Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- APC CAOP Practice Paper Answer Sheet v1.2014 PDFDocument4 pagesAPC CAOP Practice Paper Answer Sheet v1.2014 PDFhappyscottlee3438100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Dosage Cal ProblemsDocument13 pagesDosage Cal ProblemsNatalie DukesNo ratings yet
- Cialis Marketing PlanDocument5 pagesCialis Marketing PlanAsaad BayanNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ertapenem (Invanz)Document1 pageErtapenem (Invanz)Adrianne BazoNo ratings yet
- Vicks AssignmentDocument4 pagesVicks AssignmentUshnaTahirNo ratings yet
- Section 5 The Nervous SystemDocument33 pagesSection 5 The Nervous SystemNasir Javed96% (24)
- Step Eugenic Programmed Murder of Myra Snyder ScottDocument23 pagesStep Eugenic Programmed Murder of Myra Snyder ScottRally The PeopleNo ratings yet
- Data ObatDocument21 pagesData ObatHalimatun SyadyahNo ratings yet
- MathDocument7 pagesMathGiorgi BradNo ratings yet
- Sampah Segi3Document648 pagesSampah Segi3River Chandra CiscNo ratings yet
- Combined Analgesics in (Headache) Pain Therapy: Shotgun Approach or Precise Multi-Target Therapeutics?Document15 pagesCombined Analgesics in (Headache) Pain Therapy: Shotgun Approach or Precise Multi-Target Therapeutics?NirmalaNo ratings yet
- June 2016 Recalls PDFDocument262 pagesJune 2016 Recalls PDFJunaid Ali KhanNo ratings yet
- Batuk - Pilek Harga Jumlah Barang: Satuan Masuk Terjual SisaDocument7 pagesBatuk - Pilek Harga Jumlah Barang: Satuan Masuk Terjual Sisadoni januarindraNo ratings yet
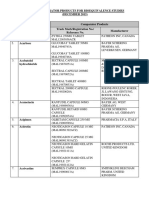
- Malaysia-NPRA List of Comparator Products For Bioequivalence Studies December 2015Document47 pagesMalaysia-NPRA List of Comparator Products For Bioequivalence Studies December 2015Noples RozaliaNo ratings yet
- Antidepressant DrugsDocument41 pagesAntidepressant DrugsSashaKay100% (5)
- p2018b3 SampleDocument21 pagesp2018b3 SampleAhmad FahroziNo ratings yet
- Public Assessment Report Decentralised ProcedureDocument22 pagesPublic Assessment Report Decentralised ProcedureHemang M. GajjarNo ratings yet
- JURIS Laws PDFDocument3 pagesJURIS Laws PDFuypaul97No ratings yet
- Pedoman Teknis Ipal 2011Document26 pagesPedoman Teknis Ipal 2011ChristellaNo ratings yet
- Drug StudyDocument7 pagesDrug StudyDiana Laura LeiNo ratings yet
- Lqts Drugs To AvoidDocument3 pagesLqts Drugs To AvoidHeart of the Valley, Pediatric CardiologyNo ratings yet
- Bromhexini Syrup LeafletDocument2 pagesBromhexini Syrup LeafletAlbert RenardNo ratings yet
- Mark Leeson 1 SubstanceAbuse UnjustifiedPrescriptions PDFDocument25 pagesMark Leeson 1 SubstanceAbuse UnjustifiedPrescriptions PDFWKYC.comNo ratings yet
- Hospital Pharmacy ProfileDocument7 pagesHospital Pharmacy ProfileJessica BautistaNo ratings yet
- Methamphetamines: Part OneDocument2 pagesMethamphetamines: Part OneFroggy100% (16)
- Antibiotic Desensitization ProtocolsDocument7 pagesAntibiotic Desensitization ProtocolsMichael FreudigerNo ratings yet
- AntiemeticsDocument4 pagesAntiemeticsAhmad Ariff Azmer MunshiNo ratings yet
- OfloxacinDocument3 pagesOfloxacinAnandUnniNo ratings yet
- CIWA-Ar F11Document2 pagesCIWA-Ar F11ssere6146No ratings yet
- Supervisi Apoteker (Icu)Document24 pagesSupervisi Apoteker (Icu)Erin FatmawatiNo ratings yet