
Polymyalgia Rheumatica: Fast Facts
Polymyalgia Rheumatica: Fast Facts
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Otc Advisor PainDocument24 pagesOtc Advisor Painfarzad100% (2)
- Onicomicosis y Laser 2020. 3 Long de Onda.Document15 pagesOnicomicosis y Laser 2020. 3 Long de Onda.Luis Angel Díaz MarínNo ratings yet
- Signs of Mental Retardation in ChildrenDocument6 pagesSigns of Mental Retardation in ChildrenShine 2009No ratings yet
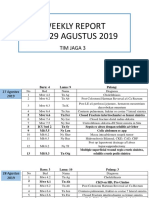
- WR Tim Jaga 3Document285 pagesWR Tim Jaga 3VincentiusNo ratings yet
- Amniotic Fluid and ItDocument8 pagesAmniotic Fluid and ItSaman SarKoNo ratings yet
- Cognitive-Behavioral Therapies For Personality DisordersDocument8 pagesCognitive-Behavioral Therapies For Personality DisordersTeodor CiobanuNo ratings yet
- Chlorpheniramine MaleateDocument3 pagesChlorpheniramine Maleateapi-3797941100% (1)
- 155 PenyakitDocument112 pages155 Penyakitpuskesmas kedungdoroNo ratings yet
- Thesis PoDocument5 pagesThesis PoJane SandovalNo ratings yet
- Duloxetine PDFDocument4 pagesDuloxetine PDFscribdseewalNo ratings yet
- DR Ashfaq ResumeDocument1 pageDR Ashfaq Resumedidoba7635No ratings yet
- What Is PresbycusisDocument4 pagesWhat Is PresbycusisNisa UcilNo ratings yet
- dm2020 0123Document47 pagesdm2020 0123Franchise AlienNo ratings yet
- Emedica MRCGP AKT Curriculum ChecklistDocument42 pagesEmedica MRCGP AKT Curriculum ChecklistSana Mustafa100% (1)
- Resume - Hamid Kermani MoakharDocument2 pagesResume - Hamid Kermani Moakharmohammadrezahajian12191No ratings yet
- HSD Sept22 Clin Chem Saqs Essay and Case Studies Exam PapersDocument10 pagesHSD Sept22 Clin Chem Saqs Essay and Case Studies Exam PapersYusuph MipawaNo ratings yet
- Ohmega: Ambulatory Impedance-pH RecorderDocument4 pagesOhmega: Ambulatory Impedance-pH RecorderMoas GabrounNo ratings yet
- Neoplasias Cisticas Do PancreasDocument37 pagesNeoplasias Cisticas Do PancreasMoises BitencourtNo ratings yet
- Dress Syndrome A Review and UpdateDocument5 pagesDress Syndrome A Review and UpdateCarlos Alberto Torres LópezNo ratings yet
- YCYSt DocumentDocument24 pagesYCYSt DocumentDodo AlsunaidiNo ratings yet
- Ulse Ximetry: Steven J. BarkerDocument17 pagesUlse Ximetry: Steven J. BarkerBRYAN RAFAEL ALEMAN HERNANDEZNo ratings yet
- Treating Vulvovaginal Atrophy Genitourinary Syndrome of Menopause How Important Is Vaginal Lubricant and Moisturizer CompositionDocument12 pagesTreating Vulvovaginal Atrophy Genitourinary Syndrome of Menopause How Important Is Vaginal Lubricant and Moisturizer CompositionPELVIC ANGELNo ratings yet
- Childrens Health Discipline GuideDocument41 pagesChildrens Health Discipline GuidegurkibajwaNo ratings yet
- BronchopneumoniaDocument11 pagesBronchopneumoniaDesiree GuerraNo ratings yet
- Immunopathology of Vesicular Cutaneous Lupus Erythematosus in The Rough Collie and Shetland Sheepdog - A Canine Homologue of SubacuteDocument10 pagesImmunopathology of Vesicular Cutaneous Lupus Erythematosus in The Rough Collie and Shetland Sheepdog - A Canine Homologue of SubacutejenNo ratings yet
- Product Monograph - Zoledronic Acid For Injection ConcentrateDocument58 pagesProduct Monograph - Zoledronic Acid For Injection ConcentrateMisgi Candra DasaNo ratings yet
- Incisions and ClosuresDocument14 pagesIncisions and ClosuresSalazar ÁngelNo ratings yet
- 342 FullDocument9 pages342 FulldrdevvratNo ratings yet
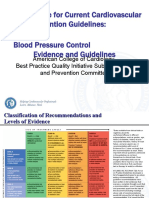
- 3 ACC Prevention Blood PressureDocument69 pages3 ACC Prevention Blood PressureMelissa Delgado100% (1)
- Jan 24 Skeletal Embryology and Limb Growth Stanmore Dr. Riego de Dios CPT TiongsonDocument3 pagesJan 24 Skeletal Embryology and Limb Growth Stanmore Dr. Riego de Dios CPT TiongsonMarlon MejiaNo ratings yet




































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Otc Advisor PainDocument24 pagesOtc Advisor Painfarzad100% (2)
- Onicomicosis y Laser 2020. 3 Long de Onda.Document15 pagesOnicomicosis y Laser 2020. 3 Long de Onda.Luis Angel Díaz MarínNo ratings yet
- Signs of Mental Retardation in ChildrenDocument6 pagesSigns of Mental Retardation in ChildrenShine 2009No ratings yet
- WR Tim Jaga 3Document285 pagesWR Tim Jaga 3VincentiusNo ratings yet
- Amniotic Fluid and ItDocument8 pagesAmniotic Fluid and ItSaman SarKoNo ratings yet
- Cognitive-Behavioral Therapies For Personality DisordersDocument8 pagesCognitive-Behavioral Therapies For Personality DisordersTeodor CiobanuNo ratings yet
- Chlorpheniramine MaleateDocument3 pagesChlorpheniramine Maleateapi-3797941100% (1)
- 155 PenyakitDocument112 pages155 Penyakitpuskesmas kedungdoroNo ratings yet
- Thesis PoDocument5 pagesThesis PoJane SandovalNo ratings yet
- Duloxetine PDFDocument4 pagesDuloxetine PDFscribdseewalNo ratings yet
- DR Ashfaq ResumeDocument1 pageDR Ashfaq Resumedidoba7635No ratings yet
- What Is PresbycusisDocument4 pagesWhat Is PresbycusisNisa UcilNo ratings yet
- dm2020 0123Document47 pagesdm2020 0123Franchise AlienNo ratings yet
- Emedica MRCGP AKT Curriculum ChecklistDocument42 pagesEmedica MRCGP AKT Curriculum ChecklistSana Mustafa100% (1)
- Resume - Hamid Kermani MoakharDocument2 pagesResume - Hamid Kermani Moakharmohammadrezahajian12191No ratings yet
- HSD Sept22 Clin Chem Saqs Essay and Case Studies Exam PapersDocument10 pagesHSD Sept22 Clin Chem Saqs Essay and Case Studies Exam PapersYusuph MipawaNo ratings yet
- Ohmega: Ambulatory Impedance-pH RecorderDocument4 pagesOhmega: Ambulatory Impedance-pH RecorderMoas GabrounNo ratings yet
- Neoplasias Cisticas Do PancreasDocument37 pagesNeoplasias Cisticas Do PancreasMoises BitencourtNo ratings yet
- Dress Syndrome A Review and UpdateDocument5 pagesDress Syndrome A Review and UpdateCarlos Alberto Torres LópezNo ratings yet
- YCYSt DocumentDocument24 pagesYCYSt DocumentDodo AlsunaidiNo ratings yet
- Ulse Ximetry: Steven J. BarkerDocument17 pagesUlse Ximetry: Steven J. BarkerBRYAN RAFAEL ALEMAN HERNANDEZNo ratings yet
- Treating Vulvovaginal Atrophy Genitourinary Syndrome of Menopause How Important Is Vaginal Lubricant and Moisturizer CompositionDocument12 pagesTreating Vulvovaginal Atrophy Genitourinary Syndrome of Menopause How Important Is Vaginal Lubricant and Moisturizer CompositionPELVIC ANGELNo ratings yet
- Childrens Health Discipline GuideDocument41 pagesChildrens Health Discipline GuidegurkibajwaNo ratings yet
- BronchopneumoniaDocument11 pagesBronchopneumoniaDesiree GuerraNo ratings yet
- Immunopathology of Vesicular Cutaneous Lupus Erythematosus in The Rough Collie and Shetland Sheepdog - A Canine Homologue of SubacuteDocument10 pagesImmunopathology of Vesicular Cutaneous Lupus Erythematosus in The Rough Collie and Shetland Sheepdog - A Canine Homologue of SubacutejenNo ratings yet
- Product Monograph - Zoledronic Acid For Injection ConcentrateDocument58 pagesProduct Monograph - Zoledronic Acid For Injection ConcentrateMisgi Candra DasaNo ratings yet
- Incisions and ClosuresDocument14 pagesIncisions and ClosuresSalazar ÁngelNo ratings yet
- 342 FullDocument9 pages342 FulldrdevvratNo ratings yet
- 3 ACC Prevention Blood PressureDocument69 pages3 ACC Prevention Blood PressureMelissa Delgado100% (1)
- Jan 24 Skeletal Embryology and Limb Growth Stanmore Dr. Riego de Dios CPT TiongsonDocument3 pagesJan 24 Skeletal Embryology and Limb Growth Stanmore Dr. Riego de Dios CPT TiongsonMarlon MejiaNo ratings yet