Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NCP Cholecystectomy RevisedDocument7 pagesNCP Cholecystectomy RevisedMariquita Buenafe100% (4)
- Subdural HematomaDocument52 pagesSubdural HematomaanjarwatiNo ratings yet
- Health System Nutrition and DietDocument2 pagesHealth System Nutrition and DietMikaela LaoNo ratings yet
- Test Bank For Laboratory Manual For Seeleys Anatomy Physiology 11th Edition Eric Wise 3 DownloadDocument69 pagesTest Bank For Laboratory Manual For Seeleys Anatomy Physiology 11th Edition Eric Wise 3 Downloadcaseyyoungtoekwmcfdi100% (30)
- Denoising of ECG Signal For Detection and Classification of Arrhythmia in On-Line Patient MonitoringDocument31 pagesDenoising of ECG Signal For Detection and Classification of Arrhythmia in On-Line Patient MonitoringPratik SinghNo ratings yet
- Saudi Board of General Surgery Final Exam, November 2009 PDFDocument47 pagesSaudi Board of General Surgery Final Exam, November 2009 PDFRahmah Shah Bahai100% (2)
- The Nasal Septum PDFDocument18 pagesThe Nasal Septum PDFalit100% (1)
- Kimia KlinikDocument1 pageKimia KlinikOldi JunizarNo ratings yet
- Presentation CVADocument43 pagesPresentation CVAHenk Kraaijenhof100% (3)
- CollagenaseDocument3 pagesCollagenaseThivia RajNo ratings yet
- 20 Literasi Bahasa InggrisDocument14 pages20 Literasi Bahasa Inggriskeysakeysa739No ratings yet
- Use and Limitations of in Vitro Dissolution Testing: Topic Introduction and OverviewDocument114 pagesUse and Limitations of in Vitro Dissolution Testing: Topic Introduction and OverviewMuthu Venkatesh100% (1)
- ThrombocytopeniaDocument49 pagesThrombocytopeniaMaria EnjelinaNo ratings yet
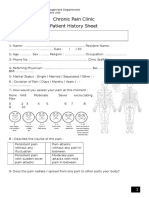
- Chronic Pain Clinic Patient History SheetDocument4 pagesChronic Pain Clinic Patient History SheetBelal N. MahfouzNo ratings yet
- Alpina, Eurycoma Longifolia, and Curcuma Xanthorrhiza) Increases Number and ImprovesDocument6 pagesAlpina, Eurycoma Longifolia, and Curcuma Xanthorrhiza) Increases Number and ImprovesedwardNo ratings yet
- Gordon's FormDocument6 pagesGordon's FormHarry AglugobNo ratings yet
- Breathing TheoryDocument3 pagesBreathing TheoryNicolás LowryNo ratings yet
- Central DogmaDocument50 pagesCentral DogmaIvilyn ManguladNo ratings yet
- Drop MethodDocument2 pagesDrop MethodCharlene Bularan100% (2)
- Pancuronium: "Pavulon - Bromurex"Document33 pagesPancuronium: "Pavulon - Bromurex"Bahaa ShaabanNo ratings yet
- The Healing Power of HumorDocument3 pagesThe Healing Power of HumorJuan Daniel Yanqui GuerreroNo ratings yet
- BP201TPDocument1 pageBP201TPDarshanNo ratings yet
- 5ykgogrgmtd3pwbpedotjsidDocument10 pages5ykgogrgmtd3pwbpedotjsidKartik SharmaNo ratings yet
- Flow Sheet TemplateDocument4 pagesFlow Sheet TemplateIulia Tania AndronacheNo ratings yet
- Heart MurmursDocument7 pagesHeart MurmursOffvb MednuNo ratings yet
- Silverthorne 2018-Learning by Osmosis An Approach To Teaching Osmolarity and TonicityDocument10 pagesSilverthorne 2018-Learning by Osmosis An Approach To Teaching Osmolarity and TonicityIlham NugrohoNo ratings yet
- Adrenocortical AgentsDocument14 pagesAdrenocortical AgentsFredie O HadjimudinNo ratings yet
- Answers: CHAPTER 1 Stimuli and ResponsesDocument22 pagesAnswers: CHAPTER 1 Stimuli and Responses林柄洲No ratings yet
- Citrate Anticoagulation During CRRTDocument12 pagesCitrate Anticoagulation During CRRTpmunizNo ratings yet
- IronGAINS How To Get Strong & Muscular - Ebook 1st Edition - CompressedDocument289 pagesIronGAINS How To Get Strong & Muscular - Ebook 1st Edition - CompressedJames Khanso100% (1)