Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- American Society of Anesthesiologists Consensus-Based Guidance on Preoperative Management of Patients (Adults and Children) on Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists American Society of Anesthesiologists (ASA)Document7 pagesAmerican Society of Anesthesiologists Consensus-Based Guidance on Preoperative Management of Patients (Adults and Children) on Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists American Society of Anesthesiologists (ASA)felipetheNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Risk Assessment and Jop Safety Practice JSPDocument20 pagesRisk Assessment and Jop Safety Practice JSPShafie ZubierNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Care of ElderlyDocument130 pagesCare of Elderlyankita93% (14)
- Western Ontario and McMaster Universities Osteoarthritis IndexDocument6 pagesWestern Ontario and McMaster Universities Osteoarthritis IndexJesse FlingNo ratings yet
- EI2311-Biomedical Instrumentation Question BankDocument20 pagesEI2311-Biomedical Instrumentation Question BankrajapandiyaNo ratings yet
- Connective TissueDocument21 pagesConnective TissueCalvin Lin Jia RongNo ratings yet
- BCM CPX Orientation 2016Document30 pagesBCM CPX Orientation 2016Chan ChanNo ratings yet
- Hec Curriculum BSN-MSN 2024Document37 pagesHec Curriculum BSN-MSN 2024Zia Ul HassanNo ratings yet
- Speaking Part 3 Update 2022Document7 pagesSpeaking Part 3 Update 2022Nhi LêNo ratings yet
- Guidelinesfordomestictravel (Airortrainorinter Statebustravel) PDFDocument1 pageGuidelinesfordomestictravel (Airortrainorinter Statebustravel) PDFBhai Amerik JiNo ratings yet
- A Journal Report of Receipt of Mrna Covid-19 Vaccines and Risk of Spontaneous AbortionDocument11 pagesA Journal Report of Receipt of Mrna Covid-19 Vaccines and Risk of Spontaneous AbortionNica Joy DesquitadoNo ratings yet
- Final Hand Book of Covid 19 AFMCDocument174 pagesFinal Hand Book of Covid 19 AFMCPadmapriya SrinivasanNo ratings yet
- Cir 0000000000000757Document458 pagesCir 0000000000000757Nona Suci rahayuNo ratings yet
- JurnalDocument10 pagesJurnalekalapaleloNo ratings yet
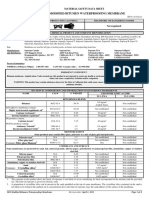
- MSDS BitumaxDocument4 pagesMSDS BitumaxNisaNo ratings yet
- Exp. 9 Test For Vitamin CDocument5 pagesExp. 9 Test For Vitamin CEdchelNo ratings yet
- Lutung Kasarung Story - Fiqri Aldiansyah - 32.0577 - F-4Document3 pagesLutung Kasarung Story - Fiqri Aldiansyah - 32.0577 - F-4Fiqri AldiansyahNo ratings yet
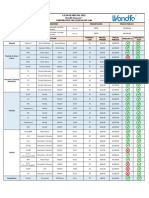
- Lista de Precios Publico Finecare Multiservicios Lab 2022Document2 pagesLista de Precios Publico Finecare Multiservicios Lab 2022Gerardo DiazNo ratings yet
- 10 1016@j Jiac 2017 02 014Document12 pages10 1016@j Jiac 2017 02 014Achmad YunusNo ratings yet
- Bipolar 1 DisorderDocument11 pagesBipolar 1 DisorderGirlly AlcantaraNo ratings yet
- Global Asbestos Disaster: Environmental Research and Public HealthDocument11 pagesGlobal Asbestos Disaster: Environmental Research and Public HealthThiago Campos MeiraNo ratings yet
- 4 Brunnstrom ApproachDocument18 pages4 Brunnstrom ApproachHabibieNaufal ChannelNo ratings yet
- Major Depressive Disorder in Adults 2016 (Philippines)Document29 pagesMajor Depressive Disorder in Adults 2016 (Philippines)Doroteo Jose StationNo ratings yet
- DS160 ApplicationDocument6 pagesDS160 ApplicationMujjuatharNo ratings yet
- Blood Pressure Levels For Boys by Age and Height Percentile: BP (Percentile) Systolic BP (MMHG) Diastolic BP (MMHG)Document4 pagesBlood Pressure Levels For Boys by Age and Height Percentile: BP (Percentile) Systolic BP (MMHG) Diastolic BP (MMHG)Annisa NurulNo ratings yet
- Pregnancy ArticleDocument2 pagesPregnancy ArticleRika AprilianiNo ratings yet
- NYSORA - The New York School of Regional Anesthesia - Spinal Anesthesia - ContinuedDocument16 pagesNYSORA - The New York School of Regional Anesthesia - Spinal Anesthesia - ContinuedPatrick RetengNo ratings yet
- The Basics of VirusesDocument4 pagesThe Basics of VirusesSharolt SierraNo ratings yet
- Soumya S Nair Biodata 4-07Document24 pagesSoumya S Nair Biodata 4-07ElizabethNo ratings yet
- GI Endo Eval Exam IIDocument7 pagesGI Endo Eval Exam IICraig Jesse B. LardizabalNo ratings yet