Am J Cardiovasc Dis 2013;3(2):85-90
www.AJCD.us /ISSN:2160-200X/AJCD1304002
Original Article
Elevated S100A12 and sRAGE are associated with
increased length of hospitalization after non-urgent
coronary artery bypass grafting surgery
Ricardo Scheiber-Camoretti1, Amit Mehrotra1, Ling Yan1, Jai Raman2, John F Beshai1, Marion A Hofmann
Bowman1
1
Department of Medicine, Section of Cardiology, The University of Chicago, Chicago Illinois, USA; 2Department of
Surgery, Section of Cardiothoracic Surgery, The University of Chicago, Chicago Illinois, USA
Received April 4, 2013; Accepted May 15, 2013; Epub June 10, 2013; Published June 15, 2013
Abstract: Study’s purpose: Plasma levels of soluble receptor for advanced glycation endproducts (sRAGE) and
S100A12 are increased in young children after cardiac surgery and correlate with the time spent on cardiopul-
monary bypass (CPB). This study was performed to investigate whether plasma levels of sRAGE and S100A12 are
affected by the use of CPB. Levels of S100A12 and sRAGE, along with of interleukin-6, tumor necrosis factor-α,
myeloperoxidase, and C-reactive protein were measured in 25 adults undergoing non-urgent coronary artery bypass
grafting with and without the use of CPB. Significant finding: Plasma levels of S100A12, sRAGE, IL-6, TNF-α and MPO
4h after cardiac surgery were elevated compared to baseline; this increase was equally observed in patients under-
going traditional coronary artery bypass grafting on cardiopulmonary bypass (n = 16), and in patients undergoing
robot-assisted coronary artery bypass grafting off pump (OPCAB, n = 9). Patients with prolonged hospitalization of 7
days or longer had significantly higher S100A12 and sRAGE 4 hours post surgery compared to patients hospitalized
≤ 6 days. Conclusion: Increased sRAGE and S100A12 after cardiac surgery is associated with prolonged length of
hospitalization in patients after coronary artery bypass grafting; however, we did not observe an intrinsic effect of
cardiopulmonary bypass on S100A12 or sRAGE plasma levels in our small pilot study. Further studies are required
to confirm the value of sRAGE and S100A12 in predicting postoperative complications after cardiac surgery in a
larger study.
Keywords: Coronary artery bypass graft surgery, S100/calgranulin, sRAGE, biomarker
Introduction S100A12 is a member of the S100 family of cal-
cium binding proteins and highly expressed
The systemic inflammatory response in patients endogenously in neutrophilic granulocytes and
undergoing cardiac surgery contributes sub- lesser in other cells. Accordingly, elevated
stantially to postoperative organ dysfunction, serum concentration of S100A12 is an emerg-
morbidity and mortality. The degree of cytokine ing biomarker of various chronic and acute
release during and after cardiac surgery varies inflammatory diseases, including acute lung
considerable among different studies and this injury [5-7]. Due to the ability to activate RAGE,
is likely influenced by many factors and pro- a multi-ligand cell surface receptor abundantly
cesses such as tissue damage, reperfusion expressed in alveolar lung cells and other cells,
injury, peri-operatively administered drugs and there is growing evidence that S100A12 may
hemodilution, as well as inter-individual cyto- modulates inflammation [8, 9]. Liu et al. recent-
kine responses to injury [1-3]. Particularly, ly reported on elevated plasma levels of
exposure of blood to non-endothelial surfaces S100A12 and sRAGE immediately after CPB in
in cardiopulmonary bypass (CPB) is debated as 58 children age < 3 years undergoing non-
a major contributor to the systemic inflamma- urgent surgery for congenital heart disease
tory response in patients undergoing coronary [10]. In this study, there was a positive correla-
artery bypass grafting (reviewed in [4]). tion of S100A12 and sRAGE plasma levels with
S100A12 and CABG
Table 1. Preoperative characteristics of patients undergoing coronary artery bypass grafting with car-
diopulmonary bypass (CABG with CPB) or off pump coronary artery bypass (OPCAB)
All patients (n = 25) CABG with CPB (n = 16) OPCAB (n = 9) P-value
Mean (SD) age (years) 60.9 (8.3) 58 (7.8) 60 (8.1) 0.27
Male 17 (68) 12 (75) 5 (55) 0.36
Current smoker 10 (40) 6 (37) 4 (44) 0.2
LV EF > 50% 14 (56) 8 (50) 6 (67) 0.3
LV EF 30%-49% 11 (44) 8 (50) 3 (33) 0.6
Diabetes 9 (36) 6 (37) 3 (33) 0.6
Hypertension 20 (80) 14 (87) 6 (66) 0.4
Statin use 19 (76) 11 (68) 8 (88) 0.2
COPD 3 (12) 1 (6) 2 (22) 0.04
Euro-Score 8.7 8.4 8.8 0.34
Mean (SD) Operation time (min) 302 (56) 312 (45) 290 (78) 0.43
In-hospital mortality 0 0 0
Mean (SD) Hospital LOS (days) 7.2 (5.3) 7.4 (6.7) 6.2 (4.1) 0.35
Values are numbers (percentages) unless stated otherwise. (LOS, length of stay).
incidence of acute lung injury and with pro- enced cardiac surgeons operated on all 25
longed length of hospitalization. Additionally, patients with no overlap between OPCAP and
Liu et al. reported a strong positive correlation CABG with CPD. All patients underwent routine
between the time spent on CPB and the preoperative and postoperative care directed
increase in these biomarkers post-surgery, rais- by the multidisciplinary surgical and medical
ing the hypothesis that altered hemodynamics team. The operative risk before surgery was
or contact with non-endothelial surfaces adher- prospectively calculated using the additive and
ent to CPB could possibly affect plasma con- logistic European System for Cardiac Operative
centration of S100A12 and sRAGE. In the here Risk Evaluation (Euro-SCORE [11]. An echo
presented study we examine the impact of CPB board certified reader measured the left ven-
on plasma concentrations of S100A12 and tricular ejection fraction (LV-EF) on transtho-
sRAGE in a small non-randomized single center racic echocardiograms prior surgery. All other
observational study of consecutive patients demographic data were collected retrospec-
undergoing elective coronary artery bypass tively from the electronic medical records.
grafting. Diabetes was defined by the use of oral medi-
cation or insulin prior surgery or upon dis-
Materials and methods charge, hypertension was defined as systolic
blood pressure > 140 before surgery or the use
Blood samples were prospectively collected on of antihypertensive medication, COPD was
25 consecutive adult patients undergoing non- defined by documented moderately or severely
urgent coronary artery bypass grafting surgery abnormal pulmonary function tests or the use
at The University of Chicago Medical Center. We of inhaler. Hospital length of stay (LOS) was
excluded patients with myocardial infarction defined as days spent in the hospital after coro-
within 6 weeks prior surgery, severe left ven- nary artery bypass grafting surgery. Discharge
tricular dysfunction (ejection fraction < 30%), from the hospital occurred daily and was deter-
chronic kidney disease > stage III, emergency mined by the surgical and medical team.
surgery after angiography or percutaneous cor-
onary intervention. Of those 25 patients, 9 sub- Blood samples were collected immediately
jects had off pump coronary artery bypass prior (0 h, in the operating room) and 4 h after
(OPCAP) using the da Vinci robot, and 16 completed cardiac surgery using a vacuum
patients had conventional coronary artery tube containing EDTA. After centrifugation at
bypass grafting (CABG with CPB). Patients were 3000 rpm for 15 min at 4°C, plasma aliquots
not randomized and the surgeon in consulta- were stored at -80°C until use. S100A12,
tion with the patient made the decision for sRAGE, IL-6, TNF-α, MPO, and CRP were select-
OPCAP versus CABG with CPD. Three experi- ed as candidate biomarker and measured
86 Am J Cardiovasc Dis 2013;3(2):85-90
S100A12 and CABG
Table 2. Plasma biomarker concentration in patients undergoing coronary artery bypass grafting with
cardiopulmonary bypass (CABG with CPB) or off pump coronary artery bypass (OPCAB)
All patients (n = 25) CABG with CPB (n = 16) OPCAB (n = 9) P-value
sRAGE, 0 h, pg/ml 765 (246) 659 (221) 771 (233) 0.273
sRAGE, 4 h, pg/ml 1976 (671)* 2145 (632)* 1732 (634)* 0.432
S100A12, 0 h, ng/ml 85 (65) 88 (49) 68 (62) 0.385
S100A12, 4 h, ng/ml 3458 (420)* 2956 (379)* 3638 (420)* 0.276
Il-6, 0 h, pg/ml 14 (21) 13 (19) 14 (22) 0.456
IL-6, 4 h, pg/ml 431 (210)* 386 (194)* 482 (170)* 0.441
MPO, 0 h, ng/ml 9.4 (4.8) 8.3 (3.8) 9.6 (4.6) 0.391
MPO, 4 h, ng/ml 23.5 (11.8)* 24.6 (9.2)* 22.6 (8.7)* 0.456
TNF-α, 0 h, pg/ml 5.2 (4.1) 5.1 (3.7) 4.7 (3.6) 0.415
TNF-α, 4 h, pg/ml 9.6 (4.1)* 9.5 (4.1)* 9.7 (3.9)* 0.562
CRP, 0 h, µg/ml 0.9 (1.3) 0.9 (1.1) 0.8 (1.2) 0.432
CRP, 4 h, µg/ml 1.4 (3.1) 1.8 (2.2) 1.3 (2.6) 0.643
Values are mean ± (SD). *p < 0.05 compared to time respective point 0 h. (sRAGE, soluble receptor for advanced glycation end
products; IL-6, interleukin-6; MPO, myeloperoxidase; TNF-α, tumor necrosis factor alpha; CRP, C-reactive protein).
using commercially available ELISA kits (R&D diately prior to cardiac surgery (Table 2).
systems), or as previously published for Furthermore, IL-6 (431 pg/ml ± 210 vs. 14 pg/
S100A12 [12]. Human plasma was obtained ml ± 21; p = 0.00038), MPO (23.5 ng/ml ± 11
with informed consent and approved by the vs. 9.4 ng/ml ± 4.8, p < 0.00001), and TNF-α
University of Chicago Institutional Review (9.6 pg/ml ± 4.1 vs. 5.2 pg/ml ± 4.1; p = 0.04)
Board. were also significantly increased postoperative-
ly, but not CRP (0.9 µg/ml ± 1.3 vs. 1.4 µg/ml,
Descriptive statistics (percentage, mean, and ± 3.1; p = 0.226).
standard deviation), crude comparison based
on chi-square statistics and plots were used to When patients were divided according to their
describe the patient cohort. All continuous data use (n = 16) or not use (n = 9) of CBP we found
are reported as mean ± SD. The independent- no difference in all measured cytokines and
sample t-test and one-way analysis of variance biomarker (IL-6, TNF-α, sRAGE, S100A12, MPO,
were used for mean comparison between the 2 CRP) at baseline 0 h and at 4 h after surgery
groups. We considered differences significant between patients in the OPCAB group com-
when p values were less than or equal to 0.05. pared to patients undergoing CABG with CPB
(Table 2). This suggests that the use of cardio-
Results pulmonary bypass does not by itself contrib-
utes independently to the up-regulation of
Baseline characteristics were similar between S100A12 and sRAGE as previously suggested
patients assigned to conventional coronary by the positive association of CPB time with
artery bypass grafting surgery and those postoperatively S100A12 and sRAGE [10].
assigned to off pump coronary artery bypass
grafting surgery (Table 1), except a higher fre- The mean hospital length of stay until discharge
quency of COPD in the OPCAB group with 2/9 was 7.2 days and there was no difference
patients having COPD compared to 1/16 in the between the groups treated by CABG with CPB
conventional group (Table 1). No cross over and treated by OPCAB (Table 1). Interestingly,
occurred between the two groups. when we stratified all 25 patients undergoing
coronary artery bypass grafting according to
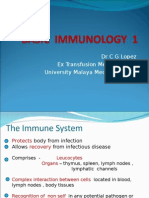
Similar to the findings of Liu et al. [10], we found their hospital length of stay (LOS), we found
a strong increase in plasma sRAGE (1976 pg/ that patients hospitalized 7 days or more (n =
ml ± 671 vs. 765 pg/ml ± 246; p = 0.00018) 13 including 5 patients with OPCAB) had higher
and S100A12 (3458 ng/ml ± 420 vs. 85 ng/ml 4h postoperative levels for S100A12 and
± 65; p = 0.00062) taken 4 h after completed sRAGE compared to patients with LOS ≤ 6 days
cardiac surgery compared to those taken imme- (n = 12 including 4 patients with OPCAB; Figure
87 Am J Cardiovasc Dis 2013;3(2):85-90
S100A12 and CABG
with length of hospitalization.
This confirms Liu et al.’s report
that showed a strong correla-
tion of postoperatively
increased S100A12 (p <
0.001) and sRAGE levels (p =
0.012) with impaired lung
function, acute lung injury and
hospital LOS in young children
undergoing cardiac surgery
for congenital heart disease
[10]. Importantly, while Liu’s
study found a correlation of
those biomarker with the time
Figure 1. Level of plasma S100A12 and sRAGE measured 4 h after coro- spent on CPB suggesting that
nary artery bypass surgeries are significantly elevated in patients with contact with non-endothelial
prolonged hospital length of stay (LOS). surfaces present in CPB could
possibly augment the release
1). However, no significant difference was of S100A12 from neutrophils, we did not
observed in 4 h postoperative levels of IL-6, observe any difference in S100A12 or sRAGE
TNF-α, MPO, and CRP between both groups. with regards to the use of CPB in patients
Notably, at baseline, patients with LOS ≥ 7 days undergoing coronary artery grafting bypass sur-
had higher levels of TNF-α (6.3 pg/ml ± 3.3 vs gery. Plasma abundance of S100A12 might
3.4 pg/ml ± 4.2, p = 0.002) but other marker stem from activated neutrophils, since
including sRAGE, S100A12, IL-6, MPO, or CRP S100A12 composes up to 5% of neutrophil
did not differ among patients with LOS ≥ 7 and cytosolic protein and is secreted upon activa-
LOS ≤ 6. Moreover, there was no significant dif- tion of protein kinase C or released during neu-
ference in all clinical parameter including age, trophil damage. In addition of serving as a bio-
gender, smoking status, LV-function, diabetes marker, an association of plasma S100A12
hypertension, statin use and COPD between with the length of hospitalization after CABG
patients with LOS ≥ 7 days or LOS ≤ 6 days. surgery might potentially indicate a direct role
Importantly, the additive Euro-Score, an index of S100A12 in modulating inflammatory path-
of co-morbidities that correlates with mortality ways associated with postoperative complica-
after cardiothoracic surgery [11], was similar tions. This is supported by our recent findings
for patients with LOS ≥ 7 (7.9, range 5-13) and examining S100A12 expression in aortic
LOS ≤ 6 days (8.3, range 6-12). Our finding of a smooth muscle. We found that pathological
positive association of postoperatively elevat- expression of S100A12 in the medial layer of
ed S100A12 and sRAGE plasma concentration aneurysmal aortic tissue predicted the length
with length of hospitalization in adults undergo- of hospitalization in patients undergoing surgi-
ing non-urgent coronary artery bypass grafting cal repair of thoracic aortic aneurysms [14].
extents earlier studies demonstrating a posi- Furthermore, we reported on a co-localization
tive correlation of S100A12 and/or sRAGE with of S100A12 with caspase-3 in the aortic media,
the onset of acute lung injury and adult respira- and found that reduction of S100A12 in cul-
tory distress syndrome [7, 10, 13]. Our study tured human aortic smooth muscle cells har-
suggests that both markers could be consid- vested from aneurysms attenuated cell inflam-
ered as useful early biomarker to indicate post- mation and apoptosis. This supports the
operative complications after cardiac surgery. hypothesis that S100A12 is not only is a bio-
marker of inflammation, but also may direct
Discussion participate in modulating inflammation.
In this prospective pilot study measuring plas- Our study has limitations that includes the
ma sRAGE and S100A12 in adult patients small size of only 25 patients being studied,
undergoing coronary artery bypass grafting we and non-randomization to the different treat-
observed an association of 4 h postoperatively ment strategies. There is considerable discus-
elevated S100A12 and sRAGE plasma levels sion as to whether the use of CPB impacts sys-
88 Am J Cardiovasc Dis 2013;3(2):85-90
S100A12 and CABG
temic inflammation in patients undergoing Address correspondence to: Dr. Marion A Hofmann
coronary artery bypass grafting, with many, Bowman, 5841 S. Maryland, MC6080 Chicago, IL
although mostly small studies like ours favor a 6063. Tel: 773 834 0807; Fax: 773 702 2681;
reduction in systemic inflammation by avoiding E-mail: mhofmann@medicine.bsd.uchicago.edu
CBP. This is reviewed by Raja et al [4]. Although
in our single center study we found a similar References
length of hospitalization between OPCAB and [1] Downing SW and Edmunds LH Jr. Release of
CABG with CPB, others have shown a signifi- vasoactive substances during cardiopulmo-
cant shorter duration in the length of hospital- nary bypass. Ann Thorac Surg 1992; 54: 1236-
ization in a prospectively randomized trial com- 1243.
paring both surgical techniques [15]. Two [2] Laffey JG, Boylan JF and Cheng DC. The sys-
randomized large clinical trials examining the temic inflammatory response to cardiac sur-
benefits of CABG without cardiopulmonary gery: implications for the anesthesiologist. An-
bypass were recently reported. The study by esthesiology 2002; 97: 215-252.
Diegeler et al. found no difference in composite [3] Roth-Isigkeit A, Hasselbach L, Ocklitz E, Bruck-
outcome of death, stroke, myocardial infarc- ner S, Ros A, Gehring H, Schmucker P, Rink L
and Seyfarth M. Inter-individual differences in
tion, repeat revascularization, or new renal-re-
cytokine release in patients undergoing cardi-
placement therapy within 30 days and within ac surgery with cardiopulmonary bypass. Clin
12 month after surgery in 2539 patients 75 Exp Immunol 2001; 125: 80-88.
years and older randomized to either off-pump [4] Raja SG and Berg GA. Impact of off-pump coro-
CABG or on-pump CABG [16]. A second large nary artery bypass surgery on systemic inflam-
multicenter randomized clinical trial examined mation: current best available evidence. J Card
the quality of life, neurocognitive function and Surg 2007; 22: 445-455.
clinical outcome 1 year after randomization of [5] Hofmann Bowman MA and Schmidt AM. S100/
4752 patients undergoing CABG on pump or off calgranulins EN-RAGEing the blood vessels:
pump, and found no significant difference in implications for inflammatory responses and
the rate of the primary or composite outcome atherosclerosis. Am J Cardiovasc Dis 2011; 1:
92-100.
[17].
[6] Meijer B, Gearry RB and Day AS. The role of
Taken together, our study confirms and extends S100A12 as a systemic marker of inflamma-
tion. Int J Inflam 2012; 2012: 907078.
the findings of Liu et al. and suggests that the
[7] Wittkowski H, Sturrock A, van Zoelen MA, Vie-
trauma related to cardiothoracic surgery itself,
mann D, van der Poll T, Hoidal JR, Roth J and
rather than intrinsic factors specific to CPB may Foell D. Neutrophil-derived S100A12 in acute
mediate the marked increase in serum lung injury and respiratory distress syndrome.
S100A12 and sRAGE measured 4 hours after Crit Care Med 2007; 35: 1369-1375.
cardiac surgery; however larger studies are [8] Hofmann MA, Drury S, Fu C, Qu W, Taguchi A,
needed for confirmation. Moreover, although Lu Y, Avila C, Kambham N, Bierhaus A, Nawroth
suggested by our pilot study, larger studies are P, Neurath MF, Slattery T, Beach D, McClary J,
needed to examine whether S100A12 and Nagashima M, Morser J, Stern D and Schmidt
sRAGE could serve as useful biomarker to pre- AM. RAGE mediates a novel proinflammatory
dict postoperative complications in patients axis: a central cell surface receptor for S100/
undergoing cardiac surgery. calgranulin polypeptides. Cell 1999; 97: 889-
901.
Acknowledgments [9] Schmidt AM, Yan SD, Yan SF and Stern DM.
The multiligand receptor RAGE as a progres-
This study was supported by funding from the sion factor amplifying immune and inflamma-
tory responses. J Clin Invest 2001; 108: 949-
Doris Duke Charitable Foundation. Dr. Hofmann
955.
Bowman is a recipient of the Doris Duke Clinical [10] Liu X, Chen Q, Shi S, Shi Z, Lin R, Tan L, Yu J,
Scientist Development Award. Shu Q and Fang X. Plasma sRAGE enables pre-
diction of acute lung injury following cardiac
Declaration of interest surgery in children. Crit Care 2012; 16: R91.
[11] Kurki TS, Jarvinen O, Kataja MJ, Laurikka J and
All authors have reported that they have no Tarkka M. Performance of three preoperative
relationship relevant to the contents of this risk indices; CABDEAL, EuroSCORE and Cleve-
paper to disclose. land models in a prospective coronary bypass
89 Am J Cardiovasc Dis 2013;3(2):85-90
S100A12 and CABG
database. Eur J Cardiothorac Surg 2002; 21: pump coronary artery bypass surgery on clini-
406-410. cal, angiographic, neurocognitive, and quality
[12] Hofmann Bowman MA, Heydemann A, Gawdzik of life outcomes: randomised controlled trial.
J, Shilling RA and Camoretti-Mercado B. Trans- BMJ 2006; 332: 1365.
genic expression of human S100A12 induces [16] Diegeler A, Börgermann J, Kappert U, Breuer
structural airway abnormalities and limited M, Böning A, Ursulescu A, Rastan A, Holzhey D,
lung inflammation in a mouse model of allergic Treede H, Rieß FC, Veeckmann P, Asfoor A, Re-
inflammation. Clin Exp Allergy 2011; 41: 878- ents W, Zacher M and Hilker M; GOPCABE
889. Study Group. Off-Pump versus On-Pump Coro-
[13] Jabaudon M, Futier E, Roszyk L, Chalus E, nary-Artery Bypass Grafting in Elderly Patients.
Guerin R, Petit A, Mrozek S, Perbet S, Cayot- N Engl J Med 2013; 368: 1189-1198.
Constantin S, Chartier C, Sapin V, Bazin JE and [17] Lamy A, Devereaux PJ, Prabhakaran D, Taggart
Constantin JM. Soluble form of the receptor for DP, Hu S, Paolasso E, Straka Z, Piegas LS, Akar
advanced glycation end products is a marker AR, Jain AR, Noiseux N, Padmanabhan C, Ba-
of acute lung injury but not of severe sepsis in hamondes JC, Novick RJ, Vaijyanath P, Reddy
critically ill patients. Crit Care Med 2011; 39: SK, Tao L, Olavegogeascoechea PA, Airan B,
480-488. Sulling TA, Whitlock RP, Ou Y, Pogue J, Chro-
[14] Das D, Gawdzik J, Dellefave-Castillo L, McNally lavicius S, Yusuf S; CORONARY Investigators.
EM, Husain A, Raman J and Hofmann Bowman Effects of Off-Pump and On-Pump Coronary-
MA. S100A12 expression in thoracic aortic an- Artery Bypass Grafting at 1 Year. N Engl J Med
eurysm is associated with increased risk of 2013; 368: 1179-1188.
dissection and perioperative complications. J
Am Coll Cardiol 2012; 60: 775-785.
[15] Al-Ruzzeh S, George S, Bustami M, Wray J, Ils-
ley C, Athanasiou T and Amrani M. Effect of off-
90 Am J Cardiovasc Dis 2013;3(2):85-90
You might also like
- C105a Pre-Sea and Periodic Medical Fitness Examinations For SeafarersDocument4 pagesC105a Pre-Sea and Periodic Medical Fitness Examinations For SeafarersAbu ShabeelNo ratings yet
- Carotid Endarterectomy: Experience in 8743 Cases.Document13 pagesCarotid Endarterectomy: Experience in 8743 Cases.Alexandre Campos Moraes AmatoNo ratings yet
- (INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Document10 pages(INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Yolanda FitrianiNo ratings yet
- Ill Wind in FriezfordDocument36 pagesIll Wind in FriezfordNick KNo ratings yet
- Interceptive OrthodonticsDocument27 pagesInterceptive OrthodonticsDivya Shrivastava100% (1)
- Age +estimated+glomerular+filtration+rate+and+ejection+fraction+score+predicts+contrast-Induced+acute+kidney+injury+in+patients+with+diabetes+and+chronic+kidney+disease +insight+from+the+TRACK-D+studyDocument5 pagesAge +estimated+glomerular+filtration+rate+and+ejection+fraction+score+predicts+contrast-Induced+acute+kidney+injury+in+patients+with+diabetes+and+chronic+kidney+disease +insight+from+the+TRACK-D+studyangga_darmawan26No ratings yet
- The Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsDocument5 pagesThe Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsM Ali AdrianNo ratings yet
- 182 FullDocument3 pages182 FullViona ApriliaNo ratings yet
- Saito 2015Document5 pagesSaito 2015didingNo ratings yet
- Pjms 31 159Document5 pagesPjms 31 159christ_cruzerNo ratings yet
- Relationship Between Platelet-To-Lymphocyte Ratio and The Presence and Severity of Coronary Artery EctasiaDocument6 pagesRelationship Between Platelet-To-Lymphocyte Ratio and The Presence and Severity of Coronary Artery EctasiaAlamgirNo ratings yet
- 0068KJR - KJR 20 1546Document8 pages0068KJR - KJR 20 1546Joshua AmenNo ratings yet
- Preoperative Serum Bicarbonate Levels Predict Acute Kidney Injury After Cardiac SurgeryDocument11 pagesPreoperative Serum Bicarbonate Levels Predict Acute Kidney Injury After Cardiac SurgeryRoni ArmandaNo ratings yet
- International Journal of CardiologyDocument7 pagesInternational Journal of CardiologySergio DiazNo ratings yet
- Lee Et Al. 2017 Am J Cardiol OA vs. RADocument4 pagesLee Et Al. 2017 Am J Cardiol OA vs. RAPraveenVeeraNo ratings yet
- Outcome With High Blood Lactate Levels During Cardiopulmonary Bypass in Adult Cardiac OperationDocument5 pagesOutcome With High Blood Lactate Levels During Cardiopulmonary Bypass in Adult Cardiac OperationMuhammad RizqiNo ratings yet
- Kosuge 2011Document6 pagesKosuge 2011LAXMI DEVINo ratings yet
- Association of Platelet-to-Lymphocyte Ratio With Severity and Complexity of Coronary Artery Disease in Patients With Acute Coronary SyndromesDocument7 pagesAssociation of Platelet-to-Lymphocyte Ratio With Severity and Complexity of Coronary Artery Disease in Patients With Acute Coronary SyndromesMaferNo ratings yet
- Radial Artery Harvesting in Coronary Artery Bypass Grafting Surgery-Endoscopic or Open Method? A Meta-AnalysisDocument20 pagesRadial Artery Harvesting in Coronary Artery Bypass Grafting Surgery-Endoscopic or Open Method? A Meta-Analysisosve91No ratings yet
- Eficacia Del Clopidogrel en Pacientes Con Fibrilacion Auricular y Sindrome Coronario AgudoDocument7 pagesEficacia Del Clopidogrel en Pacientes Con Fibrilacion Auricular y Sindrome Coronario AgudoElva MonserrathNo ratings yet
- Liver Transplantation - 2012 - Plotkin - Coronary Artery Disease and Liver Transplantation The State of The Art PDFDocument4 pagesLiver Transplantation - 2012 - Plotkin - Coronary Artery Disease and Liver Transplantation The State of The Art PDFphonex xoxNo ratings yet
- Catheter Cardiovasc Interv 2021 May 27 Romeo FJDocument8 pagesCatheter Cardiovasc Interv 2021 May 27 Romeo FJFernando SousaNo ratings yet
- Keywords:-STS Score, MACE, CABGDocument6 pagesKeywords:-STS Score, MACE, CABGInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cytokine Clearance With Cytosorb® During Cardiac Surgery: A Pilot Randomized Controlled TrialDocument12 pagesCytokine Clearance With Cytosorb® During Cardiac Surgery: A Pilot Randomized Controlled Trialgra ndynNo ratings yet
- Koch 2016Document2 pagesKoch 2016Jocilene Dantas Torres NascimentoNo ratings yet
- Stroke and Encephalopathy After Cardiac SurgeryDocument11 pagesStroke and Encephalopathy After Cardiac Surgeryilmiah neurologiNo ratings yet
- JurnalDocument4 pagesJurnalAinul NurrahmahNo ratings yet
- Usefulness of Hyponatremia in The Acute Phase of ST-Elevation Myocardial Infarction As A Marker of SeverityDocument6 pagesUsefulness of Hyponatremia in The Acute Phase of ST-Elevation Myocardial Infarction As A Marker of SeverityJicko Street HooligansNo ratings yet
- PIIS1071916411003940Document1 pagePIIS1071916411003940Monica AlbertNo ratings yet
- Evaluation of Factors Affecting Liver Function Test in Patients Underwent Coronary Artery Bypass Graft SurgeryDocument7 pagesEvaluation of Factors Affecting Liver Function Test in Patients Underwent Coronary Artery Bypass Graft SurgeryajmrdNo ratings yet
- Main 51 ???Document5 pagesMain 51 ???pokharelriwaj82No ratings yet
- Journal of Cardiothoracic and Vascular Anesthesia: Letter To The EditorDocument2 pagesJournal of Cardiothoracic and Vascular Anesthesia: Letter To The Editorghg sddNo ratings yet
- Use of CT To Guide ManagementDocument10 pagesUse of CT To Guide ManagementnatayaregizaNo ratings yet
- Correlation Between Impaired Aortic Distensibility and The Severity of Coronary Artery Disease and Calcium Scoring Measured by Cardiac CTDocument20 pagesCorrelation Between Impaired Aortic Distensibility and The Severity of Coronary Artery Disease and Calcium Scoring Measured by Cardiac CTMunir AlshameeryNo ratings yet
- Predictive Variables For Mortality After Acute Ischemic StrokeDocument9 pagesPredictive Variables For Mortality After Acute Ischemic StrokeOscar PérezNo ratings yet
- Angina PostprandialDocument10 pagesAngina PostprandialJoaquín SosaNo ratings yet
- 0178959e6a78&ie SdarticleDocument7 pages0178959e6a78&ie SdarticleRiza Adi SaputraNo ratings yet
- Circulation 2014 Silvain 918 22Document6 pagesCirculation 2014 Silvain 918 22aninNo ratings yet
- Abstrak IsicamDocument22 pagesAbstrak IsicambgusjklNo ratings yet
- None 4Document8 pagesNone 4Yehiel FlaviusNo ratings yet
- CRRT After SurgeryDocument7 pagesCRRT After SurgeryZainab MotiwalaNo ratings yet
- Marcadores Sepsis Edit Intensive Care Medicine 2013 39 (10) 1824Document5 pagesMarcadores Sepsis Edit Intensive Care Medicine 2013 39 (10) 1824giseladelarosa2006No ratings yet
- Principle and Practice of CT in Cardiac AssessmentDocument47 pagesPrinciple and Practice of CT in Cardiac AssessmentSofia KusumadewiNo ratings yet
- Sica Ar 1Document8 pagesSica Ar 1Daniela Ceballos BarbourNo ratings yet
- Research ArticleDocument10 pagesResearch ArticleHashan AbeyrathneNo ratings yet
- Jurnal EBMDocument6 pagesJurnal EBMtaniaNo ratings yet
- AbstractDocument12 pagesAbstractMunir AlshameeryNo ratings yet
- The Total Cholesterol To High-Density Lipoprotein Cholesterol As A Predictor of Poor Outcomes in A Chinese Population With Acute Ischaemic StrokeDocument6 pagesThe Total Cholesterol To High-Density Lipoprotein Cholesterol As A Predictor of Poor Outcomes in A Chinese Population With Acute Ischaemic StrokeRay HannaNo ratings yet
- DCO After TAVRDocument12 pagesDCO After TAVRBogdan BotezanNo ratings yet
- Outcome Predictors in Acute Surgical Admissions For Lower Gastrointestinal BleedingDocument1 pageOutcome Predictors in Acute Surgical Admissions For Lower Gastrointestinal BleedingEd FitzgeraldNo ratings yet
- 2D Shear Wave Liver Elastography by Aixplorer To Detect PortalDocument12 pages2D Shear Wave Liver Elastography by Aixplorer To Detect PortalValentina IorgaNo ratings yet
- JCM 09 00619 v2Document14 pagesJCM 09 00619 v2Medicina FamiliarNo ratings yet
- Value of The Measurement of Portal Flow Velocity in The Differential Diagnosis of Asymptomatic SplenomegalyDocument4 pagesValue of The Measurement of Portal Flow Velocity in The Differential Diagnosis of Asymptomatic SplenomegalydenisegmeloNo ratings yet
- Transcatheter Based Aortic Valve Replacement vs. Isolated Surgical Aortic Valve ReplacemDocument10 pagesTranscatheter Based Aortic Valve Replacement vs. Isolated Surgical Aortic Valve ReplacemGaal PinNo ratings yet
- Piis1078588400911705 PDFDocument4 pagesPiis1078588400911705 PDFnilsNo ratings yet
- Ischemic 19Document8 pagesIschemic 19Adina Alexandra CNo ratings yet
- Factores para FNRDocument10 pagesFactores para FNRPOMYNo ratings yet
- Diab 5Document4 pagesDiab 5marsim92No ratings yet
- Application of Strain and Other Echocardiographic Parameters in The Evaluation of Early and Long-Term Clinical Outcomes After Cardiac Surgery RevascularizationDocument8 pagesApplication of Strain and Other Echocardiographic Parameters in The Evaluation of Early and Long-Term Clinical Outcomes After Cardiac Surgery RevascularizationSondang JasmineNo ratings yet
- Ischemia-Modified Albumin Use As A Prognostic Factor in Coronary Bypass SurgeryDocument5 pagesIschemia-Modified Albumin Use As A Prognostic Factor in Coronary Bypass SurgerySarah KemalasariNo ratings yet
- Blah 5 AsdsadsaDocument5 pagesBlah 5 Asdsadsaprern27No ratings yet
- Effects of Endotoxin On Pacemaker Funny Current in Hek 293 CellsDocument190 pagesEffects of Endotoxin On Pacemaker Funny Current in Hek 293 CellsNemo SecretNo ratings yet
- JHLT Abstract 2020-1Document1 pageJHLT Abstract 2020-1G WNo ratings yet
- Atlas of Coronary Intravascular Optical Coherence TomographyFrom EverandAtlas of Coronary Intravascular Optical Coherence TomographyNo ratings yet
- tmpF178 TMPDocument15 pagestmpF178 TMPFrontiersNo ratings yet
- Tmp1a96 TMPDocument80 pagesTmp1a96 TMPFrontiersNo ratings yet
- Tmpa077 TMPDocument15 pagesTmpa077 TMPFrontiersNo ratings yet
- tmpE3C0 TMPDocument17 pagestmpE3C0 TMPFrontiersNo ratings yet
- tmp998 TMPDocument9 pagestmp998 TMPFrontiersNo ratings yet
- tmp27C1 TMPDocument5 pagestmp27C1 TMPFrontiersNo ratings yet
- tmp96F2 TMPDocument4 pagestmp96F2 TMPFrontiersNo ratings yet
- tmp3656 TMPDocument14 pagestmp3656 TMPFrontiersNo ratings yet
- tmpA7D0 TMPDocument9 pagestmpA7D0 TMPFrontiersNo ratings yet
- tmp97C8 TMPDocument9 pagestmp97C8 TMPFrontiersNo ratings yet
- Anatomy GlossaryDocument132 pagesAnatomy GlossaryMansoor ShahzadNo ratings yet
- Activity 1.1 Journey of A Breath of AirDocument4 pagesActivity 1.1 Journey of A Breath of AirJorjette Kate BatuNo ratings yet
- Immunology in Haematology (Part 1)Document48 pagesImmunology in Haematology (Part 1)kiedd_04100% (4)
- Uterine ProlapseDocument45 pagesUterine ProlapseAnusree AnusreervNo ratings yet
- Care Management of Small RuminantDocument29 pagesCare Management of Small RuminantstvjbjbNo ratings yet
- Bot Fly Larvae: The Bot: More Than A PestDocument3 pagesBot Fly Larvae: The Bot: More Than A PestHerrieNo ratings yet
- Aesthetic and Patient Preference Using A Bone Substitute To Preserve Extraction Sockets Under Pontics. A Cross-Sectional SurveyDocument10 pagesAesthetic and Patient Preference Using A Bone Substitute To Preserve Extraction Sockets Under Pontics. A Cross-Sectional Surveyalmond_pretzelNo ratings yet
- Titan XC Parent HandbookDocument28 pagesTitan XC Parent HandbookTitanXCNo ratings yet
- AnencephalyDocument11 pagesAnencephalyDidi SujanaNo ratings yet
- Pericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerDocument2 pagesPericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerlhenNo ratings yet
- Mantoux Skin TestDocument3 pagesMantoux Skin TestrenjoNo ratings yet
- Renal Diet - NephCure Kidney International ®Document9 pagesRenal Diet - NephCure Kidney International ®Jamal FadeNo ratings yet
- Jurnal Insect Bite PDFDocument4 pagesJurnal Insect Bite PDFjihadahNo ratings yet
- Basic Cardiac Life Support 2011Document6 pagesBasic Cardiac Life Support 2011Tashfeen Bin NazeerNo ratings yet
- Yoga Shatkriya GuideDocument39 pagesYoga Shatkriya Guidesivanarayana nallagatlaNo ratings yet
- Cardiovascular ActivitiesDocument8 pagesCardiovascular ActivitiesJuan RuizNo ratings yet
- Myofunctional ApplianceDocument84 pagesMyofunctional Appliancenikitha100% (1)
- Pauline Cabrera, M.D. Pediatrics Cardinal Santos Medical CenterDocument64 pagesPauline Cabrera, M.D. Pediatrics Cardinal Santos Medical CenterPauline Cabrera-CruzNo ratings yet
- Interpretation of CPET PosterDocument1 pageInterpretation of CPET PosterczukmiklosNo ratings yet
- MCN DX Test 2010Document9 pagesMCN DX Test 2010jjbautista100% (2)
- Man Cattle and VeldDocument7 pagesMan Cattle and Veldlosalburejos62No ratings yet
- Zoology Syllabus CBCSDocument12 pagesZoology Syllabus CBCSACADEMIC PUBLISHERS100% (1)
- Basic Fantasy Field Guide r29Document86 pagesBasic Fantasy Field Guide r29Knightsbridge~No ratings yet
- Observacion y Practica de AferesisDocument296 pagesObservacion y Practica de AferesisWilmer Cruzado CarrascoNo ratings yet
- Pelvis and Perineum (Appleton & Lange Review)Document41 pagesPelvis and Perineum (Appleton & Lange Review)orea100% (2)
- Alyssa Brooks - Breakfast FunDocument3 pagesAlyssa Brooks - Breakfast Fund4d42937No ratings yet