Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Romantic AgonyDocument521 pagesThe Romantic Agonyinanna12100% (3)
- PlayingByTheRules Apexart PDFDocument178 pagesPlayingByTheRules Apexart PDFinanna12No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Latin American Art of The 20th Century by Edward Lucie-SmithDocument220 pagesLatin American Art of The 20th Century by Edward Lucie-Smithinanna12100% (1)
- Twopri00weis PDFDocument876 pagesTwopri00weis PDFinanna1250% (2)
- The Pillow BookDocument284 pagesThe Pillow Bookinanna12100% (2)
- Animal Myth and Magic: Images From Pre-Columbian TextilesDocument168 pagesAnimal Myth and Magic: Images From Pre-Columbian Textilesinanna12100% (1)
- Brand Henrik Ibsen (Ebooksread - Com) PDFDocument248 pagesBrand Henrik Ibsen (Ebooksread - Com) PDFinanna120% (1)
- Iracmahoneylip00alenuoft PDFDocument268 pagesIracmahoneylip00alenuoft PDFinanna12No ratings yet
- Guided Self Help AnxietyDocument9 pagesGuided Self Help Anxietyinanna12No ratings yet
- Social Science Computer Review: Internet Abuse: Addiction? Disorder? Symptom? Alternative Explanations?Document11 pagesSocial Science Computer Review: Internet Abuse: Addiction? Disorder? Symptom? Alternative Explanations?inanna12100% (1)
- Digital Education ElearningDocument5 pagesDigital Education Elearninginanna12No ratings yet
- MODULE4Document38 pagesMODULE4Caryl SequitinNo ratings yet
- DCMSTIS-Senior Citizen Action Plan FY2022Document2 pagesDCMSTIS-Senior Citizen Action Plan FY2022Zoe GALLARDO33% (3)
- Wins Action PlanDocument3 pagesWins Action PlanCHRISTINE GASPACHO100% (1)
- Malariafinalthesis PDFDocument67 pagesMalariafinalthesis PDFVitalis MbuyaNo ratings yet
- Bell's Palsy - Symptoms and Causes - Mayo ClinicDocument6 pagesBell's Palsy - Symptoms and Causes - Mayo ClinicRoxan PacsayNo ratings yet
- 01f2 - ICD vs. DSM - APA PDFDocument1 page01f2 - ICD vs. DSM - APA PDFfuturistzgNo ratings yet
- A Review of Classification of Disease in AyurvedaDocument11 pagesA Review of Classification of Disease in AyurvedaEditor_IAIMNo ratings yet
- Megan Fish: 2781 Holman Drive Erie, PA 16509 (814) 460-9473Document2 pagesMegan Fish: 2781 Holman Drive Erie, PA 16509 (814) 460-9473MeganNo ratings yet
- Spinal Cord Injury Rehabilitation Webinar 2020 PDFDocument2 pagesSpinal Cord Injury Rehabilitation Webinar 2020 PDFGirijashankar KhuntiaNo ratings yet
- The in Uence of Impaction To The Third Molar Mineralization in Northwestern Chinese PopulationDocument8 pagesThe in Uence of Impaction To The Third Molar Mineralization in Northwestern Chinese PopulationIvan GalicNo ratings yet
- Modern and Classic Wound Dressing Comparison in WoDocument6 pagesModern and Classic Wound Dressing Comparison in WoJuan LuckyNo ratings yet
- Anesthesia Guide VASG 12-4-04Document164 pagesAnesthesia Guide VASG 12-4-04Radu TudorNo ratings yet
- Covid-19 and The Former Spanish Flu: PrevalenceDocument9 pagesCovid-19 and The Former Spanish Flu: PrevalenceAailaa SagharNo ratings yet
- A Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeDocument10 pagesA Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeInnani Wildania HusnaNo ratings yet
- Cot Demo Health 6-Guro21 - 3q - March 16 2023Document5 pagesCot Demo Health 6-Guro21 - 3q - March 16 2023Diego MapulaNo ratings yet
- OB NotesDocument2 pagesOB NotesJudy Ann CristeNo ratings yet
- Faris Akbar Ashari 30101407181Document25 pagesFaris Akbar Ashari 30101407181Fariseilaa PurakbarNo ratings yet
- Musculoskeletal Ultrasound Imaging Training, Use, and KnowledgeDocument10 pagesMusculoskeletal Ultrasound Imaging Training, Use, and KnowledgeChristian F. VegaNo ratings yet
- The Importance of Good PostureDocument1 pageThe Importance of Good Postureerica thapaNo ratings yet
- LipCancer BrachyDocument10 pagesLipCancer Brachyarungoel2No ratings yet
- AmputationDocument51 pagesAmputationStar CruiseNo ratings yet
- Skills Checklist Blood AdminDocument3 pagesSkills Checklist Blood AdmingtsantosNo ratings yet
- CHN Week 1 Day 2 and 3 Activity Initial Data BaseDocument6 pagesCHN Week 1 Day 2 and 3 Activity Initial Data BaseGailNo ratings yet
- Diabetic Foot Care Before and During The COVID-19 Epidemic: What Really Matters?Document2 pagesDiabetic Foot Care Before and During The COVID-19 Epidemic: What Really Matters?SitiNo ratings yet
- Medical Safety Clinical Reviewer in Chicago IL Resume Rachel DohrDocument3 pagesMedical Safety Clinical Reviewer in Chicago IL Resume Rachel DohrRachelDohr2No ratings yet
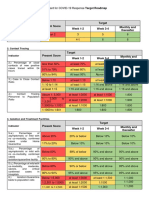
- Present Score Target Week 1-2 Week 3-4 Monthly and ThereafterDocument2 pagesPresent Score Target Week 1-2 Week 3-4 Monthly and ThereafterFret Ramirez Coronia RNNo ratings yet
- Reviewer Grade 12 Physical EducationDocument3 pagesReviewer Grade 12 Physical EducationKervin PlatonNo ratings yet
- Epirubicin: The Following Side Effects Are Common (Occurring in Greater Than 30%) For Patients Taking EpirubicinDocument5 pagesEpirubicin: The Following Side Effects Are Common (Occurring in Greater Than 30%) For Patients Taking EpirubicinSteffi EllaNo ratings yet
- DMMMSU-RETC-F013-Application For Ethics Review of A New ProtocolDocument4 pagesDMMMSU-RETC-F013-Application For Ethics Review of A New ProtocoluzamarknielconNo ratings yet
- Jospt 2009 2857Document11 pagesJospt 2009 2857Novy DitaNo ratings yet