Download as pdf or txt
You might also like
- Citrate CRRT Anticoagulation ProtocolDocument5 pagesCitrate CRRT Anticoagulation ProtocolXavi AnpiNo ratings yet
- ICU Note Writing GuidelinesDocument2 pagesICU Note Writing GuidelinesMohammedNo ratings yet
- Shocks MCQDocument6 pagesShocks MCQJaya Krishna Naidu100% (1)
- Clinical Presentation: Home Books Journals Flying Publisher Guides Flying PublisherDocument15 pagesClinical Presentation: Home Books Journals Flying Publisher Guides Flying PublisherDrbhavin PatelNo ratings yet
- بحث الروماتيزم-1Document11 pagesبحث الروماتيزم-1ahmed.omer222555No ratings yet
- Fever in Older PersonsDocument9 pagesFever in Older PersonsKaya Kanti AltaNo ratings yet
- Viral MyocarditisDocument42 pagesViral MyocarditisAlishba AtifNo ratings yet
- F - CMCRep 1 Assy Et Al - 1405Document2 pagesF - CMCRep 1 Assy Et Al - 1405faegrerh5ju75yu34yNo ratings yet
- RigorsDocument3 pagesRigorsLina HasbiNo ratings yet
- Aseptic MeningitisDocument4 pagesAseptic MeningitisCheng XinvennNo ratings yet
- Isolated Thrombocytopenia A Rare Presenting Feature of Enteric FeverDocument2 pagesIsolated Thrombocytopenia A Rare Presenting Feature of Enteric FeverputiridhaNo ratings yet
- CPH Rabbit ReportDocument30 pagesCPH Rabbit ReportClarissa IsuriñaNo ratings yet
- L. Ari Jutkowitz, VMD, DACVECC Michigan State University East Lansing, MI, USADocument5 pagesL. Ari Jutkowitz, VMD, DACVECC Michigan State University East Lansing, MI, USAyoedanuxNo ratings yet
- Ans Fon Ist SemDocument3 pagesAns Fon Ist SemVaishali SinghNo ratings yet
- On Rheumatic FeverDocument30 pagesOn Rheumatic Feverkiran kumari yadav100% (1)
- Rheumatic FeverDocument27 pagesRheumatic FeverMalueth AnguiNo ratings yet
- Approach To The Adult With Fever of Unknown Origin - UpToDateDocument23 pagesApproach To The Adult With Fever of Unknown Origin - UpToDatecrlajnmNo ratings yet
- Level of Evidence 3Document4 pagesLevel of Evidence 3andamar0290No ratings yet
- Pathogenesis of Acute Rheumatic Fever (ARF) : DR - Modni AbdulmajeedDocument5 pagesPathogenesis of Acute Rheumatic Fever (ARF) : DR - Modni AbdulmajeedJana AliNo ratings yet
- Rheumatic Fever Small Group DiscussionDocument13 pagesRheumatic Fever Small Group DiscussionLyca Mae AurelioNo ratings yet
- Systemic Inflammatory Response Syndrome (SIRS) & Sepsis: Dr.H.Asril Zahari SP.B.KBDDocument43 pagesSystemic Inflammatory Response Syndrome (SIRS) & Sepsis: Dr.H.Asril Zahari SP.B.KBDPark ji SangNo ratings yet
- Tropical Med Int Health - 2007 - Gulati - Atypical Manifestations of DengueDocument9 pagesTropical Med Int Health - 2007 - Gulati - Atypical Manifestations of DenguekosalNo ratings yet
- Daftar Pustaka Emedicine MedscapeDocument7 pagesDaftar Pustaka Emedicine MedscapeAyesha Nabilla Putri0% (1)
- Nursing AssessmentDocument4 pagesNursing AssessmentFlor SabaysabayNo ratings yet
- A Chilly FeverDocument5 pagesA Chilly FeverChangNo ratings yet
- Histoplasmosis: Histoplasma CapsulatumDocument19 pagesHistoplasmosis: Histoplasma CapsulatumKathzkaMaeAgcaoiliNo ratings yet
- Vector-Borne Disease LouseDocument37 pagesVector-Borne Disease LouseSohail AhmedNo ratings yet
- Approach To The Febrile Patient: Dr.P.V.Balamurugan, M.D Senior Assistant Professor Dept. of Medicine GTMCH, TheniDocument85 pagesApproach To The Febrile Patient: Dr.P.V.Balamurugan, M.D Senior Assistant Professor Dept. of Medicine GTMCH, TheniAlp HatNo ratings yet
- A Review On Dengue and Treatments 13 23Document3 pagesA Review On Dengue and Treatments 13 23Karina Mega WNo ratings yet
- Lapsus Tifoid + DengueDocument10 pagesLapsus Tifoid + DengueM.ThaufiqurrakhmanNo ratings yet
- Mycobacteria Tuberculosis: Mycobacterium Tuberculosis Is The Primary Bacterium Responsible For CausingDocument4 pagesMycobacteria Tuberculosis: Mycobacterium Tuberculosis Is The Primary Bacterium Responsible For CausingGregorio ValllejoNo ratings yet
- Rheumatic Fever & RHDDocument13 pagesRheumatic Fever & RHDValerrie NgenoNo ratings yet
- Fever of Unknown OriginDocument6 pagesFever of Unknown OriginJyothsna S MandarapuNo ratings yet
- Septic Shock: by Nsubuga Ivan BMS/12264/182/DU 4.2Document55 pagesSeptic Shock: by Nsubuga Ivan BMS/12264/182/DU 4.2Nsubuga IvanNo ratings yet
- CT and MR Imaging Findings Associated With Subacute ThyroiditisDocument9 pagesCT and MR Imaging Findings Associated With Subacute ThyroiditisMoh SuriyawalNo ratings yet
- AnaplasmosisDocument1 pageAnaplasmosisfredyNo ratings yet
- Leptospirosis: A Case Study: Mathew SullivanDocument3 pagesLeptospirosis: A Case Study: Mathew SullivanSagara MaheshNo ratings yet
- J Infect Dis. 2005 Radolf 948 9Document2 pagesJ Infect Dis. 2005 Radolf 948 9Diego BenavidesNo ratings yet
- FuoDocument4 pagesFuoDevi Eliani ChandraNo ratings yet
- Dave ILOs (Example)Document7 pagesDave ILOs (Example)Suraj MadeshiyaNo ratings yet
- Acute Bacterial ParotitisDocument3 pagesAcute Bacterial ParotitisPatrick JimenezNo ratings yet
- Soldiers From Indo Myanmar Border Presenting With Scrub Typhus: Case ReportDocument5 pagesSoldiers From Indo Myanmar Border Presenting With Scrub Typhus: Case ReportIOSRjournalNo ratings yet
- 278 977 1 SMDocument2 pages278 977 1 SMMohamed MukhrizNo ratings yet
- Fever of Unknown Origin (Fuo) : DR Budi Enoch SPPDDocument23 pagesFever of Unknown Origin (Fuo) : DR Budi Enoch SPPDRoby KieranNo ratings yet
- Pulmonary Tuberculosis Presenting With Acute Respiratory Distress Syndrome (ARDS) : A Case Report and Review of LiteratureDocument5 pagesPulmonary Tuberculosis Presenting With Acute Respiratory Distress Syndrome (ARDS) : A Case Report and Review of LiteratureCimol AgustinaNo ratings yet
- Review Article: Etiology and Risk Factors of Febrile Seizure - An UpdateDocument10 pagesReview Article: Etiology and Risk Factors of Febrile Seizure - An UpdateResty Rahmiliah RahimNo ratings yet
- Acute Rheumatic FeverDocument5 pagesAcute Rheumatic FeverSyahmi AhmadNo ratings yet
- Chronic Urticaria Clinical Presentation - History, Physical Examination, ComplicationsDocument5 pagesChronic Urticaria Clinical Presentation - History, Physical Examination, ComplicationsOgy SkillNo ratings yet
- Amjad Bani Hani: Sir S, Sep S Is, A N D ModsDocument67 pagesAmjad Bani Hani: Sir S, Sep S Is, A N D ModsRuffaeelJabrNo ratings yet
- 1663503021Document23 pages1663503021lovekohli235No ratings yet
- Infectious Diseases For InternsDocument60 pagesInfectious Diseases For InternsMaya SwariNo ratings yet
- Dengue Hemorrhagic Fever With Special Emphasis On ImmunopathogenesisDocument12 pagesDengue Hemorrhagic Fever With Special Emphasis On ImmunopathogenesisHadley AuliaNo ratings yet
- Infection: Dr. Mehrunnisa Umar Assistant Professor Department of MedicineDocument57 pagesInfection: Dr. Mehrunnisa Umar Assistant Professor Department of MedicinedrusmanjamilhcmdNo ratings yet
- Case Report: Fatal Staphylococcal Infection Following Classic Dengue FeverDocument4 pagesCase Report: Fatal Staphylococcal Infection Following Classic Dengue FeverRia Septi HarmiaNo ratings yet
- Dengue Hemorrhagic FeverDocument15 pagesDengue Hemorrhagic FeverAcca Malik MuhammadNo ratings yet
- SarcoidosisDocument22 pagesSarcoidosisveerraju tvNo ratings yet
- Rheumatic FeverDocument13 pagesRheumatic Feverpaulkimunya100No ratings yet
- Scarlet Fever - Background, Pathophysiology, EtiologyDocument8 pagesScarlet Fever - Background, Pathophysiology, EtiologyPaskalia ChristinNo ratings yet
- Clinical Manifestations, Etiology, and Pathogenesis of The Hyper-Ige SyndromesDocument6 pagesClinical Manifestations, Etiology, and Pathogenesis of The Hyper-Ige SyndromesPauline CabreraNo ratings yet
- Grunewald 2019Document22 pagesGrunewald 2019Josver PretellNo ratings yet
- Evaluation of The Febrile Patient A Case-Based Approach: Fevers and Fevers of Unknown OriginDocument97 pagesEvaluation of The Febrile Patient A Case-Based Approach: Fevers and Fevers of Unknown Originkrish vjNo ratings yet
- Fever of Unknown Origin 2024Document14 pagesFever of Unknown Origin 2024Veronica Romero MouthonNo ratings yet
- Tugas DR Rizal: Medical Equipment Made Easy To Understand ...Document73 pagesTugas DR Rizal: Medical Equipment Made Easy To Understand ...Beuty SavitriNo ratings yet
- Association of Interleukin-1 Polymorphisms With Periodontitis in Down SyndromeDocument10 pagesAssociation of Interleukin-1 Polymorphisms With Periodontitis in Down SyndromeBeuty SavitriNo ratings yet
- Archive of SIDDocument6 pagesArchive of SIDBeuty SavitriNo ratings yet
- Management of Respiratory Arrest Bag-Mask Ventilation Testing ChecklistDocument1 pageManagement of Respiratory Arrest Bag-Mask Ventilation Testing ChecklistBeuty SavitriNo ratings yet
- 33 Varan Alel CYP2A6Document15 pages33 Varan Alel CYP2A6Beuty SavitriNo ratings yet
- 13 Male InfertilityDocument13 pages13 Male InfertilityBeuty SavitriNo ratings yet
- Facts About Atrial Septal DefectDocument3 pagesFacts About Atrial Septal DefectBeuty SavitriNo ratings yet
- Impetigo in Children: A Clinical Guide and Treatment OptionsDocument2 pagesImpetigo in Children: A Clinical Guide and Treatment OptionsBeuty SavitriNo ratings yet
- Bile Peritonitis 2021Document6 pagesBile Peritonitis 2021Brvo CruzNo ratings yet
- Normal Puerperium & PostnatalDocument38 pagesNormal Puerperium & PostnatalBernice GyapongNo ratings yet
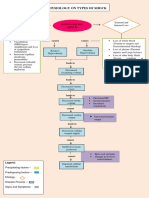
- Pathophysiology On Types of ShockDocument4 pagesPathophysiology On Types of ShockJessa Mae Alforque AsentistaNo ratings yet
- DR Franciscus Ginting - Sepsis PIN PAPDI Surabaya WS-051019-DikonversiDocument82 pagesDR Franciscus Ginting - Sepsis PIN PAPDI Surabaya WS-051019-DikonversiDea LudjenNo ratings yet
- Aaa Ayush Patel (Shock)Document53 pagesAaa Ayush Patel (Shock)Ayush PatelNo ratings yet
- Nutrition Support in Critically Ill PatientDocument19 pagesNutrition Support in Critically Ill PatienttantoNo ratings yet
- (Ebook PDF) Textbook of Critical Care 7th Edition Jean-Louis Vincent - Ebook PDF All ChapterDocument69 pages(Ebook PDF) Textbook of Critical Care 7th Edition Jean-Louis Vincent - Ebook PDF All Chapterdryndalifasi100% (11)
- BPMN Modeler - Demo - Bpmn.ioDocument9 pagesBPMN Modeler - Demo - Bpmn.ioJHON FREDY CASTAÑEDA LOPEZNo ratings yet
- Sepsis 2021 A ReviewDocument9 pagesSepsis 2021 A ReviewvictorNo ratings yet
- Short Answer Questions AnaesthesiaDocument91 pagesShort Answer Questions AnaesthesiaMeena Ct100% (12)
- Antimicrobial Agents and Chemotherapy-2010-Pea-4605.fullDocument6 pagesAntimicrobial Agents and Chemotherapy-2010-Pea-4605.fullGül BaktırNo ratings yet
- Infections AntibioticsDocument4 pagesInfections AntibioticsMatthieu FortinNo ratings yet
- UrosepsisDocument6 pagesUrosepsisParama AdhikresnaNo ratings yet
- Crystalloid Fluid Choice and Clinical Outcomes in Pediatric Sepsis J Peds 2017 PDFDocument17 pagesCrystalloid Fluid Choice and Clinical Outcomes in Pediatric Sepsis J Peds 2017 PDFYan Hein TanawaniNo ratings yet
- Pharmacotherapeutics-II Question Bank 3rd Pharm DDocument11 pagesPharmacotherapeutics-II Question Bank 3rd Pharm DAnanda Vijayasarathy100% (3)
- Approach To The Patient With Fever EditedDocument72 pagesApproach To The Patient With Fever EditedKevin Karim100% (1)
- Nueva Ecija University of Science And: A Case Analysis of Acute Conditions of The NeonatesDocument68 pagesNueva Ecija University of Science And: A Case Analysis of Acute Conditions of The NeonatesShane PangilinanNo ratings yet
- Handbook July 2016 - Formatted v3Document172 pagesHandbook July 2016 - Formatted v3ElaineNo ratings yet
- Sepsis: Dr. Cristhian Huanca Panozo Medicina InternaDocument25 pagesSepsis: Dr. Cristhian Huanca Panozo Medicina InternafranciNo ratings yet
- Estate of Jeffrey Scott Lillis v. Correct Care Solutions LLC, Et. Al.Document42 pagesEstate of Jeffrey Scott Lillis v. Correct Care Solutions LLC, Et. Al.Michael_Lee_RobertsNo ratings yet
- Shock - Classification and Pathophysiological Principles of TherapeuticsDocument12 pagesShock - Classification and Pathophysiological Principles of TherapeuticsLuis ChancusigNo ratings yet
- Lecture-18 Obstructed LaborDocument8 pagesLecture-18 Obstructed LaborMadhu Sudhan PandeyaNo ratings yet
- Module 3 A PresentationDocument79 pagesModule 3 A PresentationMelinda FiskaNo ratings yet
- Acca Cs Syok SepsisDocument1 pageAcca Cs Syok SepsisSamuel KalonkNo ratings yet
- Utilidad Del Lactato Sérico Elevado Como Factor Pronóstico de Muerte en Sepsis SeveraDocument6 pagesUtilidad Del Lactato Sérico Elevado Como Factor Pronóstico de Muerte en Sepsis SeveraManuelito ZeNo ratings yet
- J Chest 2017 08 022Document30 pagesJ Chest 2017 08 022malvindersahiNo ratings yet
- Silver-Coated Dressing Acticoat Caused Raised LiverDocument5 pagesSilver-Coated Dressing Acticoat Caused Raised LiverJorgeNo ratings yet