Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Paul E. Steiner - Okinawa and Its People (I)Document10 pagesPaul E. Steiner - Okinawa and Its People (I)José Luis IgueNo ratings yet
- The American College of Radiology BI-RADS Atlas 5 Edition: Frequently Asked QuestionsDocument18 pagesThe American College of Radiology BI-RADS Atlas 5 Edition: Frequently Asked QuestionssatanioNo ratings yet
- Aspartame Side EffectsDocument3 pagesAspartame Side Effectsnettie95No ratings yet
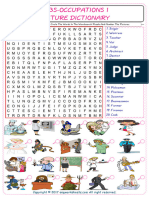
- Jobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Document2 pagesJobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Raquel NoeliaNo ratings yet
- Imogen Edwards-Jones, The Woman Behind Hotel Babylon, Is Training Her Sights On The Unlikeliest of Targets: The NHSDocument3 pagesImogen Edwards-Jones, The Woman Behind Hotel Babylon, Is Training Her Sights On The Unlikeliest of Targets: The NHSinfo7462100% (1)
- Food Microbiology, AASTUDocument119 pagesFood Microbiology, AASTUmikialeNo ratings yet
- Slender Quest DetailsDocument1 pageSlender Quest Detailsparents021No ratings yet
- The HearthDocument1 pageThe HearthRaffaela CerroneNo ratings yet
- Quiz Section: Level 1Document4 pagesQuiz Section: Level 1AinunZamiraNo ratings yet
- Manual Book Isuzu Panther PDFDocument23 pagesManual Book Isuzu Panther PDFZidna IlmaNo ratings yet
- Chemical Constituents From The Stems Of: Celastrus OrbiculatusDocument5 pagesChemical Constituents From The Stems Of: Celastrus OrbiculatusTuan PhamquocNo ratings yet
- Critical Care EnvironmentDocument16 pagesCritical Care EnvironmentJeffrey KauvaNo ratings yet
- Brain Heart Infusion Broth - MerckDocument3 pagesBrain Heart Infusion Broth - MerckMitha Arianti100% (1)
- ASHP Guidelines On Compounding Sterile PreparationsDocument22 pagesASHP Guidelines On Compounding Sterile PreparationsHeru NugrohoNo ratings yet
- Wulandari Ramadiyani 22010111110083 Lap - KTI Bab8 PDFDocument17 pagesWulandari Ramadiyani 22010111110083 Lap - KTI Bab8 PDFZorofan Roronoa AzNo ratings yet
- Immunology Exam 4 Study GuideDocument2 pagesImmunology Exam 4 Study GuideKeaton EisenmengerNo ratings yet
- MDocument86 pagesMeheidariNo ratings yet
- Code BlueDocument18 pagesCode Blueandri100% (1)
- Cervical Vertigo PDFDocument5 pagesCervical Vertigo PDFPaijo SusenoNo ratings yet
- Wa0022 PDFDocument9 pagesWa0022 PDFAtul BajpaiNo ratings yet
- Stephen's Story: A 19 Year Old'S Life Lessons OnDocument16 pagesStephen's Story: A 19 Year Old'S Life Lessons OnSylvia DobsonNo ratings yet
- Eye and Vision 7th EditionDocument35 pagesEye and Vision 7th EditionCrystal LynaeNo ratings yet
- Eng PDFDocument45 pagesEng PDFKartika NINo ratings yet
- WPI PharmaceuticalsDocument23 pagesWPI PharmaceuticalsKyle Millar-CorlissNo ratings yet
- NCM 200 - Preparing Administering MedicationDocument21 pagesNCM 200 - Preparing Administering MedicationjhonmarcNo ratings yet
- Joint Commision RegulationsDocument12 pagesJoint Commision Regulationsapi-223525467No ratings yet
- SPJIMR PGDM Operations, IM, Marketing and Finance Tracker 2017-2019Document11 pagesSPJIMR PGDM Operations, IM, Marketing and Finance Tracker 2017-2019Shiv PraNo ratings yet
- Psych Unit I Part 1Document42 pagesPsych Unit I Part 1api-293070066No ratings yet
- Harm Reduction Strategy PDFDocument184 pagesHarm Reduction Strategy PDFArjumand AdilNo ratings yet
- Iceman TattoosDocument3 pagesIceman TattoosfuturearunaNo ratings yet