Download as docx, pdf, or txt
You might also like
- BCJ582 Final Exam 100% Correct AnswersDocument49 pagesBCJ582 Final Exam 100% Correct AnswersHomeworkhelpbylance0% (3)
- Françoise Dolto and Child PsychoanalysisDocument130 pagesFrançoise Dolto and Child PsychoanalysisDr. Peter Fritz Walter100% (4)
- ADHD Screening Test PDFDocument20 pagesADHD Screening Test PDFdcowan94% (17)
- Photodermatology MCQsDocument53 pagesPhotodermatology MCQsDr.Tawheed100% (8)
- The Beginning Human LifeDocument1 pageThe Beginning Human LifeDon SumiogNo ratings yet
- Problem With The PassageDocument3 pagesProblem With The PassageLuiciaNo ratings yet
- Muscle Stretching in Manual Therapy I - The Extremities (Team Nanban) (TPB)Document177 pagesMuscle Stretching in Manual Therapy I - The Extremities (Team Nanban) (TPB)CNPOULIS100% (22)
- Stage Fright Pranic HealingDocument5 pagesStage Fright Pranic HealingHitesh Parmar100% (1)
- Inner Work Is The Hero's Journey Mythic Interpretations of Holotropic Breathwork Archambault DissertationDocument226 pagesInner Work Is The Hero's Journey Mythic Interpretations of Holotropic Breathwork Archambault DissertationAntonio VaszkenNo ratings yet
- B.Barnes - Thyroid GlandDocument8 pagesB.Barnes - Thyroid GlandoptinNo ratings yet
- Nur 332 Ebp PosterDocument1 pageNur 332 Ebp Posterapi-419091662No ratings yet
- Attachment TheoryDocument40 pagesAttachment Theorycristeacristina2007100% (9)
- Bioethics ArtificialDocument17 pagesBioethics ArtificialJannica Mae D SacristiaNo ratings yet
- Midterm Exam McaDocument7 pagesMidterm Exam McaBeverly DatuNo ratings yet
- Post Cs Na Revised Na TohDocument31 pagesPost Cs Na Revised Na TohMinerva CortalNo ratings yet
- AnencephalyDocument10 pagesAnencephalyRm LavariasNo ratings yet
- Or Write Up (Appendectomy) : Pines City Colleges College of NursingDocument9 pagesOr Write Up (Appendectomy) : Pines City Colleges College of Nursingthomasfinley44No ratings yet
- Bone Marrow Transplant: Submitted To: Dr. Karanjot Singh Submitted By: Jasmeen KaurDocument58 pagesBone Marrow Transplant: Submitted To: Dr. Karanjot Singh Submitted By: Jasmeen KaurMani RaoNo ratings yet
- NCP Risk For Infection Related To Postop IncisionDocument1 pageNCP Risk For Infection Related To Postop IncisionCharry de VeraNo ratings yet
- Upper Respiratory Tract InfectionDocument12 pagesUpper Respiratory Tract InfectionErmie BalingitNo ratings yet
- Rafols, Janna Mae L. 3F-2C OR QuestionsDocument8 pagesRafols, Janna Mae L. 3F-2C OR QuestionsJan Crizza Dale R. FrancoNo ratings yet
- Bea-Case StudyDocument21 pagesBea-Case Studybea pegadNo ratings yet
- Cord ProlapseDocument22 pagesCord ProlapseJoyjet Evangelista-murilloNo ratings yet
- 8th Quiz URINARY SYSTEM (Quiz)Document1 page8th Quiz URINARY SYSTEM (Quiz)Jobelle VergaraNo ratings yet
- Post-Partum Hemorrhage Pathophysiology PaperDocument5 pagesPost-Partum Hemorrhage Pathophysiology Paperapi-399619969No ratings yet
- First Stage: Stages of Labor Start End Duration Nullipara MultiparaDocument4 pagesFirst Stage: Stages of Labor Start End Duration Nullipara MultiparaElleNo ratings yet
- 1.3 Issues On Artificial ReproductionDocument46 pages1.3 Issues On Artificial ReproductionKeana DacayanaNo ratings yet
- Foreign Body Airway ObstructionDocument15 pagesForeign Body Airway ObstructionKristine Anne SorianoNo ratings yet
- Bioethics: Bachelor of Science in NursingDocument6 pagesBioethics: Bachelor of Science in NursingSherinne Jane Cariazo0% (1)
- Malaria PosterDocument1 pageMalaria PosterTommaso ForzaNo ratings yet
- Beliefs and PracticesDocument10 pagesBeliefs and PracticesGeorge Aquino CondeNo ratings yet
- Postpartum: Competency Appraisal - OBDocument54 pagesPostpartum: Competency Appraisal - OBkimalli92No ratings yet
- Discharge PlanDocument4 pagesDischarge PlanPaul Loujin LeeNo ratings yet
- Chapter 31 MalnutritionDocument7 pagesChapter 31 MalnutritionNeil Dave SuarezNo ratings yet
- Obgyn Abbreviations For RotationDocument2 pagesObgyn Abbreviations For RotationBigBoostingNo ratings yet
- NCM 110A Module 2 Advanced Hardware and MhealthDocument9 pagesNCM 110A Module 2 Advanced Hardware and MhealthKi PieNo ratings yet
- Pre Gestational GestationalDocument19 pagesPre Gestational GestationalRoger Jr PumarenNo ratings yet
- NCP TemplateDocument1 pageNCP TemplateAngelo GarinoNo ratings yet
- Case Study CSDocument21 pagesCase Study CSThessa Lonica GarciaNo ratings yet
- Bubbles HeDocument39 pagesBubbles HePerrilyn PereyNo ratings yet
- Module 12 ContempoDocument5 pagesModule 12 ContempoJericho CunananNo ratings yet
- Normal Delivery Checklist 2020Document4 pagesNormal Delivery Checklist 2020Ever Seneca EscaLeraNo ratings yet
- Chapter 44-Activity and ExerciseDocument4 pagesChapter 44-Activity and ExerciseollietonkNo ratings yet
- Case Study AGE With Signs of DehydrationDocument27 pagesCase Study AGE With Signs of DehydrationZhenmeiNo ratings yet
- Case PresDocument100 pagesCase PresJoj BagnateNo ratings yet
- Gestational Thropoblastic DiseaseDocument56 pagesGestational Thropoblastic DiseaseGringo Barroga0% (1)
- Community Health NursingDocument105 pagesCommunity Health NursingKBDNo ratings yet
- 01 Chapter Anti InfectiveDocument90 pages01 Chapter Anti InfectiveMSKCNo ratings yet
- NCM 109 MCN Finals Topic 1 Problems With The PassengerDocument3 pagesNCM 109 MCN Finals Topic 1 Problems With The PassengerQUEZON, BRITNEY KIM E.No ratings yet
- Reflection PaperDocument2 pagesReflection PapershanoiapowelllNo ratings yet
- Patient Positioning: Complete Guide For Nurses: Marjo S. Malabanan, R.N.,M.NDocument43 pagesPatient Positioning: Complete Guide For Nurses: Marjo S. Malabanan, R.N.,M.NMercy Anne EcatNo ratings yet
- Uremic EncephalophatyDocument48 pagesUremic EncephalophatySindi LadayaNo ratings yet
- Pilitter 2Document2 pagesPilitter 2Jenny VilleNo ratings yet
- Test Questions CA1Document3 pagesTest Questions CA1Gemery Jade ArtatesNo ratings yet
- EuthanasiaDocument4 pagesEuthanasiaDip PerNo ratings yet
- HERNIORRHAPHYDocument2 pagesHERNIORRHAPHYSheldon Deypalubos Jr.No ratings yet
- Procedure-Assessing Fetal Heart ToneDocument1 pageProcedure-Assessing Fetal Heart ToneCyril Joy N. FernandoNo ratings yet
- Case Study UrtiDocument9 pagesCase Study UrtiHomework PingNo ratings yet
- Assessing Breast and AxillaeDocument23 pagesAssessing Breast and AxillaeGemmalene PaclebNo ratings yet
- SWADDLINGDocument4 pagesSWADDLINGksjsellsNo ratings yet
- 3.3 Integrated Management of Childhood Illness PDFDocument11 pages3.3 Integrated Management of Childhood Illness PDFVernonDimalNo ratings yet
- Giger and DavidhizarDocument4 pagesGiger and DavidhizarHv EstokNo ratings yet
- Metabolic EmergenciesDocument53 pagesMetabolic EmergenciesWengel Redkiss100% (1)
- Nursing Care Plan General Objective: To Promote Safety Through Prevention of The Spread of InfectionDocument3 pagesNursing Care Plan General Objective: To Promote Safety Through Prevention of The Spread of InfectionitsmeayaNo ratings yet
- Pediatric Community Acquired Pneumonia - Moderate Risk: University of The Cordilleras College of NursingDocument22 pagesPediatric Community Acquired Pneumonia - Moderate Risk: University of The Cordilleras College of NursingJemimah AdaclogNo ratings yet
- Discharge Plan 3Document3 pagesDischarge Plan 3minjungNo ratings yet
- Ectopic PregnancyDocument65 pagesEctopic PregnancyWen SilverNo ratings yet
- Module 2 Proliferative Growth Patterns Etiology Role of The Immune SystemDocument69 pagesModule 2 Proliferative Growth Patterns Etiology Role of The Immune SystemAlessandra MercadoNo ratings yet
- Normal Pediatric Milestones PDFDocument1 pageNormal Pediatric Milestones PDFShara SampangNo ratings yet
- Normal Pediatric Milestones PDFDocument1 pageNormal Pediatric Milestones PDFShara SampangNo ratings yet
- Newborn Reflexes PDFDocument1 pageNewborn Reflexes PDFShara Sampang0% (1)
- Safari - 18 Jul 2018 at 1:43 PMDocument1 pageSafari - 18 Jul 2018 at 1:43 PMShara SampangNo ratings yet
- Respiratory Modalities PPT - KateDocument80 pagesRespiratory Modalities PPT - KateShara SampangNo ratings yet
- Postmodern PhilosophyDocument13 pagesPostmodern PhilosophyShara SampangNo ratings yet
- Acute. KetoacidosisdocxDocument12 pagesAcute. KetoacidosisdocxShara SampangNo ratings yet
- Nursing Associations in The PhilippinesDocument10 pagesNursing Associations in The PhilippinesShara SampangNo ratings yet
- Traumatic Brain InJuryDocument21 pagesTraumatic Brain InJuryShara SampangNo ratings yet
- Future Trends and Issues in Mental Health Nursing PracticeDocument17 pagesFuture Trends and Issues in Mental Health Nursing PracticeShara Sampang100% (4)
- Problem Identification ToolsDocument23 pagesProblem Identification ToolsShara SampangNo ratings yet
- Legal Issues Affecting Mental Health NursingDocument14 pagesLegal Issues Affecting Mental Health NursingShara Sampang0% (1)
- Diabetesa 1223313005812508 8Document82 pagesDiabetesa 1223313005812508 8Shara SampangNo ratings yet
- Evaluation and FHSISDocument6 pagesEvaluation and FHSISShara SampangNo ratings yet
- Mental Health Psychiatric Nursing PracticeDocument14 pagesMental Health Psychiatric Nursing PracticeShara SampangNo ratings yet
- Problem Identification ToolsDocument23 pagesProblem Identification ToolsShara SampangNo ratings yet
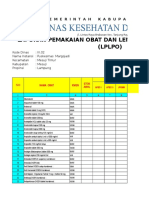
- LPLPO PuskesmasDocument16 pagesLPLPO Puskesmashastin fitriacahyaniNo ratings yet
- 1000111774Document909 pages1000111774juancmuNo ratings yet
- Sirsasana Father of All AsanasDocument2 pagesSirsasana Father of All AsanasHaseebNo ratings yet
- Impaired Skin IntegDocument2 pagesImpaired Skin IntegMarcus Philip GonzalesNo ratings yet
- Efficacy of Latanoprostene Bunod 0.024% Compared With Timolol 0.5% in Lowering Intraocular Pressure Over 24 HoursDocument9 pagesEfficacy of Latanoprostene Bunod 0.024% Compared With Timolol 0.5% in Lowering Intraocular Pressure Over 24 HoursAnnisa AuliaNo ratings yet
- Management of Tooth Surface Loss (By Bruxism)Document11 pagesManagement of Tooth Surface Loss (By Bruxism)yuuudiiiNo ratings yet
- Effect of Transcutaneous Electrical Nerve Stimulation On Spasticity in Adults With Stroke A Syst Review and Metaanalysis PDFDocument18 pagesEffect of Transcutaneous Electrical Nerve Stimulation On Spasticity in Adults With Stroke A Syst Review and Metaanalysis PDFjaunasvyras69 Jaunasvyras69No ratings yet
- Caring For Older PeopleDocument57 pagesCaring For Older PeopleOsama Elsayed AhmedNo ratings yet
- Prognosis SampleDocument3 pagesPrognosis SampleCJ GambaNo ratings yet
- Down SyndromeDocument18 pagesDown SyndromeBlake BoggenpoelNo ratings yet
- ARDS Berlin Definition - JAMADocument8 pagesARDS Berlin Definition - JAMAaji_jati_2005No ratings yet
- Angelo Karam Career TestDocument2 pagesAngelo Karam Career Testapi-248094656No ratings yet
- Psychoanalysis Class Assignment Group SettingDocument7 pagesPsychoanalysis Class Assignment Group Settingapi-251996923No ratings yet
- Hypnosis 2Document17 pagesHypnosis 2safia100% (2)
- Jurnal 2Document10 pagesJurnal 2adi suciptoNo ratings yet
- Canadian PharmaciestDocument1 pageCanadian PharmaciestzevlesiukasNo ratings yet
- 001 What Is Thai Massage (FreeCourseWeb - Com)Document6 pages001 What Is Thai Massage (FreeCourseWeb - Com)Victor FernandesNo ratings yet
- Equipment Replacement Intervals PDFDocument6 pagesEquipment Replacement Intervals PDFKevin MicoltaNo ratings yet
- BROMOCRIPTINE in Patients With Attention Deficit Hyperactive DisorderDocument46 pagesBROMOCRIPTINE in Patients With Attention Deficit Hyperactive DisorderOlayinka Awofodu100% (1)
- Reiki 3Document281 pagesReiki 3Akfaini MarfirdausNo ratings yet