
2011 HMCT Equity Report Final 2
2011 HMCT Equity Report Final 2
You might also like
- Community Needs AssessmentDocument12 pagesCommunity Needs Assessmentrachael costello100% (1)
- HHB Chapter 4 The Nazis Take PowerDocument55 pagesHHB Chapter 4 The Nazis Take PowerJosé Juan Góngora CortésNo ratings yet
- Walaa Network List - 19 November 2019Document76 pagesWalaa Network List - 19 November 2019hafezasad40% (5)
- Classification of Hospitals DOHDocument2 pagesClassification of Hospitals DOHAnjo Aglugub100% (2)
- RWJF Issue BriefDocument4 pagesRWJF Issue BriefiggybauNo ratings yet
- Running Head: Service Learning Project Plan 1Document12 pagesRunning Head: Service Learning Project Plan 1api-238156787No ratings yet
- DiscussionDocument5 pagesDiscussionVivek SuranaNo ratings yet
- Community Assessment 26 Ebi Template WordDocument9 pagesCommunity Assessment 26 Ebi Template Wordapi-641501601No ratings yet
- Final Version of The BME HNA Updated Document 12 March 189460Document294 pagesFinal Version of The BME HNA Updated Document 12 March 189460Mario LanzaNo ratings yet
- Analyzing The Health Disparities in Urban VsDocument10 pagesAnalyzing The Health Disparities in Urban Vsbash5042No ratings yet
- AAFP Letter To Domestic Policy Council 6-10-2020Document3 pagesAAFP Letter To Domestic Policy Council 6-10-2020iggybauNo ratings yet
- The Health of The African American Community in D.C.Document16 pagesThe Health of The African American Community in D.C.Christina Sturdivant100% (1)
- Nur 340 Community Change Group Project Final VersionDocument23 pagesNur 340 Community Change Group Project Final Versionapi-239588178No ratings yet
- Health Disparaties ReportDocument11 pagesHealth Disparaties Reportapi-677763604No ratings yet
- Confronting Health Inequity - The Global DimensionDocument5 pagesConfronting Health Inequity - The Global Dimensionmanique_abeyrat2469No ratings yet
- LGBT Public Health Outcomes Framework CompanionDocument57 pagesLGBT Public Health Outcomes Framework CompanionAurelia AureliaNo ratings yet
- 7h FS-Mainstreaming Gender Perspective PDFDocument4 pages7h FS-Mainstreaming Gender Perspective PDFJairus Joel A. SuminegNo ratings yet
- Declaration Racism As A PH CrisisDocument3 pagesDeclaration Racism As A PH CrisisBarbara GellerNo ratings yet
- Comprehensive Systems ThinkingDocument10 pagesComprehensive Systems ThinkingAnnette Rae SpellmanNo ratings yet
- BNA Executive SummaryDocument23 pagesBNA Executive SummaryMME FTENo ratings yet
- Comm Health NursDocument8 pagesComm Health NursMatt DavidNo ratings yet
- ACCESS Transformed Full ReportDocument40 pagesACCESS Transformed Full ReportMark ReinhardtNo ratings yet
- Health Care's Blind Side PDFDocument12 pagesHealth Care's Blind Side PDFiggybauNo ratings yet
- Nsach Community AssessmentDocument8 pagesNsach Community Assessmentapi-311766385No ratings yet
- Peg Health Equity Report 2015Document24 pagesPeg Health Equity Report 2015Metro English CanadaNo ratings yet
- HB 13-1088: Office of Health Equity CDPHEDocument3 pagesHB 13-1088: Office of Health Equity CDPHESenator Mike JohnstonNo ratings yet
- Document HealthDocument2 pagesDocument HealthHarveyNo ratings yet
- Introduction To Health ResearchDocument22 pagesIntroduction To Health Researchdoreen100% (1)
- Artigo Referencia - Africa - AFHS1101-0108Document8 pagesArtigo Referencia - Africa - AFHS1101-0108Thais CoutinhoNo ratings yet
- Peg Health Equity ReportDocument24 pagesPeg Health Equity ReportChrisDcaNo ratings yet
- Running Head: SBHC Policy Analysis 1Document17 pagesRunning Head: SBHC Policy Analysis 1api-314835119No ratings yet
- The Anatomy of The Philippine Health Care SystemDocument2 pagesThe Anatomy of The Philippine Health Care SystemIra Jane MintarNo ratings yet
- Singer, Judy Qualitative Evaluation of A Community NavajoDocument15 pagesSinger, Judy Qualitative Evaluation of A Community NavajoLuis R HdezNo ratings yet
- RWJFPhysicians Survey Executive SummaryDocument12 pagesRWJFPhysicians Survey Executive SummaryhousingworksNo ratings yet
- CHSI - SequatchieDocument8 pagesCHSI - SequatchieerlangerhealthNo ratings yet
- Chsi Meigs Co.Document8 pagesChsi Meigs Co.erlangerhealthNo ratings yet
- Tillman, Matt Rural Health Care HC Systems Paper (Final)Document17 pagesTillman, Matt Rural Health Care HC Systems Paper (Final)api-282411018No ratings yet
- RoadMAPP Plan - Dec. 5, 2014Document4 pagesRoadMAPP Plan - Dec. 5, 2014Casey JonesNo ratings yet
- Community Diagnosis of The UnicoiDocument11 pagesCommunity Diagnosis of The UnicoikazulamaNo ratings yet
- Teen Pregnancy Group PaperDocument7 pagesTeen Pregnancy Group Paperapi-259018499No ratings yet
- Trends and Innovations in Chronic Disease Prevention TreatmentDocument48 pagesTrends and Innovations in Chronic Disease Prevention TreatmentKrisTina KhaiZer RicoNo ratings yet
- MHP Assesment 2018Document60 pagesMHP Assesment 2018dharry8108No ratings yet
- Responding to Healthcare Reform: A Strategy Guide for Healthcare LeadersFrom EverandResponding to Healthcare Reform: A Strategy Guide for Healthcare LeadersNo ratings yet
- Nys Ahec 2021-22 Sign-On Letter 6.30.21Document2 pagesNys Ahec 2021-22 Sign-On Letter 6.30.21BQLI AHECNo ratings yet
- PIC ASSIGN 1.editedDocument7 pagesPIC ASSIGN 1.editedviennenabo04No ratings yet
- CHSI Polk Co.Document8 pagesCHSI Polk Co.erlangerhealthNo ratings yet
- Capstone SummativeDocument10 pagesCapstone Summativeapi-283153247No ratings yet
- Director of Public Health Annual Report 2011 12 Section1Document34 pagesDirector of Public Health Annual Report 2011 12 Section1Bijay Kumar MahatoNo ratings yet
- Health Aff 2011 Maxwell 1451 60Document11 pagesHealth Aff 2011 Maxwell 1451 60Brennan BollmanNo ratings yet
- Running Head: Policy Action Plan: Health Care Disparities 1Document9 pagesRunning Head: Policy Action Plan: Health Care Disparities 1api-509672908No ratings yet
- Health Promotion and Population HealthDocument39 pagesHealth Promotion and Population HealthSuyanto YantoNo ratings yet
- Oaxaca Health South AfricaDocument13 pagesOaxaca Health South AfricaalelaNo ratings yet
- Preventing Obesity and Promoting Cardiometabolic Health: The Promise and Potential of Policies and The Affordable Care ActDocument5 pagesPreventing Obesity and Promoting Cardiometabolic Health: The Promise and Potential of Policies and The Affordable Care ActKristine Anne SorianoNo ratings yet
- Chap Executive Summary Final2011june16Document7 pagesChap Executive Summary Final2011june16api-130477923No ratings yet
- Draft Proposal - Measuring HospitalsDocument24 pagesDraft Proposal - Measuring HospitalsAli H. MhmdNo ratings yet
- What Is Public HealthDocument13 pagesWhat Is Public HealthHpg HsuNo ratings yet
- 5 Roles and Responsibilities of A Community Health NurseDocument7 pages5 Roles and Responsibilities of A Community Health NurseJULIUS BORDONNo ratings yet
- HMP 601 Midterm PaperDocument4 pagesHMP 601 Midterm PaperDavontae Foxx-DrewNo ratings yet
- Improving Sexual Health - November 2011Document22 pagesImproving Sexual Health - November 2011Chris FindlayNo ratings yet
- Global Health Initiatives 2007 enDocument32 pagesGlobal Health Initiatives 2007 enChristian Anthony CullarinNo ratings yet
- Philippines: Health SystemDocument5 pagesPhilippines: Health SystemmarvinbreyesNo ratings yet
- Cipp ModelDocument34 pagesCipp ModelEricson MitraNo ratings yet
- Person Centered TherapyDocument4 pagesPerson Centered Therapysusanwhitten100% (2)
- Person Centered TherapyDocument4 pagesPerson Centered Therapysusanwhitten100% (2)
- Carl RogersDocument5 pagesCarl Rogerssusanwhitten100% (1)
- Faith Found Expect 2014Document2 pagesFaith Found Expect 2014susanwhittenNo ratings yet
- Buddhism Paper Spring 2013Document1 pageBuddhism Paper Spring 2013susanwhittenNo ratings yet
- A. Mood Disorders: Name: Intro To Psych Module 23 - Mood Disorders and SchizophreniaDocument7 pagesA. Mood Disorders: Name: Intro To Psych Module 23 - Mood Disorders and SchizophreniasusanwhittenNo ratings yet
- FHAO Scope and SequenceDocument1 pageFHAO Scope and SequencesusanwhittenNo ratings yet
- Class Condit UrlDocument1 pageClass Condit UrlsusanwhittenNo ratings yet
- CH 1 Reading Guide Part 1Document2 pagesCH 1 Reading Guide Part 1susanwhittenNo ratings yet
- CH 1 Reading Guide Part 2Document3 pagesCH 1 Reading Guide Part 2susanwhittenNo ratings yet
- Freudian and Humanistic Theories A. Freud's Psychodynamic TheoryDocument5 pagesFreudian and Humanistic Theories A. Freud's Psychodynamic TheorysusanwhittenNo ratings yet
- A. Appraisal: Name: Intro To Psychology Module 21 - Health, Stress, and CopingDocument5 pagesA. Appraisal: Name: Intro To Psychology Module 21 - Health, Stress, and CopingsusanwhittenNo ratings yet
- A. Factors in Mental Disorders: Name: SCORE: - /91 Intro To Psych Module 22-Assessment and Anxiety DisordersDocument4 pagesA. Factors in Mental Disorders: Name: SCORE: - /91 Intro To Psych Module 22-Assessment and Anxiety DisorderssusanwhittenNo ratings yet
- Module 15 Study GuideDocument7 pagesModule 15 Study GuidesusanwhittenNo ratings yet
- Module 10 Study GuideDocument4 pagesModule 10 Study GuidesusanwhittenNo ratings yet
- Infancy and Childhood B. Newborns' Abilities: Name: Score - /137Document6 pagesInfancy and Childhood B. Newborns' Abilities: Name: Score - /137susanwhittenNo ratings yet
- Adolescence & Adulthood B. Cognitive and Emotional Changes: Name: SCORE: - /123Document6 pagesAdolescence & Adulthood B. Cognitive and Emotional Changes: Name: SCORE: - /123susanwhittenNo ratings yet
- A) Peripheral Theories Neuroscience Approaches To Emotions. (Try To Paraphrase and Not Just Copy TheDocument5 pagesA) Peripheral Theories Neuroscience Approaches To Emotions. (Try To Paraphrase and Not Just Copy ThesusanwhittenNo ratings yet
- Module 13 Study Guide-Student VersionDocument5 pagesModule 13 Study Guide-Student VersionsusanwhittenNo ratings yet
- A. Continuum of Consciousness Copied From Book - Paraphrase or Just List Words or Phrases That Help You Recall What These Terms Mean)Document7 pagesA. Continuum of Consciousness Copied From Book - Paraphrase or Just List Words or Phrases That Help You Recall What These Terms Mean)susanwhittenNo ratings yet
- Conformity and ObedienceDocument43 pagesConformity and ObediencesusanwhittenNo ratings yet
- Module 9 ReadingGuideDocument4 pagesModule 9 ReadingGuidesusanwhittenNo ratings yet
- Introduction To Psychology: Mrs. Snodgrass Office: 255 Taylor / Classroom: 241 Buckman / 901-537-1429Document2 pagesIntroduction To Psychology: Mrs. Snodgrass Office: 255 Taylor / Classroom: 241 Buckman / 901-537-1429susanwhittenNo ratings yet
- HHB ch8 0Document55 pagesHHB ch8 0susanwhittenNo ratings yet
- HHB ch3Document45 pagesHHB ch3susanwhittenNo ratings yet
- Supervision and The Johari Window: A Framework For Asking QuestionsDocument6 pagesSupervision and The Johari Window: A Framework For Asking QuestionsGarfield PosternNo ratings yet
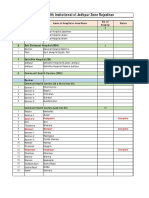
- Medical Health Insitutional of Jodhpur Zone Rajasthan: District Hospital (DH)Document3 pagesMedical Health Insitutional of Jodhpur Zone Rajasthan: District Hospital (DH)Vishnu PrajapatiNo ratings yet
- PrimaryCare JAWDA - Update 2022Document40 pagesPrimaryCare JAWDA - Update 2022SECRIVINo ratings yet
- List of HospitalDocument61 pagesList of HospitalConsuelo Narag GalagalaNo ratings yet
- Levels of Health Care BHM - 105Document3 pagesLevels of Health Care BHM - 105black roseNo ratings yet
- A Comprehensive CRM Strategy For AstraZenecaDocument15 pagesA Comprehensive CRM Strategy For AstraZenecasabaarehman7No ratings yet
- Marier - ST Onge 510essayDocument7 pagesMarier - ST Onge 510essayGenevieveMarierSt-OngeNo ratings yet
- Historical SupplyDocument5 pagesHistorical Supplylara torricoNo ratings yet
- Measuring Up 2018Document80 pagesMeasuring Up 2018CityNewsTorontoNo ratings yet
- Community Oriented Primary Care COPC in District Health Services of Gauteng South AfricaDocument4 pagesCommunity Oriented Primary Care COPC in District Health Services of Gauteng South AfricaKim G. SarongNo ratings yet
- BlueDocument94 pagesBluemht1No ratings yet
- Nursing Care ModelDocument7 pagesNursing Care ModelRobin Ravenel100% (1)
- Canadian Personal Care Provider Canadian 1st Edition Wolgin Solutions ManualDocument36 pagesCanadian Personal Care Provider Canadian 1st Edition Wolgin Solutions Manualampyxprimei5136100% (18)
- Rodwin - The French Health Care SystemDocument7 pagesRodwin - The French Health Care SystemChris HarrisNo ratings yet
- Aster Group CoDocument3 pagesAster Group Coeason insightsNo ratings yet
- The Role of Social Work in Integrated Health: Judith Anne Debonis PHDDocument66 pagesThe Role of Social Work in Integrated Health: Judith Anne Debonis PHDGouri BhosaleNo ratings yet
- RetrieveDocument8 pagesRetrieveSahian Montserrat Angeles HortaNo ratings yet
- Provider List 011121Document7 pagesProvider List 011121Titilayomi Ehire100% (1)
- Provider - Networks Rajhi TakafulDocument10 pagesProvider - Networks Rajhi Takafulumair baigNo ratings yet
- Spring / Summer 2011 Annual ReportDocument40 pagesSpring / Summer 2011 Annual ReportCCHSNo ratings yet
- Effect of Trust in Primary Care Physicians On Patient Satisfaction: A Cross-Sectional Study Among Patients With Hypertension in Rural ChinaDocument13 pagesEffect of Trust in Primary Care Physicians On Patient Satisfaction: A Cross-Sectional Study Among Patients With Hypertension in Rural ChinarachelzefanyaNo ratings yet
- Business LettersDocument39 pagesBusiness Lettersjdvroxas100% (1)
- CHN Transes Week 2Document2 pagesCHN Transes Week 2cheskalyka.asiloNo ratings yet
- ICPC User GuideDocument54 pagesICPC User GuidePkts Universitas Duta BangsaNo ratings yet
- Current and Updated Provider List January 2021Document105 pagesCurrent and Updated Provider List January 2021Maverick ChukwuNo ratings yet
- Why You Need To Be A Systems Thinker in Health CareDocument3 pagesWhy You Need To Be A Systems Thinker in Health CareBhavik PrajapatiNo ratings yet
- GPPAQ - GuidanceDocument22 pagesGPPAQ - Guidancesfs_idxNo ratings yet
- Whitepaper TH Canadian Virtual Care Landscape-EnDocument11 pagesWhitepaper TH Canadian Virtual Care Landscape-Enalaric7nurmNo ratings yet


















































































































Download as pdf or txt
You might also like
- Community Needs AssessmentDocument12 pagesCommunity Needs Assessmentrachael costello100% (1)
- HHB Chapter 4 The Nazis Take PowerDocument55 pagesHHB Chapter 4 The Nazis Take PowerJosé Juan Góngora CortésNo ratings yet
- Walaa Network List - 19 November 2019Document76 pagesWalaa Network List - 19 November 2019hafezasad40% (5)
- Classification of Hospitals DOHDocument2 pagesClassification of Hospitals DOHAnjo Aglugub100% (2)
- RWJF Issue BriefDocument4 pagesRWJF Issue BriefiggybauNo ratings yet
- Running Head: Service Learning Project Plan 1Document12 pagesRunning Head: Service Learning Project Plan 1api-238156787No ratings yet
- DiscussionDocument5 pagesDiscussionVivek SuranaNo ratings yet
- Community Assessment 26 Ebi Template WordDocument9 pagesCommunity Assessment 26 Ebi Template Wordapi-641501601No ratings yet
- Final Version of The BME HNA Updated Document 12 March 189460Document294 pagesFinal Version of The BME HNA Updated Document 12 March 189460Mario LanzaNo ratings yet
- Analyzing The Health Disparities in Urban VsDocument10 pagesAnalyzing The Health Disparities in Urban Vsbash5042No ratings yet
- AAFP Letter To Domestic Policy Council 6-10-2020Document3 pagesAAFP Letter To Domestic Policy Council 6-10-2020iggybauNo ratings yet
- The Health of The African American Community in D.C.Document16 pagesThe Health of The African American Community in D.C.Christina Sturdivant100% (1)
- Nur 340 Community Change Group Project Final VersionDocument23 pagesNur 340 Community Change Group Project Final Versionapi-239588178No ratings yet
- Health Disparaties ReportDocument11 pagesHealth Disparaties Reportapi-677763604No ratings yet
- Confronting Health Inequity - The Global DimensionDocument5 pagesConfronting Health Inequity - The Global Dimensionmanique_abeyrat2469No ratings yet
- LGBT Public Health Outcomes Framework CompanionDocument57 pagesLGBT Public Health Outcomes Framework CompanionAurelia AureliaNo ratings yet
- 7h FS-Mainstreaming Gender Perspective PDFDocument4 pages7h FS-Mainstreaming Gender Perspective PDFJairus Joel A. SuminegNo ratings yet
- Declaration Racism As A PH CrisisDocument3 pagesDeclaration Racism As A PH CrisisBarbara GellerNo ratings yet
- Comprehensive Systems ThinkingDocument10 pagesComprehensive Systems ThinkingAnnette Rae SpellmanNo ratings yet
- BNA Executive SummaryDocument23 pagesBNA Executive SummaryMME FTENo ratings yet
- Comm Health NursDocument8 pagesComm Health NursMatt DavidNo ratings yet
- ACCESS Transformed Full ReportDocument40 pagesACCESS Transformed Full ReportMark ReinhardtNo ratings yet
- Health Care's Blind Side PDFDocument12 pagesHealth Care's Blind Side PDFiggybauNo ratings yet
- Nsach Community AssessmentDocument8 pagesNsach Community Assessmentapi-311766385No ratings yet
- Peg Health Equity Report 2015Document24 pagesPeg Health Equity Report 2015Metro English CanadaNo ratings yet
- HB 13-1088: Office of Health Equity CDPHEDocument3 pagesHB 13-1088: Office of Health Equity CDPHESenator Mike JohnstonNo ratings yet
- Document HealthDocument2 pagesDocument HealthHarveyNo ratings yet
- Introduction To Health ResearchDocument22 pagesIntroduction To Health Researchdoreen100% (1)
- Artigo Referencia - Africa - AFHS1101-0108Document8 pagesArtigo Referencia - Africa - AFHS1101-0108Thais CoutinhoNo ratings yet
- Peg Health Equity ReportDocument24 pagesPeg Health Equity ReportChrisDcaNo ratings yet
- Running Head: SBHC Policy Analysis 1Document17 pagesRunning Head: SBHC Policy Analysis 1api-314835119No ratings yet
- The Anatomy of The Philippine Health Care SystemDocument2 pagesThe Anatomy of The Philippine Health Care SystemIra Jane MintarNo ratings yet
- Singer, Judy Qualitative Evaluation of A Community NavajoDocument15 pagesSinger, Judy Qualitative Evaluation of A Community NavajoLuis R HdezNo ratings yet
- RWJFPhysicians Survey Executive SummaryDocument12 pagesRWJFPhysicians Survey Executive SummaryhousingworksNo ratings yet
- CHSI - SequatchieDocument8 pagesCHSI - SequatchieerlangerhealthNo ratings yet
- Chsi Meigs Co.Document8 pagesChsi Meigs Co.erlangerhealthNo ratings yet
- Tillman, Matt Rural Health Care HC Systems Paper (Final)Document17 pagesTillman, Matt Rural Health Care HC Systems Paper (Final)api-282411018No ratings yet
- RoadMAPP Plan - Dec. 5, 2014Document4 pagesRoadMAPP Plan - Dec. 5, 2014Casey JonesNo ratings yet
- Community Diagnosis of The UnicoiDocument11 pagesCommunity Diagnosis of The UnicoikazulamaNo ratings yet
- Teen Pregnancy Group PaperDocument7 pagesTeen Pregnancy Group Paperapi-259018499No ratings yet
- Trends and Innovations in Chronic Disease Prevention TreatmentDocument48 pagesTrends and Innovations in Chronic Disease Prevention TreatmentKrisTina KhaiZer RicoNo ratings yet
- MHP Assesment 2018Document60 pagesMHP Assesment 2018dharry8108No ratings yet
- Responding to Healthcare Reform: A Strategy Guide for Healthcare LeadersFrom EverandResponding to Healthcare Reform: A Strategy Guide for Healthcare LeadersNo ratings yet
- Nys Ahec 2021-22 Sign-On Letter 6.30.21Document2 pagesNys Ahec 2021-22 Sign-On Letter 6.30.21BQLI AHECNo ratings yet
- PIC ASSIGN 1.editedDocument7 pagesPIC ASSIGN 1.editedviennenabo04No ratings yet
- CHSI Polk Co.Document8 pagesCHSI Polk Co.erlangerhealthNo ratings yet
- Capstone SummativeDocument10 pagesCapstone Summativeapi-283153247No ratings yet
- Director of Public Health Annual Report 2011 12 Section1Document34 pagesDirector of Public Health Annual Report 2011 12 Section1Bijay Kumar MahatoNo ratings yet
- Health Aff 2011 Maxwell 1451 60Document11 pagesHealth Aff 2011 Maxwell 1451 60Brennan BollmanNo ratings yet
- Running Head: Policy Action Plan: Health Care Disparities 1Document9 pagesRunning Head: Policy Action Plan: Health Care Disparities 1api-509672908No ratings yet
- Health Promotion and Population HealthDocument39 pagesHealth Promotion and Population HealthSuyanto YantoNo ratings yet
- Oaxaca Health South AfricaDocument13 pagesOaxaca Health South AfricaalelaNo ratings yet
- Preventing Obesity and Promoting Cardiometabolic Health: The Promise and Potential of Policies and The Affordable Care ActDocument5 pagesPreventing Obesity and Promoting Cardiometabolic Health: The Promise and Potential of Policies and The Affordable Care ActKristine Anne SorianoNo ratings yet
- Chap Executive Summary Final2011june16Document7 pagesChap Executive Summary Final2011june16api-130477923No ratings yet
- Draft Proposal - Measuring HospitalsDocument24 pagesDraft Proposal - Measuring HospitalsAli H. MhmdNo ratings yet
- What Is Public HealthDocument13 pagesWhat Is Public HealthHpg HsuNo ratings yet
- 5 Roles and Responsibilities of A Community Health NurseDocument7 pages5 Roles and Responsibilities of A Community Health NurseJULIUS BORDONNo ratings yet
- HMP 601 Midterm PaperDocument4 pagesHMP 601 Midterm PaperDavontae Foxx-DrewNo ratings yet
- Improving Sexual Health - November 2011Document22 pagesImproving Sexual Health - November 2011Chris FindlayNo ratings yet
- Global Health Initiatives 2007 enDocument32 pagesGlobal Health Initiatives 2007 enChristian Anthony CullarinNo ratings yet
- Philippines: Health SystemDocument5 pagesPhilippines: Health SystemmarvinbreyesNo ratings yet
- Cipp ModelDocument34 pagesCipp ModelEricson MitraNo ratings yet
- Person Centered TherapyDocument4 pagesPerson Centered Therapysusanwhitten100% (2)
- Person Centered TherapyDocument4 pagesPerson Centered Therapysusanwhitten100% (2)
- Carl RogersDocument5 pagesCarl Rogerssusanwhitten100% (1)
- Faith Found Expect 2014Document2 pagesFaith Found Expect 2014susanwhittenNo ratings yet
- Buddhism Paper Spring 2013Document1 pageBuddhism Paper Spring 2013susanwhittenNo ratings yet
- A. Mood Disorders: Name: Intro To Psych Module 23 - Mood Disorders and SchizophreniaDocument7 pagesA. Mood Disorders: Name: Intro To Psych Module 23 - Mood Disorders and SchizophreniasusanwhittenNo ratings yet
- FHAO Scope and SequenceDocument1 pageFHAO Scope and SequencesusanwhittenNo ratings yet
- Class Condit UrlDocument1 pageClass Condit UrlsusanwhittenNo ratings yet
- CH 1 Reading Guide Part 1Document2 pagesCH 1 Reading Guide Part 1susanwhittenNo ratings yet
- CH 1 Reading Guide Part 2Document3 pagesCH 1 Reading Guide Part 2susanwhittenNo ratings yet
- Freudian and Humanistic Theories A. Freud's Psychodynamic TheoryDocument5 pagesFreudian and Humanistic Theories A. Freud's Psychodynamic TheorysusanwhittenNo ratings yet
- A. Appraisal: Name: Intro To Psychology Module 21 - Health, Stress, and CopingDocument5 pagesA. Appraisal: Name: Intro To Psychology Module 21 - Health, Stress, and CopingsusanwhittenNo ratings yet
- A. Factors in Mental Disorders: Name: SCORE: - /91 Intro To Psych Module 22-Assessment and Anxiety DisordersDocument4 pagesA. Factors in Mental Disorders: Name: SCORE: - /91 Intro To Psych Module 22-Assessment and Anxiety DisorderssusanwhittenNo ratings yet
- Module 15 Study GuideDocument7 pagesModule 15 Study GuidesusanwhittenNo ratings yet
- Module 10 Study GuideDocument4 pagesModule 10 Study GuidesusanwhittenNo ratings yet
- Infancy and Childhood B. Newborns' Abilities: Name: Score - /137Document6 pagesInfancy and Childhood B. Newborns' Abilities: Name: Score - /137susanwhittenNo ratings yet
- Adolescence & Adulthood B. Cognitive and Emotional Changes: Name: SCORE: - /123Document6 pagesAdolescence & Adulthood B. Cognitive and Emotional Changes: Name: SCORE: - /123susanwhittenNo ratings yet
- A) Peripheral Theories Neuroscience Approaches To Emotions. (Try To Paraphrase and Not Just Copy TheDocument5 pagesA) Peripheral Theories Neuroscience Approaches To Emotions. (Try To Paraphrase and Not Just Copy ThesusanwhittenNo ratings yet
- Module 13 Study Guide-Student VersionDocument5 pagesModule 13 Study Guide-Student VersionsusanwhittenNo ratings yet
- A. Continuum of Consciousness Copied From Book - Paraphrase or Just List Words or Phrases That Help You Recall What These Terms Mean)Document7 pagesA. Continuum of Consciousness Copied From Book - Paraphrase or Just List Words or Phrases That Help You Recall What These Terms Mean)susanwhittenNo ratings yet
- Conformity and ObedienceDocument43 pagesConformity and ObediencesusanwhittenNo ratings yet
- Module 9 ReadingGuideDocument4 pagesModule 9 ReadingGuidesusanwhittenNo ratings yet
- Introduction To Psychology: Mrs. Snodgrass Office: 255 Taylor / Classroom: 241 Buckman / 901-537-1429Document2 pagesIntroduction To Psychology: Mrs. Snodgrass Office: 255 Taylor / Classroom: 241 Buckman / 901-537-1429susanwhittenNo ratings yet
- HHB ch8 0Document55 pagesHHB ch8 0susanwhittenNo ratings yet
- HHB ch3Document45 pagesHHB ch3susanwhittenNo ratings yet
- Supervision and The Johari Window: A Framework For Asking QuestionsDocument6 pagesSupervision and The Johari Window: A Framework For Asking QuestionsGarfield PosternNo ratings yet
- Medical Health Insitutional of Jodhpur Zone Rajasthan: District Hospital (DH)Document3 pagesMedical Health Insitutional of Jodhpur Zone Rajasthan: District Hospital (DH)Vishnu PrajapatiNo ratings yet
- PrimaryCare JAWDA - Update 2022Document40 pagesPrimaryCare JAWDA - Update 2022SECRIVINo ratings yet
- List of HospitalDocument61 pagesList of HospitalConsuelo Narag GalagalaNo ratings yet
- Levels of Health Care BHM - 105Document3 pagesLevels of Health Care BHM - 105black roseNo ratings yet
- A Comprehensive CRM Strategy For AstraZenecaDocument15 pagesA Comprehensive CRM Strategy For AstraZenecasabaarehman7No ratings yet
- Marier - ST Onge 510essayDocument7 pagesMarier - ST Onge 510essayGenevieveMarierSt-OngeNo ratings yet
- Historical SupplyDocument5 pagesHistorical Supplylara torricoNo ratings yet
- Measuring Up 2018Document80 pagesMeasuring Up 2018CityNewsTorontoNo ratings yet
- Community Oriented Primary Care COPC in District Health Services of Gauteng South AfricaDocument4 pagesCommunity Oriented Primary Care COPC in District Health Services of Gauteng South AfricaKim G. SarongNo ratings yet
- BlueDocument94 pagesBluemht1No ratings yet
- Nursing Care ModelDocument7 pagesNursing Care ModelRobin Ravenel100% (1)
- Canadian Personal Care Provider Canadian 1st Edition Wolgin Solutions ManualDocument36 pagesCanadian Personal Care Provider Canadian 1st Edition Wolgin Solutions Manualampyxprimei5136100% (18)
- Rodwin - The French Health Care SystemDocument7 pagesRodwin - The French Health Care SystemChris HarrisNo ratings yet
- Aster Group CoDocument3 pagesAster Group Coeason insightsNo ratings yet
- The Role of Social Work in Integrated Health: Judith Anne Debonis PHDDocument66 pagesThe Role of Social Work in Integrated Health: Judith Anne Debonis PHDGouri BhosaleNo ratings yet
- RetrieveDocument8 pagesRetrieveSahian Montserrat Angeles HortaNo ratings yet
- Provider List 011121Document7 pagesProvider List 011121Titilayomi Ehire100% (1)
- Provider - Networks Rajhi TakafulDocument10 pagesProvider - Networks Rajhi Takafulumair baigNo ratings yet
- Spring / Summer 2011 Annual ReportDocument40 pagesSpring / Summer 2011 Annual ReportCCHSNo ratings yet
- Effect of Trust in Primary Care Physicians On Patient Satisfaction: A Cross-Sectional Study Among Patients With Hypertension in Rural ChinaDocument13 pagesEffect of Trust in Primary Care Physicians On Patient Satisfaction: A Cross-Sectional Study Among Patients With Hypertension in Rural ChinarachelzefanyaNo ratings yet
- Business LettersDocument39 pagesBusiness Lettersjdvroxas100% (1)
- CHN Transes Week 2Document2 pagesCHN Transes Week 2cheskalyka.asiloNo ratings yet
- ICPC User GuideDocument54 pagesICPC User GuidePkts Universitas Duta BangsaNo ratings yet
- Current and Updated Provider List January 2021Document105 pagesCurrent and Updated Provider List January 2021Maverick ChukwuNo ratings yet
- Why You Need To Be A Systems Thinker in Health CareDocument3 pagesWhy You Need To Be A Systems Thinker in Health CareBhavik PrajapatiNo ratings yet
- GPPAQ - GuidanceDocument22 pagesGPPAQ - Guidancesfs_idxNo ratings yet
- Whitepaper TH Canadian Virtual Care Landscape-EnDocument11 pagesWhitepaper TH Canadian Virtual Care Landscape-Enalaric7nurmNo ratings yet