Dr Tim Sandle, UK Bio Products Laboratory
AIR PURIFICATION
CLEANROOMS AND CLEAN AIR
The importance of air handling and HEPA ltration
From the wear and tear of the HVAC system
Cleanrooms are highly controlled environments where the air quality is monitored to ensure the extreme standards of cleanliness required for surgical units and for hospital pharmacies.
A cleanroom is as a specially designed room in which the concentration of airborne contamination is controlled, and which is constructed and used in a manner to minimise the introduction, generation and retention of particles inside the room and in which other important parameters, such as pressure, temperature and humidity are controlled1. In order to supply cleanrooms with clean, high fresh air rates, extensive filtering, temperature and humidity control are required. The supply of clean air to cleanrooms, and the control of the parameters of temperature, humidity and pressure, is through HVAC (Heating Ventilation and Air Conditioning) systems (sometimes called air handling systems). A fundamental part of the HVAC system are the specially designed filters, termed HEPA (High Efficiency Particulate Air) filters, which are designed to reduce the number of microorganisms and other particles down to an appropriate level of cleanliness. This article examines how air handling systems and HEPA filters work and discusses some of the important tests required in order to verify systems to demonstrate that they continue to work efficiently and keep cleanrooms clean.
Generated by personnel working within the cleanroom Although air is a source of contamination, however, microorganisms do not grow and increase in numbers in air and most microorganisms find it hard to survive in air because the environment desiccates them, and also because of the exposure to ultraviolet radiation. Thus the risk to cleanrooms is from those microorganisms in the air settling onto critical surfaces. Although air is a contamination source, air is also the answer to many contamination problems. There are four principles which apply to the control of airborne contamination in cleanrooms. These are: Filtration: cleanrooms need to be designed so that most of the contamination in the air is filtered out Dilution: cleanrooms need to be supplied with a sufficient volume of fresh air at regular intervals so that any contamination generated by people working in the room is at first diluted and then removed from the room. This is achieved by having a set number of air changes per hour. The minimum requirement is normally 20 air changes per hour; that is, the room air volume is replaced every three minutes
Contamination control and airflow
Before examining air handling systems and HEPA filters it is important to review cleanroom contamination. Contamination control is the primary consideration in cleanroom design2; however, the relationships between contamination control and airflow are not well understood. Supplying cleanrooms with clean air, through HEPA filters, means that most cleanrooms are supplied with clean air. Contaminants in cleanrooms, such as particles or microorganisms, are primarily introduced to cleanrooms by people, although processes in cleanrooms may also introduce contamination3. With contamination present in cleanrooms, the supply of clean air is necessary in order to remove contamination through the replacement of the room air volume with clean air. There are three ways in which particles could get into a cleanroom: From outside air even in the countryside, away from factories, air contains approximately 108 particles of 0.5m size and greater per cubic metre
19
January 2012
17
AIR PURIFICATION
maintained at appropriate levels. In addition, the air must be filtered and for this the cleanroom requires appropriate HEPA (high efficiency particulate air) systems. The HVAC system operates on the basis of mechanical ventilation. An example of the air supply is illustrated in Figure 1. Air handling units consist of filters, coils and fans in a metal casing, with an insulation liner applied to the inside of the casing. For healthcare applications the unit casing must be a double skin sandwich of metal with insulation between the metal sheets to provide a smooth, cleanable interior surface that does not foster the growth of microorganisms. The two most important elements are the fans, which control the air speed, and the HEPA filters.
High efficiency particulate air filters
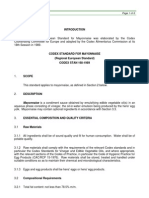
a) How HEPA filters work The HEPA filter is a fundamental part of the HVAC system. The filters are designed to control the number of particles entering a clean area by filtration. HEPA filters function through a combination of three important aspects. First, there are one or more outer filters that work like sieves to stop the larger particles of dirt, dust, and hair. Inside those filters, there is a concertina a mat of very dense fibres arranged in a random order. The fibres are normally made from fibreglass. The function of the fibres is to trap smaller particles. The inner part of the HEPA filter catches particles as they pass through in the moving air stream, through three mechanisms: Interception. For this, particles following a line of flow in the air stream come within one radius of a fibre and adhere to it Impaction. Here, larger particles are unable to avoid fibres by following the curving contours of the air stream and are forced to embed in one of them directly; this effect increases with diminishing fibre separation and higher air flow velocity Diffusion. Here, smaller particles are impeded by colliding with gas molecules which impedes the movement of the particles These concepts are illustrated in Figure 2.
Figure 1 - Typical air ventilation supply
Directional Air Flow: for ultra-clean activities, undertaken in unidirectional airflow cabinets operating at EU and WHO Grade A (ISO class 5), the air needs to move in a straight direction so that any contamination generated within the area is removed. This is achieved by having the air enter at a high velocity normally at 0.45 metres per second 20% Air Movement: the air within cleanrooms needs to keep moving so that any contamination remains suspended in the air rather than being allowed to settle onto surfaces. This is achieved by having unidirectional or turbulent airflow
Heating ventilation and air conditioning
The key design consideration for the cleanroom is the HVAC (Heating Ventilation and Air Conditioning) system. HVAC systems were first designed by mechanical engineers for the electronics industry and for the manufacture of aircraft parts in World War II. Post war, the application of HVAC to provide clean air was orientated towards the healthcare and pharmaceutical sectors. The functions of HVAC are: To heat the air To supply ventilation the process of replacing air in a room in order to remove heat, dust, and airborne bacteria To condition air this involves the control of humidity (dehumidification) or the removal of heat to cool the air to required level Maintain room pressure (delta P) areas that must remain cleaner than surrounding areas must be kept under a positive pressurisation (a concept examined below) In conjunction with HEPA filters, to control airborne particulates and microorganisms For healthcare cleanrooms airflow and air changes must be controlled, and the temperature and humidity of the air Filter class H 10 H 11 H 12 H 13 H 14 U 15 U 16 U 17
Overall value efficiency (%) 85 95 99.5 99.95 99.995 99.9995 99.99995 99.999995
Overall Value Penetration (%) 15 5 0.5 0.05 0.005 0.0005 0.00005 0.000005
Leak test efficiency (%) 99.75 99.975 99.9975 99.99975 99.9999
Leak test penetration (%) 0.25 0.025 0.0025 0.00025 0.0001
Table 1 - Classification of air filters based on standard EN 18224
January 2012
20
AIR PURIFICATION
b) Standards for HEPA filters There are different grades of HEPA filters based on their efficiency ratings. These are shown in Table 1. There is a second type of filter called a ULPA (Ultra Low Penetration Air) filter. These filters are capable of a far greater particle reduction than HEPA filters. They are expensive to operate, however, and tend to be used more often in the manufacture of electronic circuits. The type of filter purchased depends upon the requirement of the facility. Most healthcare facilities use H13 or H14 HEPA filters. Arguably the most important parameter of a HEPA filter is the efficiency value. This determines how many particles the HEPA filter will theoretically let pass through into a cleanroom. This is based on the theoretical assumption that if 1,000 particles of a size of 0.3 m size are challenged to the filter then only x number will pass through. An H13 rated filter, for example, is capable of filtering out 99.97% particles of 0.3 m or larger. c) Positioning HEPA filters Most HEPA filters are ceiling mounted, which allows the HEPA filters to supply air with sufficient velocity and volume to unidirectional sweep over the critical areas. Sometimes HEPA filters are located lower down within walls, although in general this makes the filters less efficient at distributing the airflow. See Figure 3 d) Modification of HEPA filters
Air handing systems and HEPA filters also reduce contamination through air movement. The cleanroom air flow pattern should be designed to provide sufficient air to constantly cover all critical areas where risk is high particularly where the patient or product is exposed. The physical bathing of the critical areas with the filtered air acts as a shield to help prevent contaminates from reaching the exposed products. Ceiling mounted HEPA filters can supply air with sufficient velocity and volume to unidirectional sweep over the critical areas. It is typical for air handling systems to provide sufficient air volume to allow multiple complete air changes in the cleanroom. This flushes the room with filtered air and functions to continually remove potential contaminants that may enter or accumulate in the room during normal use. The number of air changes required for cleanrooms where a product is exposed is often sited to a minimum standard not less than 20 air changes per hour, but in practice it is common to see cleanrooms designed to provide a much higher number of air changes.
Interception
For some healthcare applications greater assurance that pathogens have been removed from the air supply is required. For this, ultraviolet (UV) lighting is used. The total power of the UV lamp is a product to the power of the light source multiplied by the exposure time. A typical specification for a UV light is a 254 nanometer wavelength UV light operating at 6,500 mW /cm2.
Impaction
Diffusion
Function of air handling systems and HEPA filters for contamination control
The key function of HEPA filters is air filtration. Filtration removes particles and microorganisms. Although HEPA filters are efficient at removing particles, they need to be protected from blockage by pre-filters, otherwise the life span of the HEPA filter would be relatively short. Pre-filters remove up to about 90% of particles from air5. To illustrate the importance of pre-filters, if air contains about 3 x 108 particles per m3, and there is one pre-filter and one HEPA filter, the pre-filter removes a sufficient number of particles to leave about 3 x 107 per m3 as a challenge to the HEPA filter. The terminal HEPA filter will leave about 103 per m3 to enter the cleanroom. This is a relatively low number and is within the limits for EU and WHO GMP Grade A (ISO class 5) and Grade B (ISO class 7). In fact, most air handling systems recirculate up to 80% of the air supplied to cleanrooms. Therefore the initial challenge to the HEPA filters is probably only about 106 particles per m3. So in practice there is normally no more than 3 x 102 particles per m3 supplied to pharmaceutical cleanrooms. This level is even further within the required limits.
Figure 2 - Illustration of the concepts of interception, impaction and diffusion in relation to HEPA filters
Structural slab
Inlet duct
Gaskets
HEPA Filter Integrity test probe Seals False ceiling
Figure 3 - HEPA filter
21
January 2012
21
AIR PURIFICATION
Most cleanrooms are of the turbulent air flow type. Here, air is driven in through grilles and ducts at ceiling height and removed through low level ducts. While the air is in the room its initial supply velocity is sufficient to keep it in constant turbulence, which prevents particles and microorganisms from settling settle out. This is an ideal because dead air can occur beneath objects such as tables. It is important to know where dead areas occur these can be shown through airflow visualisation studies using smoke. If they cannot be avoided then monitoring should be targeted at these locations.
critical operations are being performed. Values of 10-15 Pascal between rooms of different grades are typical. The way in which the dirty air is prevented from entering the cleanroom is by ensuring a very high rate of air supply to the cleanroom, thus keeping it at a higher pressure than its surroundings. If there is contact with outside air, any mixing of the two types of air takes place outside the cleanroom because the direction of air flow is from the clean to the dirty area. This directional air flow is measured and monitored through pressure differentials. Thus air will always move from an area where it is at a high pressure to one where there is a low pressure this is due to a Law of Physics. Particles and microorganisms cannot swim upstream against a directional air flow.
particles and microorganisms cannot swim upstream against a directional air ow
The amount of air supplied and exhausted in a cleanroom compared to that supplied to the adjacent rooms is also used to create a pressure differential cascade between the cleanroom and the surrounding rooms. This is an essential function to control contamination entering from room to room together with materials and personnel. The pressure cascade should be designed to have a higher pressure where the more
Routine monitoring
In order to ensure that control measures are being maintained and to examine the status of the cleanroom, the air handling system must be monitored closely and maintained regularly. This includes routine monitoring of particulates using optical particle counters; viable (microbial) environmental
January 2012
22
AIR PURIFICATION
monitoring using methods which employ a microbiological agar culture medium; assessing differential pressures; and examining the parameters of temperature and relative humidity6.
Summary
This article has outlined the importance of the supply of clean air to cleanrooms and has discussed the importance of HEPA filters in achieving this clean air supply. For users of cleanrooms it is important to specify the types of air handling systems and HEPA filters required and to ensure that the cleanroom is designed in an appropriate way. Once established, regular performance checking and annual calibration is required in order to maintain control.
Annual verification
In order to ensure that HVAC systems continue to work effectively, annual testing the HEPA filters (e.g. integrity-leak tests, air velocity) and air flow patterns via smoke tests are essential parts of the regular maintenance of the air handling system. Other tests include: assessing the air stream velocity under each filter panel; taking airflow measurements at the supply, return and exhaust outlets; particulate testing of the cleanroom to show that the system can deliver air of appropriate quality; measuring pressure differentials between the cleanroom and adjacent areas; assessing the pressure drop across the final filters and recording room temperatures and relative humidity.
References
1. ISO 14644-1: Cleanrooms and associated controlled environments - Part 1: Classification of air cleanliness. International Organization for Standardization ISO, Geneva (May 1999) 2. Ljungqvist B., Reinmller Berit: Cleanroom design - Minimizing contamination through proper design. Interpharm Press, Buffalo Grove IL/ USA (1997). 3. Austin Ph.R.: People generated contamination. Journal of the American Association of Contamination Control 5 (1966) no. 1. 4. EN 1822: High efficiency particulate air filters (EPA, HEPA and ULPA): Part 1 - Classification, performance testing and marking; Part 2 - Aerosol production, measuring equipment, particle counting statistics; Part 3 Testing flat sheet filter media; Part 4 - Determining leakage of filter elements (scan method); Part 5 - Determining the efficiency of filter elements. Idem, ibid. (Nov. 2009). 5. Jarmey-Swan, C. Filtration. [ed.] Norman Hodges and Geoff Hanlon. Industrial Pharmaceutical Microbiology Standards & Controls. Haslemere : Euromed Communications, 2008, S7. 6. Sandle, T. (2011): Environmental Monitoring in Saghee, M.R., Sandle, T. and Tidswell, E.C. (Eds.) (2011): Microbiology and Sterility Assurance in Pharmaceuticals and Medical Devices, New Delhi: Business Horizons, pp293-326
regular performance checking and annual calibration is required in order to maintain control
The main failure risk is from leaks, where the concern is with pinhole leaks in the HEPA filter media, across sealants and frame gaskets, supporting frame and wall. A leak would allow a higher concentration of particles to enter the cleanroom. To check their effectiveness they are checked for leaks by challenging the filters with a particle generating substance (an aerosol challenge, for example Di-octyl phtalate [DOP] or Shell Ondino mineral oil) and measuring the efficiency of the filter. Leakage is assessed using an aerosol photometer. The aerosol photometer has to be fixed in a way to be able to measure the concentration of aerosol in front of and behind the filter. A photometer assesses the HEPA filter by taking a sample of the air at the filter downstream. When particles pass through a special light within the photometer, they reflect the light and this light passes through lenses and through a photomultiplier where the light is converted into electric signal. The result is the higher the number of particles the stronger the signal. The photometers usually measure the concentration of aerosol from 0.0001 g/l to 100 g/l the instrument functions by measuring the weight of particles rather than counting the actual number.
Author
Dr Tim Sandle is a chartered biologist and has worked for various healthcare and pharmaceutical organisations. Dr Sandle is an honorary consultant with the University of Manchester. In addition, he serves on several international committees relating to pharmaceutical microbiology and cleanroom contamination control. Dr Sandle has written more than 100 book chapters, peer reviewed papers and technical articles relating to microbiology. He is co-editor of the comprehensive book Microbiology and Sterility Assurance in Pharmaceuticals and Medical Devices. Dr. Sandle has also delivered papers to more than 40 international conferences. Dr Sandle operates a microbiology and healthcare blog http://www.pharmig.blogspot.com He can be contacted at: timsandle@btinternet.com
25
January 2012
21
You might also like
- Biotechnology: From Idea To MarketDocument4 pagesBiotechnology: From Idea To MarketTim Sandle100% (1)
- Cleanroom Contamination Prevention & Control: A Practical Guide To The ScienceDocument13 pagesCleanroom Contamination Prevention & Control: A Practical Guide To The ScienceTim Sandle56% (9)
- Contamination Control in Healthcare Product Manufacturing, Volume 4Document2 pagesContamination Control in Healthcare Product Manufacturing, Volume 4Tim Sandle0% (1)
- Aseptic and Sterile Processing: Control, Compliance and Future TrendsDocument2 pagesAseptic and Sterile Processing: Control, Compliance and Future TrendsTim Sandle100% (1)
- Cleanroom Performance Testing Specifications - Bio-Medical PharmaceuticalDocument18 pagesCleanroom Performance Testing Specifications - Bio-Medical PharmaceuticalginnaNo ratings yet
- Conducting Compliant InvestigationsDocument10 pagesConducting Compliant InvestigationsTim Sandle100% (1)
- Digital Transformation in Pharmaceuticals and HealthcareDocument1 pageDigital Transformation in Pharmaceuticals and HealthcareTim Sandle100% (1)
- Digital Transformation of Pharmaceuticals (New Book)Document2 pagesDigital Transformation of Pharmaceuticals (New Book)Tim SandleNo ratings yet
- Publications by Tim Sandle - July 2019Document53 pagesPublications by Tim Sandle - July 2019Tim SandleNo ratings yet
- Aseptic and Sterile Processing: Control, Compliance and Future TrendsDocument1 pageAseptic and Sterile Processing: Control, Compliance and Future TrendsTim SandleNo ratings yet
- Data Integrity BookDocument2 pagesData Integrity BookTim Sandle100% (1)
- Codex Standar MayyonaiseDocument6 pagesCodex Standar MayyonaiseTaufiksyaefulmalik100% (1)
- Hot Work: Standard Operating ProceduresDocument4 pagesHot Work: Standard Operating Proceduresdroffilcz27No ratings yet
- D B I C: Clean Air Technology, Inc. Esigns, Uilds and Nstalls LeanroomsDocument2 pagesD B I C: Clean Air Technology, Inc. Esigns, Uilds and Nstalls LeanroomsRajeshNo ratings yet
- 2.4 Cleanrooms and Air Quality - A Risk-Based ApproachDocument13 pages2.4 Cleanrooms and Air Quality - A Risk-Based ApproachJorge Humberto HerreraNo ratings yet
- Designing Clean Room HVAC SystemsDocument10 pagesDesigning Clean Room HVAC Systemssushant_jhawerNo ratings yet
- HVAC Design For Pharmaceutical Facilities Course NoDocument24 pagesHVAC Design For Pharmaceutical Facilities Course NoLouay GhonaymNo ratings yet
- Calculating Clean Room CleanlinessDocument3 pagesCalculating Clean Room CleanlinessThanh NhatNo ratings yet
- HEPA Cleanroom Filter Testing PDFDocument4 pagesHEPA Cleanroom Filter Testing PDFprovaoralNo ratings yet
- 2002 07 08 - Airflow Management & Control in Pharmaceutical HVAC ApplicationsDocument12 pages2002 07 08 - Airflow Management & Control in Pharmaceutical HVAC ApplicationsHubert BonamisNo ratings yet
- Usp 797GCDocument61 pagesUsp 797GCAwni1989No ratings yet
- What Is A Cleanroom - Cleanroom ClassificationsDocument2 pagesWhat Is A Cleanroom - Cleanroom ClassificationsMai Phuong Phan TranNo ratings yet
- Presentation - NEBBDocument7 pagesPresentation - NEBBBhavik Thakar100% (1)
- Basic Requirements For Clean RoomDocument6 pagesBasic Requirements For Clean Roomsamuel debebeNo ratings yet
- HEPA Filter Testing - IssuesDocument3 pagesHEPA Filter Testing - Issueszivko13No ratings yet
- Duct Leakage TestingDocument4 pagesDuct Leakage TestingAbd Elhaleem RabeaNo ratings yet
- 2 Understanding Cleanroom Classification PDFDocument22 pages2 Understanding Cleanroom Classification PDFTECHNO DATENo ratings yet
- Air Handling UnitDocument3 pagesAir Handling UnitPrince Moni100% (2)
- CLEAN ROOM PresentationDocument54 pagesCLEAN ROOM PresentationSanjay Gade100% (1)
- Low RH Design Guide For Pharmaceutical IndustryDocument93 pagesLow RH Design Guide For Pharmaceutical IndustryMHNAD100% (1)
- Airflow Design For Clean Rooms and Its Economic ImplicationsDocument7 pagesAirflow Design For Clean Rooms and Its Economic ImplicationsDanny D.No ratings yet
- DOP BasicsDocument1 pageDOP BasicsRamesh KanalNo ratings yet
- Ash Rae Clean Room Design Guide Content DraftDocument6 pagesAsh Rae Clean Room Design Guide Content DraftQuan TranNo ratings yet
- HTTP WWW - Bryair.com Manuals Man07Document17 pagesHTTP WWW - Bryair.com Manuals Man07rama deviNo ratings yet
- HEPA and ULPA Filters: The Aseptic CoreDocument7 pagesHEPA and ULPA Filters: The Aseptic CoreVaidhyanadhan DeepakNo ratings yet
- Apparel Considerations For Clean ManufacturingDocument2 pagesApparel Considerations For Clean ManufacturingGaurav ShakyaNo ratings yet
- Tabb PDFDocument7 pagesTabb PDFFsNo ratings yet
- Percent Outdoor Air (%OA) Calculation and Its Use: Application NoteDocument7 pagesPercent Outdoor Air (%OA) Calculation and Its Use: Application NoteAce Glen GarciaNo ratings yet
- Fundamental of CGMP For Pharmaceutical Hvac SystemDocument41 pagesFundamental of CGMP For Pharmaceutical Hvac SystemRamy MahmoudNo ratings yet
- Hvac & Personnel Facilities: Heating, Ventilating & Air-Conditioning SystemDocument34 pagesHvac & Personnel Facilities: Heating, Ventilating & Air-Conditioning Systemخبراء التصنيع الدوائي-اليمنNo ratings yet
- (Heating Ventilation & Air Conditioning System) : Career Scope Course HighlightsDocument2 pages(Heating Ventilation & Air Conditioning System) : Career Scope Course HighlightsMilind KshirsagarNo ratings yet
- Excel Clean Room TechnologiesDocument9 pagesExcel Clean Room Technologiesxlcleantech100% (2)
- A Low-Cost, High Performance Lab HVAC DesignDocument4 pagesA Low-Cost, High Performance Lab HVAC Designhtosar2No ratings yet
- Cleanroom Flow ChartDocument1 pageCleanroom Flow Chartjirt2011No ratings yet
- Clean Room SpecificationsDocument4 pagesClean Room Specificationsminimoy86No ratings yet
- Airborne Particulate Cleanliness ClassesDocument4 pagesAirborne Particulate Cleanliness ClassesaKureishiNo ratings yet
- Federal Standard 209E Airborne Particulate Cleanliness Classes in Cleanrooms and Clean ZonesDocument56 pagesFederal Standard 209E Airborne Particulate Cleanliness Classes in Cleanrooms and Clean ZonesHassan HoudoudNo ratings yet
- ECA Clean Rooms HVAC SystemsDocument4 pagesECA Clean Rooms HVAC SystemsMac Nyandoro0% (1)
- 093 Paint Booth VentDocument3 pages093 Paint Booth VentFajar Hadi CrisnamurtiNo ratings yet
- Combustible Dust PosterDocument1 pageCombustible Dust PosterEvert W. VanderBergNo ratings yet
- Hospital Pharmacy Assignment Submitted To: DR Zubair Malik Submitted By: Ansar Mushtaq (20) Topic of AssignmentDocument9 pagesHospital Pharmacy Assignment Submitted To: DR Zubair Malik Submitted By: Ansar Mushtaq (20) Topic of AssignmentAnsar MushtaqNo ratings yet
- Clean Rooms L Essentiel 3Document4 pagesClean Rooms L Essentiel 3Sweekar BorkarNo ratings yet
- CLEAN ROOM DESIGN - CASE STUDY Zbook - 2017Document30 pagesCLEAN ROOM DESIGN - CASE STUDY Zbook - 2017ton_bela4911100% (1)
- En 1822 Epa, Hepa and Ulpa TestingDocument7 pagesEn 1822 Epa, Hepa and Ulpa TestingSteven HungNo ratings yet
- HVAC Rev1Document54 pagesHVAC Rev1Blank SermNo ratings yet
- Desiccant Dehumidifier ML1100Document2 pagesDesiccant Dehumidifier ML1100blackfzoneNo ratings yet
- CDA Clean Dry AirDocument15 pagesCDA Clean Dry AirJonNo ratings yet
- Aseptic FillingDocument5 pagesAseptic FillingMIKENo ratings yet
- Hepa Filter Product-SummaryDocument8 pagesHepa Filter Product-Summaryphase_shekhar21No ratings yet
- CEN LSC AMER 5 Rules of Sensor Placement B211369EN ADocument11 pagesCEN LSC AMER 5 Rules of Sensor Placement B211369EN AmajaNo ratings yet
- Vaisala On-Demand Webinar:: Listen To The Recording atDocument46 pagesVaisala On-Demand Webinar:: Listen To The Recording atMohammad IsmailNo ratings yet
- Microbiology Clean Room Design SpecificationDocument2 pagesMicrobiology Clean Room Design SpecificationMHNADNo ratings yet
- Introduction To Pharmaceutical Clean Room 1Document61 pagesIntroduction To Pharmaceutical Clean Room 1Abdul KalimNo ratings yet
- FAQ HEPAs and ULPAs Technical Bulletin - Parte2Document1 pageFAQ HEPAs and ULPAs Technical Bulletin - Parte2Nicolás VargasNo ratings yet
- Pharmaceutical AAF 1 206Document20 pagesPharmaceutical AAF 1 206Bader ShrbajiNo ratings yet
- About Air PurifiersDocument51 pagesAbout Air PurifierspempekplgNo ratings yet
- Integrity Testing of HEPA FiltersDocument3 pagesIntegrity Testing of HEPA FilterspradeepNo ratings yet
- Cleanrooms & Air Quality - A Risk-Based Approach - Tim SandleDocument13 pagesCleanrooms & Air Quality - A Risk-Based Approach - Tim SandleHubert BonamisNo ratings yet
- Cleanrooms and Air Quality A Risk BasedDocument13 pagesCleanrooms and Air Quality A Risk BasedwilyNo ratings yet
- Perfect Air-Interview Round 2 Case Study With Solution: Hvac Heating Ventilation and Air ConditioningDocument7 pagesPerfect Air-Interview Round 2 Case Study With Solution: Hvac Heating Ventilation and Air ConditioningMd TanveerNo ratings yet
- Air Cleaners, High-Efficiency Filter - 070413064320Document7 pagesAir Cleaners, High-Efficiency Filter - 070413064320Arshad NazarNo ratings yet
- Publications by Tim Sandle - 5th EditionDocument92 pagesPublications by Tim Sandle - 5th EditionTim SandleNo ratings yet
- An Interview With DR Tim Sandle - March 2019Document4 pagesAn Interview With DR Tim Sandle - March 2019Tim Sandle100% (1)
- Digital Transformation and Regulatory Considerations For Biopharmaceutical and Healthcare Manufacturers Volume 1 Digital Technologies For Automation and Process ImprovementDocument8 pagesDigital Transformation and Regulatory Considerations For Biopharmaceutical and Healthcare Manufacturers Volume 1 Digital Technologies For Automation and Process ImprovementTim SandleNo ratings yet
- Pharmaceutical Microbiology NewsletterDocument12 pagesPharmaceutical Microbiology NewsletterTim SandleNo ratings yet
- NOW IS THE TIME For Animal Welfare in PharmaDocument2 pagesNOW IS THE TIME For Animal Welfare in PharmaTim SandleNo ratings yet
- Audit and Control For Healthcare Manufacturers: A Systems-Based ApproachDocument13 pagesAudit and Control For Healthcare Manufacturers: A Systems-Based ApproachTim Sandle100% (1)
- Audit and Control For Healthcare Manufacturers: A Systems-Based ApproachDocument13 pagesAudit and Control For Healthcare Manufacturers: A Systems-Based ApproachTim Sandle100% (1)
- Real-Time Mycoplasma Contamination Detection For BiomanufacturingDocument3 pagesReal-Time Mycoplasma Contamination Detection For BiomanufacturingTim SandleNo ratings yet
- Biocontamination Control For Pharmaceuticals and HealthcareDocument2 pagesBiocontamination Control For Pharmaceuticals and HealthcareTim Sandle100% (1)
- Cleanroom Management (2017 Ed)Document1 pageCleanroom Management (2017 Ed)Tim Sandle50% (2)
- Cleaning and CleanroomsDocument7 pagesCleaning and CleanroomsTim SandleNo ratings yet
- Pharmigs 26th Annual Conference Programme Interactive 2018 FinalDocument8 pagesPharmigs 26th Annual Conference Programme Interactive 2018 FinalTim SandleNo ratings yet
- Burkholderia Cepacia Complex: Characteristics, Products Risks and Testing RequirementsDocument17 pagesBurkholderia Cepacia Complex: Characteristics, Products Risks and Testing RequirementsTim Sandle100% (1)
- PDA Bookstore ESeries Flyer - OrderformDocument2 pagesPDA Bookstore ESeries Flyer - OrderformTim SandleNo ratings yet
- CleanroomMicrobiology Flyer Order FormDocument2 pagesCleanroomMicrobiology Flyer Order FormTim SandleNo ratings yet
- The New Concept of Automatic Gloved Hand SanitizationDocument3 pagesThe New Concept of Automatic Gloved Hand SanitizationTim SandleNo ratings yet
- Publications by Tim Sandle (3rd Revision)Document42 pagesPublications by Tim Sandle (3rd Revision)Tim SandleNo ratings yet
- Products For Microbiological ControlDocument120 pagesProducts For Microbiological ControlTim Sandle100% (2)
- PDA Europe Microbiology Conference 2017Document18 pagesPDA Europe Microbiology Conference 2017Tim SandleNo ratings yet
- CleanroomMicrobiology Flyer Order FormDocument2 pagesCleanroomMicrobiology Flyer Order FormTim SandleNo ratings yet
- Mulusew PROJECTDocument29 pagesMulusew PROJECTHenok Bedilu0% (2)
- Ammonia Vapor Test For Determining Susceptibility To Stress Corrosion Cracking in Copper AlloysDocument4 pagesAmmonia Vapor Test For Determining Susceptibility To Stress Corrosion Cracking in Copper AlloysDanZel DanNo ratings yet
- DIOM Tyco Hygood IG541Document103 pagesDIOM Tyco Hygood IG541appril26No ratings yet
- CDL Florida Air Brake TestDocument14 pagesCDL Florida Air Brake TestBlagota DjukanovicNo ratings yet
- Lecture Notes Rebreather SCUBA DesignDocument10 pagesLecture Notes Rebreather SCUBA DesignAngel MosesNo ratings yet
- Zheng Fei Zhen Guo2003 Article IdentificationOfThePrecipitateDocument6 pagesZheng Fei Zhen Guo2003 Article IdentificationOfThePrecipitatePraveen CNo ratings yet
- Msds Karbol WangiDocument3 pagesMsds Karbol Wangiqaktj agustus22No ratings yet
- Blood Glucose Monitoring SystemDocument17 pagesBlood Glucose Monitoring SystemhardikdeekshaNo ratings yet
- Rate Factors LabDocument4 pagesRate Factors LabAadilNo ratings yet
- List Harga Per Agustus 2022Document21 pagesList Harga Per Agustus 2022nskhldNo ratings yet
- Basf Masterseal 725hc TdsDocument2 pagesBasf Masterseal 725hc TdsshashiNo ratings yet
- Polymer-Solute Complexation, Ov. 8 - AShDocument7 pagesPolymer-Solute Complexation, Ov. 8 - AShSara AlrubaiiNo ratings yet
- Bochure Catalase Enzyme Test PDFDocument2 pagesBochure Catalase Enzyme Test PDF08-Pimlada JakpingNo ratings yet
- Billet Defects 1Document7 pagesBillet Defects 1Vi KraNo ratings yet
- Assignment On Orsat's ApparatusDocument9 pagesAssignment On Orsat's ApparatusK SachinNo ratings yet
- Casing Attachment EquipmentDocument61 pagesCasing Attachment EquipmentDoni KurniawanNo ratings yet
- 07 Apr 2018 1600009675JRMYML2PFRBluetronFinal PDFDocument50 pages07 Apr 2018 1600009675JRMYML2PFRBluetronFinal PDFBimo Ary Pujangga PutraNo ratings yet
- High Pressure EquipmentDocument38 pagesHigh Pressure EquipmentAdhie WaelacxhNo ratings yet
- Content: Standard Operating Procedure (SOP) Use and Maintenance of An AutoclaveDocument10 pagesContent: Standard Operating Procedure (SOP) Use and Maintenance of An Autoclaverijulesh karmelNo ratings yet
- Biochem Lab Practice Exam PDFDocument9 pagesBiochem Lab Practice Exam PDFcanalescp9No ratings yet
- Sec 4.13 - Hydrolysis (Notes) : Group 1 (Alkali Metal Ions) Eg. Li Group 2 (Alkaline Earth Ions) Eg. BeDocument15 pagesSec 4.13 - Hydrolysis (Notes) : Group 1 (Alkali Metal Ions) Eg. Li Group 2 (Alkaline Earth Ions) Eg. BeDavid SobralNo ratings yet
- Superparamagnetism: Limits and ApplicationsDocument7 pagesSuperparamagnetism: Limits and ApplicationsNguyen VuNo ratings yet
- SVS.4096 A4.1017 - Elliott Repair Capabilities in Asia PacificDocument16 pagesSVS.4096 A4.1017 - Elliott Repair Capabilities in Asia PacificJOSE GARCIANo ratings yet
- MSDS Maptrons Organic Acidfree Toilet Bowl Cleaner PDFDocument4 pagesMSDS Maptrons Organic Acidfree Toilet Bowl Cleaner PDFanandNo ratings yet
- Wal-Mart Facility Security Assessment Application Form (English Only)Document3 pagesWal-Mart Facility Security Assessment Application Form (English Only)Ranjit RoyNo ratings yet
- Reactive Chemistry Incidents Can Happen Anywhere!: Did You Know?Document1 pageReactive Chemistry Incidents Can Happen Anywhere!: Did You Know?KiranNo ratings yet
- 2011 Global Generic Directory DemoDocument14 pages2011 Global Generic Directory DemoBassem SalemNo ratings yet
- GED Chemistry Note3 (Chemical Reactions)Document7 pagesGED Chemistry Note3 (Chemical Reactions)Shahadat Hussain Parvez100% (2)