 2Tsigereda AberaNo ratings yet
- Psoriasis Case Presentation 2Document9 pagesPsoriasis Case Presentation 2conterNo ratings yet
- Dermatology D. Azr Lec2 Mon 18.10.2010: Papulosquamous DiseasesDocument9 pagesDermatology D. Azr Lec2 Mon 18.10.2010: Papulosquamous DiseasesMohamed Al-zichrawyNo ratings yet
- Thesis PsoriasisDocument4 pagesThesis PsoriasisDereck Downing100% (2)
- Case Report of Acne Vulgaris Edit 1Document18 pagesCase Report of Acne Vulgaris Edit 1Irwin FitriansyahNo ratings yet
- Psoriasis and Dermatitis AtopicDocument11 pagesPsoriasis and Dermatitis AtopicsayasajaNo ratings yet
- Ijms 20 01475 With CoverDocument29 pagesIjms 20 01475 With CoverJemini PereraNo ratings yet
- Psoriasis: PathophysiologyDocument23 pagesPsoriasis: PathophysiologyImran KhanNo ratings yet
- Psoriasis A Case StudyDocument14 pagesPsoriasis A Case StudyYayin PestañoNo ratings yet
- Staphylococcal Scalded Skin Syndrome in Child A CADocument6 pagesStaphylococcal Scalded Skin Syndrome in Child A CAsalshabilaNo ratings yet
- Stevens-Johnson Syndrome Induced by Carbamazepine: PharmacologyDocument4 pagesStevens-Johnson Syndrome Induced by Carbamazepine: PharmacologyginNo ratings yet
- Case ReportDocument12 pagesCase ReportRimueng GhuenNo ratings yet
- Psoriasis A Comprehensive Review On The AetiopathoDocument29 pagesPsoriasis A Comprehensive Review On The AetiopathoGregorius HocevarNo ratings yet
- 170 FullDocument4 pages170 FullRegita LatuihamalloNo ratings yet
- Systemic Lupus Erythematosus Discoid in Dog CanisDocument4 pagesSystemic Lupus Erythematosus Discoid in Dog CanisAlina BlondaNo ratings yet
- Psoriasis: Psoriasis Type of PsoriasisDocument18 pagesPsoriasis: Psoriasis Type of PsoriasisDeepikaNo ratings yet
- Psoriasis A Biological and Behavioral Management ApproachDocument5 pagesPsoriasis A Biological and Behavioral Management ApproachAthenaeum Scientific PublishersNo ratings yet
- Oral Manifestations of Behcet's Syndrome: Case ReportDocument6 pagesOral Manifestations of Behcet's Syndrome: Case Report24 februaryNo ratings yet
- Sjogren Syndrome A Case ReportDocument3 pagesSjogren Syndrome A Case ReportEditor IJTSRDNo ratings yet
- Psoriasis - StatPearls - NCBI BookshelfDocument8 pagesPsoriasis - StatPearls - NCBI BookshelfMehmet TaşçıNo ratings yet
- LuciophenomenonDocument6 pagesLuciophenomenonAdniana NareswariNo ratings yet
- Pathology Outlines - PsoriasisDocument1 pagePathology Outlines - PsoriasisCaryl DagamiNo ratings yet
- Faculty of Medicine: DR Archianda Arsad HakimDocument8 pagesFaculty of Medicine: DR Archianda Arsad HakimnikfarisNo ratings yet
- Papules On The Back: Figure 1a, BDocument3 pagesPapules On The Back: Figure 1a, BDwi Tantri SPNo ratings yet
- Herpes OdontalgiaDocument5 pagesHerpes OdontalgiaBramita Beta ArnandaNo ratings yet
- Erythroderma Caused Drug Allergies: Case ReportDocument7 pagesErythroderma Caused Drug Allergies: Case Report568563No ratings yet
- Patterns of Skin Disease and Prescribing Trends in Rural India Juno J. Joel, Neethu Jose, Shastry C.SDocument6 pagesPatterns of Skin Disease and Prescribing Trends in Rural India Juno J. Joel, Neethu Jose, Shastry C.SHabibur RahmanNo ratings yet
- Muco-Cutaneous & Aphthous UlcerDocument7 pagesMuco-Cutaneous & Aphthous Ulcerربيد احمد مثنى يحيى كلية طب الاسنان - جامعة عدنNo ratings yet
- Case Report: Lepra Reaction With Lucio Phenomenon Mimicking Cutaneous VasculitisDocument5 pagesCase Report: Lepra Reaction With Lucio Phenomenon Mimicking Cutaneous VasculitisadibahtiarNo ratings yet
- Herpes Zoster Thorakalis Th9Document13 pagesHerpes Zoster Thorakalis Th9Roby Syah Putra FirmansyahNo ratings yet
- Tugas Behcet SyndromDocument6 pagesTugas Behcet SyndromIsmy HoiriyahNo ratings yet
- 2545-Article Text-7661-1-10-20190414 PDFDocument6 pages2545-Article Text-7661-1-10-20190414 PDFClariza ZulyanNo ratings yet
- Therapy Selection For Tinea Corporis and Cruris With CommorbidityDocument9 pagesTherapy Selection For Tinea Corporis and Cruris With CommorbidityShimie Shimie KokobopNo ratings yet
- Background: Aphthous Ulcers UveitisDocument19 pagesBackground: Aphthous Ulcers UveitisCupris23No ratings yet
- Comorbidities in Psoriasis PDFDocument9 pagesComorbidities in Psoriasis PDFbogdansoroNo ratings yet
- Recent Insights Into The Immunopathogenesis of Psoriasis Provide New Therapeutic OpportunitiesDocument13 pagesRecent Insights Into The Immunopathogenesis of Psoriasis Provide New Therapeutic Opportunitiesraudhatul muttaqinNo ratings yet
- Psoriasis Research PaperDocument4 pagesPsoriasis Research Papervvjrpsbnd100% (1)
- 1 PBDocument6 pages1 PBdamayantiwenny24No ratings yet
- Case Report - PsoriasisDocument7 pagesCase Report - Psoriasisnathalia gabriellaNo ratings yet
- Serbian Association of Dermatovenereologists Guidelines For The Diagnosis and Treatment of PsoriasisDocument18 pagesSerbian Association of Dermatovenereologists Guidelines For The Diagnosis and Treatment of PsoriasisAndjela KosticNo ratings yet
- Jurnal Reading Glorivy Regita 112021072Document5 pagesJurnal Reading Glorivy Regita 112021072Regita LatuihamalloNo ratings yet
- Psoriasis NATURE AYFinlayDocument48 pagesPsoriasis NATURE AYFinlayMelly SyafridaNo ratings yet
- Behc Et's Disease Physiopathology: A Contemporary Review: DescriptionDocument12 pagesBehc Et's Disease Physiopathology: A Contemporary Review: Descriptionerma gusmayantiNo ratings yet
- Kuliah 4 B - PSORIASISDocument30 pagesKuliah 4 B - PSORIASISTimothy TobiasNo ratings yet
- Basic of AutoimmunityDocument13 pagesBasic of Autoimmunitymahadevabhu07100% (1)
- Presentation 3 (Information) Major Descending (Motor) Pathway and Spinal Cord Tracts March 25, 2012Document23 pagesPresentation 3 (Information) Major Descending (Motor) Pathway and Spinal Cord Tracts March 25, 2012bsittNo ratings yet
- Antigen - Antibody Reactions: Dr.D.BinduDocument46 pagesAntigen - Antibody Reactions: Dr.D.Bindubindu dhanapalNo ratings yet
- Molecules 28 05624Document30 pagesMolecules 28 05624Sayed Newaj ChowdhuryNo ratings yet
- Alphabetical Listing of CLSI Books0309Document15 pagesAlphabetical Listing of CLSI Books0309glodovichiNo ratings yet
- Intervenciones en Dermatitis Atópica CaninaDocument16 pagesIntervenciones en Dermatitis Atópica CaninaMaka.ibanezNo ratings yet
- Cellular AberrationsDocument94 pagesCellular AberrationsridzkhaNo ratings yet
- Brugia MalayiDocument8 pagesBrugia MalayiROn Ace DancelNo ratings yet
- Oms BookDocument292 pagesOms BookLUisNo ratings yet
- Carlos Simon, Antonio Pellicer-Stem Cells in Human Reproduction_ Basic Science and Therapeutic Potential, 2nd Edition (Reproductive Medicine & Assisted Reproductive Techniques)-Informa Healthcare (200Document273 pagesCarlos Simon, Antonio Pellicer-Stem Cells in Human Reproduction_ Basic Science and Therapeutic Potential, 2nd Edition (Reproductive Medicine & Assisted Reproductive Techniques)-Informa Healthcare (200yasirhistoNo ratings yet
- Textbook Therapy For Severe Psoriasis Jashin J Wu Ebook All Chapter PDFDocument53 pagesTextbook Therapy For Severe Psoriasis Jashin J Wu Ebook All Chapter PDFcalvin.price163100% (2)
- Report Regarding DepressionDocument18 pagesReport Regarding Depressiontech masterNo ratings yet
- Antimicrobial DrugsDocument20 pagesAntimicrobial Drugsmaria adventia martinNo ratings yet
- Stress Management Thru Sahaja Yoga (Always Free)Document19 pagesStress Management Thru Sahaja Yoga (Always Free)Vinay Singh100% (5)
- HCV Treatment RevolutionDocument3 pagesHCV Treatment RevolutionMai NabiehNo ratings yet
- Cells vs. Viruses Venn Diagram Sort: Interactive Notebooking ActivityDocument2 pagesCells vs. Viruses Venn Diagram Sort: Interactive Notebooking ActivityNellyRdzNo ratings yet
- MCQs From All Subjects For Medical PG EntranceDocument16 pagesMCQs From All Subjects For Medical PG EntranceEMIN3MNo ratings yet
- Protein BiosynthesisDocument33 pagesProtein BiosynthesisLucy WijayaNo ratings yet
- Vitamin DeficiencyDocument43 pagesVitamin DeficiencyAathi Pathmanathan100% (1)
- Cellometer Via Stain CS1 0108 5ML Product Insert Rev A PDFDocument4 pagesCellometer Via Stain CS1 0108 5ML Product Insert Rev A PDFDimasPrasetiantoWicaksonoNo ratings yet
- Dwnload Full Wheaters Basic Pathology A Text Atlas and Review of Histopathology 5th Edition Young Test Bank PDFDocument36 pagesDwnload Full Wheaters Basic Pathology A Text Atlas and Review of Histopathology 5th Edition Young Test Bank PDFasherharrisgdo3100% (12)
- Intraocular Pressure and Aqueous Humor DynamicsDocument36 pagesIntraocular Pressure and Aqueous Humor DynamicsIntan EkarulitaNo ratings yet
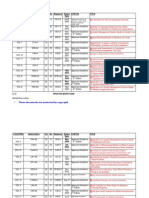
- Vitamin ChartDocument3 pagesVitamin ChartSrivani MamidishettyNo ratings yet
- Mesenchymal Stem Cells: From Biology To Clinical UseDocument10 pagesMesenchymal Stem Cells: From Biology To Clinical UseroyNo ratings yet
- The Regeneration of Human Limbs PDFDocument21 pagesThe Regeneration of Human Limbs PDFKeke MauroNo ratings yet
- Thirteenth Course "Clinical Cytogenetics", Goldrain Castle (BZ), ItalyDocument2 pagesThirteenth Course "Clinical Cytogenetics", Goldrain Castle (BZ), ItalyDoina Ababii UrsanNo ratings yet
- Muscle & MalocclusionDocument57 pagesMuscle & MalocclusionRazeev Mishra100% (1)
- DNADocument23 pagesDNAMuneeb Jan100% (1)
- Lung Cancer Presentation: DR Richard Sullivan and Ms Anne FraserDocument24 pagesLung Cancer Presentation: DR Richard Sullivan and Ms Anne FraseranggiNo ratings yet