Download as pdf or txt
You might also like
- Mapeh Least Learned Competencies 6Document5 pagesMapeh Least Learned Competencies 6Anonymous QnNICuArTx75% (12)
- Existential Therapy ActivityDocument3 pagesExistential Therapy ActivityMaria Isabel CornelioNo ratings yet
- Meilleur, A.-A. S., Jelenic, P., & Mottron, L. (2015) - Prevalence of Clinically and Empirically Defined Talents and Strengths in AutismDocument14 pagesMeilleur, A.-A. S., Jelenic, P., & Mottron, L. (2015) - Prevalence of Clinically and Empirically Defined Talents and Strengths in AutismTomislav CvrtnjakNo ratings yet
- Personality Assignment Final !!!Document8 pagesPersonality Assignment Final !!!Chloe SaundersNo ratings yet
- Corsini - Existential PsychotherapyDocument5 pagesCorsini - Existential Psychotherapynini345No ratings yet
- Detailed History and Description of Transactional AnalysisDocument8 pagesDetailed History and Description of Transactional AnalysisWinda WidyantyNo ratings yet
- Robert WallersteinDocument26 pagesRobert WallersteinRocio Trinidad100% (1)
- HinshelwoodR.D TransferenceDocument8 pagesHinshelwoodR.D TransferenceCecilia RoblesNo ratings yet
- Comments On DR - Frankl's PaperDocument6 pagesComments On DR - Frankl's Paperecodoma100% (1)
- THOMSON - Normativity PDFDocument3 pagesTHOMSON - Normativity PDFlacanilla quegoteaNo ratings yet
- Mindfulness and Psychoanalytic Psychotherapy: A Clinical Convergence.Document13 pagesMindfulness and Psychoanalytic Psychotherapy: A Clinical Convergence.IngridSusuMood100% (1)
- Nursing Care Plan For Interrupted Breastfeeding NCPDocument3 pagesNursing Care Plan For Interrupted Breastfeeding NCPderic88% (8)
- Plavix ClopidogrelDocument2 pagesPlavix ClopidogrelAdrianne Bazo50% (2)
- Explore - Neural and Cognitive Basis of Spiritual ExperienceDocument10 pagesExplore - Neural and Cognitive Basis of Spiritual ExperienceVanessa Leal100% (1)
- A Practical Application of Personal Existential Analysis (Alfried Längle)Document15 pagesA Practical Application of Personal Existential Analysis (Alfried Längle)abaeram2100% (1)
- Ferenczi, S. (1930) - The Principle of Relaxation and Neocatharsis. Int. J. Psycho-AnalDocument12 pagesFerenczi, S. (1930) - The Principle of Relaxation and Neocatharsis. Int. J. Psycho-AnalCiprian Jurma100% (1)
- The Dark Night of The SoulDocument14 pagesThe Dark Night of The SoulIsabelMargaritaJordánNo ratings yet
- Psychotherapy As Personal ConfessionDocument70 pagesPsychotherapy As Personal Confessionazoth7No ratings yet
- Lce V3.2Document8 pagesLce V3.2igarathNo ratings yet
- PSPA3714 Chapter 3 2021Document65 pagesPSPA3714 Chapter 3 2021Kamogelo MakhuraNo ratings yet
- The Phenomenology of Intersubjectivity in Bipolar Disorder and SquizophreniaDocument9 pagesThe Phenomenology of Intersubjectivity in Bipolar Disorder and Squizophreniajanettst2No ratings yet
- Susan Sugarman - Freud's Interpretation of Dreams - A Reappraisal-Cambridge University Press (2022)Document195 pagesSusan Sugarman - Freud's Interpretation of Dreams - A Reappraisal-Cambridge University Press (2022)Rodolfo Ferronatto De SouzaNo ratings yet
- Joe Mannath-Where Have We Gone WrongDocument3 pagesJoe Mannath-Where Have We Gone WrongJMannathNo ratings yet
- Carpy - Tolerating The CountertransferenceDocument8 pagesCarpy - Tolerating The CountertransferenceEl Karmo San100% (1)
- Carl Jung SummaryDocument9 pagesCarl Jung SummaryJunna Alitagtag100% (1)
- Person-Centered Theory: Carl RogersDocument8 pagesPerson-Centered Theory: Carl RogersKenNo ratings yet
- Fromm's Humanistic Psychoanalysis - Case StudyDocument6 pagesFromm's Humanistic Psychoanalysis - Case StudyLily ManobanNo ratings yet
- Psychological Types - Carl JungDocument4 pagesPsychological Types - Carl JunglaconuniNo ratings yet
- Essentials of PsychoanalysisDocument16 pagesEssentials of Psychoanalysisbrisamaritima56No ratings yet
- Freud - PsychoanalysisDocument80 pagesFreud - PsychoanalysisSafira YulfaNo ratings yet
- Psychophysiologic Self-Regulation and Human Potential: TheoreticalDocument17 pagesPsychophysiologic Self-Regulation and Human Potential: TheoreticalAndrea BertocchiNo ratings yet
- Freud Returns8Document8 pagesFreud Returns8Dimitris KatsidoniotisNo ratings yet
- (2008) Frosh & Baraister Psychoanalysis - and - Psychosocial - StudiesDocument21 pages(2008) Frosh & Baraister Psychoanalysis - and - Psychosocial - StudiesAndreia Almeida100% (1)
- Tattooing The Body, Marking CultureDocument15 pagesTattooing The Body, Marking CultureLiliana AndreeaNo ratings yet
- Fromm's Therapeutic Approach PDFDocument7 pagesFromm's Therapeutic Approach PDFskanzeniNo ratings yet
- Psychoanalysis Theory and PracticeDocument30 pagesPsychoanalysis Theory and PracticeYexalen ZazilNo ratings yet
- PDF-3 Psychodynamic ModelDocument37 pagesPDF-3 Psychodynamic ModelChinmayi C SNo ratings yet
- Pathological Guilt7!2!09 ACP Revision DrafttDocument17 pagesPathological Guilt7!2!09 ACP Revision DrafttLeslie ShapiroNo ratings yet
- Hoffman - The Myths of Free AssociationDocument20 pagesHoffman - The Myths of Free Association10961408No ratings yet
- Displacing CastrationDocument27 pagesDisplacing Castrationamiller1987No ratings yet
- THE TRANSPERSONAL REVOLUTION FundamentalDocument59 pagesTHE TRANSPERSONAL REVOLUTION FundamentalRamon Enrique Hinostroza GutierrezNo ratings yet
- Freud Interpretation of DreamsDocument445 pagesFreud Interpretation of DreamsHassaan MemonNo ratings yet
- On Existential TherapyDocument22 pagesOn Existential TherapyIan Rory Owen100% (1)
- Running Head: Understanding Personality 1Document10 pagesRunning Head: Understanding Personality 1TigreoeilNo ratings yet
- Sentence Starters, Transitional and Other Useful WordsDocument4 pagesSentence Starters, Transitional and Other Useful WordsPichay BunsoyNo ratings yet
- Journal2011 - I5 - Gestalt JournalDocument82 pagesJournal2011 - I5 - Gestalt JournalIrena JurjevicNo ratings yet
- L'Express - Interview With Jacques LacanDocument12 pagesL'Express - Interview With Jacques LacanBananna LaFleur100% (1)
- American Journal of Psychoanalysis - HappinessDocument20 pagesAmerican Journal of Psychoanalysis - HappinessJeremy De Chavez100% (1)
- Person - Centered TheoryDocument72 pagesPerson - Centered TheoryKatox RafalNo ratings yet
- Acceptance and Commitment Therapy ModelDocument31 pagesAcceptance and Commitment Therapy ModelSusana FossaNo ratings yet
- Ernesto Spinelli Practising Existential PDFDocument4 pagesErnesto Spinelli Practising Existential PDFJulie Re50% (2)
- Psychodynamic Diagnostic ManualDocument6 pagesPsychodynamic Diagnostic Manualas9as9as9as9No ratings yet
- Three Legs of The Practitioner's (Skovholt & Starkey 2010)Document6 pagesThree Legs of The Practitioner's (Skovholt & Starkey 2010)Mia Valdes100% (1)
- WhatworksDocument8 pagesWhatworksapi-353789688No ratings yet
- Gestalt FinalDocument25 pagesGestalt FinalDeeksha WaliaNo ratings yet
- Dynamics and Theories of PersonalityDocument12 pagesDynamics and Theories of PersonalityBiswas AruNo ratings yet
- The Biopsychosocial Model in Psychiatry A CritiqueDocument8 pagesThe Biopsychosocial Model in Psychiatry A CritiquePetar DimkovNo ratings yet
- Humanistic Psychoanalysis PDFDocument29 pagesHumanistic Psychoanalysis PDFAriel Pollak100% (1)
- Eastern PsychotherapiesDocument54 pagesEastern PsychotherapiesVeera Balaji Kumar100% (1)
- Existential Psychology: Rollo Reese MayDocument2 pagesExistential Psychology: Rollo Reese MayRustumme Mirelle Reyes100% (1)
- Historical Women in Psychology - Karen HorneyDocument7 pagesHistorical Women in Psychology - Karen HorneyDenny DailNo ratings yet
- Asphalt - MC 800 (Superior) - Superior Refining Company, LLC (Husky Energy)Document11 pagesAsphalt - MC 800 (Superior) - Superior Refining Company, LLC (Husky Energy)Lindsey BondNo ratings yet
- Literature ReviewDocument13 pagesLiterature ReviewMaxine VirayNo ratings yet
- Biopsychosocial and Interventions PaperDocument13 pagesBiopsychosocial and Interventions Paperapi-272668024No ratings yet
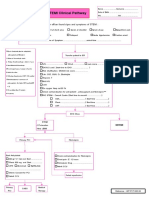
- STEMI Clinical PathwayDocument1 pageSTEMI Clinical PathwayKanoknun PisitpatcaragulNo ratings yet
- COMMISSION ON HIGHER EDUCATION (CHED) Medtech Laws PHDocument2 pagesCOMMISSION ON HIGHER EDUCATION (CHED) Medtech Laws PHJohn Michael CastroNo ratings yet
- NCP Seizure FinalDocument4 pagesNCP Seizure FinalLyrechel de GuzmanNo ratings yet
- Sos CVDocument4 pagesSos CVKaafiya IsaaqNo ratings yet
- CXC Social Studies Sba 2023Document27 pagesCXC Social Studies Sba 2023David DillonNo ratings yet
- David Montgomery MD PHD BioDocument2 pagesDavid Montgomery MD PHD Biolilsowell89No ratings yet
- DSM Diagnostic CodesDocument6 pagesDSM Diagnostic CodesEdward Usca GamarraNo ratings yet
- Initial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentDocument3 pagesInitial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentLamNo ratings yet
- Photo TherapyDocument7 pagesPhoto TherapyMaysa Ismail100% (1)
- Bilchitz and Landau - The Evolution of The Separation of PowersDocument146 pagesBilchitz and Landau - The Evolution of The Separation of PowersJose Almanza MacedoNo ratings yet
- Analysis Aiapget 2018Document4 pagesAnalysis Aiapget 2018arpit sachanNo ratings yet
- Attitude Towards Second Hand Smoke, Smoking and QuitingDocument5 pagesAttitude Towards Second Hand Smoke, Smoking and QuitingBaonganNo ratings yet
- Kishore AccountsDocument8 pagesKishore AccountskishoreNo ratings yet
- Community Pharmacy ActivitiesDocument15 pagesCommunity Pharmacy ActivitiesSha-Ad KaytingNo ratings yet
- Alcoholism Clin Exp Res 2023 Didier Holding Your Liquor Comparison of Alcoholinduced Psychomotor Impairment inDocument11 pagesAlcoholism Clin Exp Res 2023 Didier Holding Your Liquor Comparison of Alcoholinduced Psychomotor Impairment injhasperandaya4No ratings yet
- Mapeh 8health q3 Summative TestDocument3 pagesMapeh 8health q3 Summative TestJanmae ImperialNo ratings yet
- Medical Reimbursement AptranscoDocument13 pagesMedical Reimbursement AptranscopenusilaNo ratings yet
- IntroductionDocument5 pagesIntroductionPaul OrbinoNo ratings yet
- Management of Patients Receiving Local Anaesthesia 2021Document76 pagesManagement of Patients Receiving Local Anaesthesia 2021Micheal ShawkyNo ratings yet
- Ubretid 5mg Tablets PIDocument3 pagesUbretid 5mg Tablets PInovitalumintusariNo ratings yet
- Clodinafop - Msds PDFDocument6 pagesClodinafop - Msds PDFMishra KewalNo ratings yet
- SHE List DocumentDocument1 pageSHE List DocumentMunajamNo ratings yet
- INDIA - NRHM Common Review Mission - Fifth ReportDocument252 pagesINDIA - NRHM Common Review Mission - Fifth ReportKaushik BanerjeeNo ratings yet
- ISAAL 2020 Literary Contests-Pliant 14Document6 pagesISAAL 2020 Literary Contests-Pliant 14Noli CalderonNo ratings yet